
Abstract
BACKGROUND:
Transient tachypnea of the newborn(TTNB) is the most common respiratory morbidity in late preterm and term babies and is pathophysiologically related to delayed lung fluid clearance after birth. Mimicking low physiological fluid intake in the initial period of life may accelerate the recovery from TTNB. In a randomized controlled trial, we compared the roles of restricted versus standard fluid management in babies with TTNB requiring respiratory support.
METHODS:
This parallel group,non-blinded, stratified randomized controlled trial was conducted in a level III neonatal unit of eastern India. Late preterm and term babies with TTNB requiring continuous positive airway pressure (CPAP) were randomly allocated to standard and restricted fluid arms for the first 72 hours (hrs). Primary outcome was CPAP duration.
RESULTS:
In total, 100 babies were enrolled in this study with 50 babies in each arm. CPAP duration was significantly less in the restricted arm (48[42, 54] hrs vs 54[48,72] hrs, p = 0.002). However, no difference was observed in the incidence of CPAP failure between the two arms. In the subgroup analysis, the benefit of reduced CPAP duration persisted in late preterm but not in term infants. However, the effect was not significant in the late preterm babies exposed to antenatal steroid.
CONCLUSION:
This trial demonstrated the safety and effectiveness of restrictive fluid strategy in reducing CPAP duration in late preterm and term babies with TTNB. Late preterm babies, especially those not exposed to antenatal steroid were the most benefitted by this strategy.
Keywords
Introduction
Transient tachypnea of the newborn (TTNB) is the most common cause of respiratory distress in late preterm and term newborns in the immediate neonatal period, with an estimated incidence of 0.5% – 2.8% of all live births [1]. Traditional risk factors for TTNB include premature delivery, caesarean section delivery (without labour),mothers with diabetes, male sex, and asphyxia [2 –4]. Although the condition is self-limited in most babies within 72–96 hours (hrs) of birth, respiratory support other than free flow oxygen, in the form of continuous positive airway pressure (CPAP), non-invasive ventilation (NIV), or heated humidified high flow nasal cannula is often required, particularly in infants requiring fraction of inspired oxygen (FiO2) of >0.4, or with delayed presentation from peripheral health center. Inadequate respiratory support may lead to persistent pulmonary hypertension (PPHN) in babies, resulting in significant morbidity or mortality [5 –7]. Requirement of CPAP or NIV significantly increases the hospital stay, hospital costs, and parental anxiety. Although various treatment options, such as inhaled epinephrine, salbutamol, and diuretics have been attempted in babies with TTNB, none of them has proved to be effective [8 –12]. A recent multicenter study reported that antenatal administration of betamethasone to mothers with late preterm fetus reduces TTNB incidence [13]. In developing countries, including India, the coverage of antenatal steroid is still low [14, 15]. In this scenario, modification of the initial fluid management protocol for babies with TTNB requiring respiratory support should be investigated to reduce the total support duration. This intervention is based on the fact that TTNB pathophysiologically relates to a delayed lung fluid clearance during the transition from in - utero to ex- utero [16, 17]. Thus, mimicking a low physiological fluid intake in the initial period of life after birth may accelerate recovery from the effect of excess lung fluid. A Cochrane review on restricted fluid intake in the initial few weeks of life reported a reduced incidence of patent ductus arteriosus (PDA) and necrotizing enterocolitis (NEC) with a trend towards less chance of bronchopulmonary dysplasia (BPD) without any significant effect on TTNB [18]. On the other hand, a separate Cochrane review on the benefit of fluid restriction in TTNB emphasized the requirement of further randomized controlled trials addressing the issue [19]. Although a study by Stroustrup et al. [20] reported the benefit of a restricted fluid strategy in severe TTNB in terms of reduced CPAP duration, data regarding its benefit in developing countries are scarce. We conducted a randomized controlled trial to compare the roles of restricted fluid and standard fluid in babies with TTNB requiring CPAP in a developing country.
Methods
Study design
This parallel-group, non-blinded, stratified prospective randomized controlled trial was conducted in a level III neonatal unit of eastern India between January 2019 and October 2019. This study was approved by the ethical committee of the institution, and it was registered in the Clinical Trial Registry- India (Trial registration No-CTRI/2019/01/017125).
TTNB was diagnosed as a respiratory distress starting within 6 hrs of life and involving characteristic chest X -ray findings (linear streaking at hilum or fluid in the interlobar fissure) after ruling out other causes of respiratory distresses (congenital pneumonia, meconium aspiration syndrome, respiratory distress syndrome, and surgical causes). As per the unit protocol, babies with TTNB with preductal oxygen saturation (SpO2) of <90% were started on free flow oxygen at 0.5FiO2 and flow of 1L /minute through a nasal cannula. Oxygen concentration was increased by 5% to achieve the target preductal SpO2 of 90%–95%. The Silverman score and SpO2 were monitored, and CPAP was considered if either of the following criteria was satisfied: a) Preductal SpO2 of <90% despite FiO2 of ≥40 %; b) A Silverman score that progressively increased to ≥4 for late preterm and ≥5 for term babies. Bubble or ventilator CPAP was started with an initial setting of 0.5 FiO2 and CPAP of 5 cm of water (H2O). Babies were monitored on an hourly basis. The babies with TTNB who exhibited signs of respiratory failure or hemodynamic instability on admission were intubated directly without a CPAP trial and not included in the study. CPAP was increased by 1 cm of H2O every hour if the Silverman score increased by 1 or more during the observation period. Similarly, FiO2 was increased by 5% to maintain preductal SpO2 between 90% and 95%. For every 10% increase in FiO2, CPAP was increased by 1 cm of H2O even if the Silverman score was not worse. On the other hand, FiO2 was reduced by 5% if preductal SpO2 was >95% over the last 1 hr. If FiO2 could be reduced by10 % and the Silverman score improved by 1 or more, CPAP was reduced by 1 cm of H2O until CPAP was 5 cm of H2O and FiO2 was 0.5. Thereafter, FiO2 was reduced to 30% before reducing CPAP to 4 cm of H2O if the Silverman score improved progressively. CPAP was removed when the Silverman score was 2 or less and preductal SpO2was >95% with FiO2 of ≤0.25 and CPAP of 4 cm of H2O for at least 4 hrs. Babies might require free flow oxygen after CPAP removal, which was provided through a nasal cannula to maintain preductal SpO2 between 90 and 95%.
CPAP failure was defined by any of the following criteria: a) Preductal SpO2 of <90% with FiO2 of ≥70% and CPAP of ≥7 cm of H2O; b) Progressively increasing Silverman score of ≥7 despite the maximum CPAP support; c) Frequent and severe apnea requiring bag mask ventilation; d) PaO2 of <50 mm Hg or PaCO2 of >60 mm Hg; e) Severe metabolic acidosis (arterial base deficit > – 10) or shock. Arterial blood gas was estimated only when deemed necessary by treating physicians. Babies with CPAP failure were intubated as per the study protocol.
Participant flow
Based on the aforementioned study protocol following inclusion and exclusion criteria were established.
Inclusion criteria: Inborn babies born between 34 and 41 6/7 weeks and having a birth weight of >1500 grams, fulfilling the definition of TTNB and requiring CPAP as respiratory support within 6 hrs of life, whose parents provided consent for participation.
Exclusion criteria: Presence of air leak, presence of congenital anomalies, babies with TTNB with respiratory failure or hemodynamic instability requiring intubation and mechanical ventilation on admission to NICU, babies with TTNB requiring only oxygen, requirement of CPAP beyond the first 6 hrs of life, diagnosis of other causes of respiratory distress (meconium aspiration syndrome, respiratory distress syndrome, PPHN, congenital pneumonia, and surgical causes), babies born through meconium stained amniotic fluid, babies suspected of having sepsis on the basis of risk factors or clinical profile, perinatal asphyxia, and presence of shock.
Parents of eligible newborns were approached for consent. Babies of parents providing consent were randomized to the standard arm or restricted arm at the time of CPAP application. Randomization was stratified into late preterm (34–366/7 weeks) and term newborn (37–416/7 weeks)and was performed on the basis of a computer- generated sequence with a 1 : 1 allocation ratio using a block size of 4. An investigator who was not clinically involved in the trial prepared the randomization list. According to the records of last 12 months from the unit, late preterm and term newborns with TTNB required CPAP of 72±12 hrs (mean±standard deviation [SD]). A difference of 8 hrs in respiratory support was considered meaningful between the two arms. With a two sided alpha of 0.05 and power of 80%, 90 babies need to be recruited with 45 babies in each group. Assuming 10% loss due to development of hypoglycemia, over hydration, dehydration, or air leak, 50 babies were recruited in each arm. The nursing staff performed allocation concealment by using the sequentially numbered opaque sealed envelope technique. Sealed envelopes were placed at the nursing station. The corresponding envelope was opened at the time of randomization of babies by the respective nursing staff, and the treating physician was informed. Physicians and nursing staffs were not blinded to the study intervention.
The standard arm received 60, 80 and 100 mL/kg of total fluid (including both parenteral and enteral routes) on days 1, 2, and 3, respectively, whereas the restricted arm received 40, 60, and 80 mL/kg of total fluid on the same days of life. Fluid was increased by 20 mL/kg per day in either group if all of the following criteria were met: Daily weight change between 1% and 3% of birth weight, daily serum sodium between 130 and 145 mEq/L, daily urine specific gravity between 1. 005 and 1.020, and daily urine output between 1 and 4 mL/Kg/hr.
Babies exhibiting signs of fluid overload (all of the following: daily weight loss of <1% of birth weight, serum Na level of <130 mEq/L, urine specific gravity of <1.005, and urine output of >3 mL/kg/hr) or dehydration (all of the following: daily weight loss of >3% of birth weight, serum Na concentration of >145 mEq/L, urine specific gravity of >1.020, and urine output of <1 mL/kg/hr) during the study period were excluded. Any baby developing hypoglycemia (random blood sugar level of <40 mg/dL, measured using a point-of-care glucometer) was withdrawn from the study. A solution of 10% dextrose was administered for the first two days, and electrolytes were administered after 48 hrs to both groups. Daily weight, serum Na concentration, blood urea nitrogen (BUN) level, and creatinine level were measured, and intake/output was calculated±4 hrs of completion of a 24 hr period from the time of birth until 72 hrs of life. Intervention was continued for the first 72 hrs of life. Data regarding fluid intake and physiological parameters were collected until 72 hrs of life, and data pertaining to the respiratory support were obtained until the requirement of CPAP or oxygen.
The primary outcome of the study was duration of CPAP support in both groups.
Following secondary outcomes were considered: Incidence of CPAP failure in both groups, duration of oxygen requirement after weaning from CPAP, incidence of common neonatal morbidities (hyperbilirubinemia, hypoglycemia, and dehydration).
Statistical analysis
The study population was tested for normality using the Kolmogorov-Smirnov Test. Continuous variables were displayed as mean±SD for normally distributed data and as median (interquartile range) for skewed data. Categorical variables were presented as frequencies and percentages. The unpaired Student t test was used for quantitative variables with a normal distribution, and the Mann-Whitney U test was used for variables with a skewed distribution. The chisquare test was performed for qualitative variables. All study outcomes were analyzed using SPSS (version 23; IBM corporation, Armonk, NY, USA),with a p value of <0.05 considered significant. Analysis was performed on an intention-to-treat basis.
Results
Of 178 babies assessed for eligibility, 78 were excluded and 100 were enrolled in the study. Among the enrolled neonates, 50 each were allocated to the standard fluid and restricted fluid groups. Four babies from each group were excluded. Thus, 46 babies in each arm were analysed (Fig. 1). A total of two babies from each group developed hypoglycemia, two babies from the restricted group and one baby from the standard group developed dehydration, and one baby from the standard group developed air leak. No difference was observed in the incidence of hypoglycaemia (4% in each group, p = 1.00) and dehydration (2% in the standard arm vs 4% in the restricted arm, p = 0.557) between the two arms. Baseline characteristics of the two groups are shown in Tables 1 and 2. Overall, both groups were similar in every aspect, except that more babies in the restricted arm had 5 minutes Apgar of ≥8 (97.82% vs 84.78%, p = 0.026) (Table 1). If we consider late preterm separately, babies allocated to the restricted arm were heavier (2250 g±433.56 g vs 1996. 74 g±365.92 g, p = 0.034). All the other parameters, including the receipt of antenatal steroid, were similar between the two groups (48% in the restricted arm vs 43.47% in the standard arm, p = 0.753). In case of term babies, no difference was observed in baseline parameters (Table 2).

Trial flow chart.
Baseline characteristics of enrolled neonates allocated to standard and restricted fluid group
SD – Standard deviation, n- number, result of continuous variables are shown as mean±SD for normally distributed data and as median(Interquartile range) for skewed data and result of categorical variables are shown as number(percentage).
Baseline characteristics of enrolled neonates stratified as per gestational age
The restricted group had exhibited more cumulative weight loss at the end of the study period (6.08% ±0.732% vs 4.99% ±0.661%, p < 0.001), reflecting the difference in fluid management. Similarly, at the end of the study period, serum Na (137. 37±0.837 mEq/L vs 136.64±1.155 mEq/L, p = 0.001) and BUN levels (10.92±0.615 mg/dL vs 10.58±0.74 mg/dL, p = 0.021) were higher in the restricted arm. Although urine output was low in the restricted group on day three (1.92±0.175 mL/kg/hr vs 2±0.134 mL/kg/hr, p = 0.018), no difference was observed on days one and two. Likewise, no difference was observed between serum Na and BUN levels on days one and two between the two arms. Regarding the primary outcome, babies in the restricted arm required CPAP for significantly less duration compared with those in the standard arm (48[42,54] hr vs 54[48,72] hr, p = 0.002). However, the incidence of CPAP failure (4.34% in the restricted arm vs 6.52% in the standard arm, p = 0.645) and post-CPAP O2 requirement were not different (Table 3).
Study outcome of the entire cohort
U. O – urine output, S- serum, BUN- Blood urea nitrogen, n- number, result of continuous variables are shown as mean±SD for normally distributed data and as median(Interquartile range) for skewed data and result of categorical variables are shown as number(percentage).
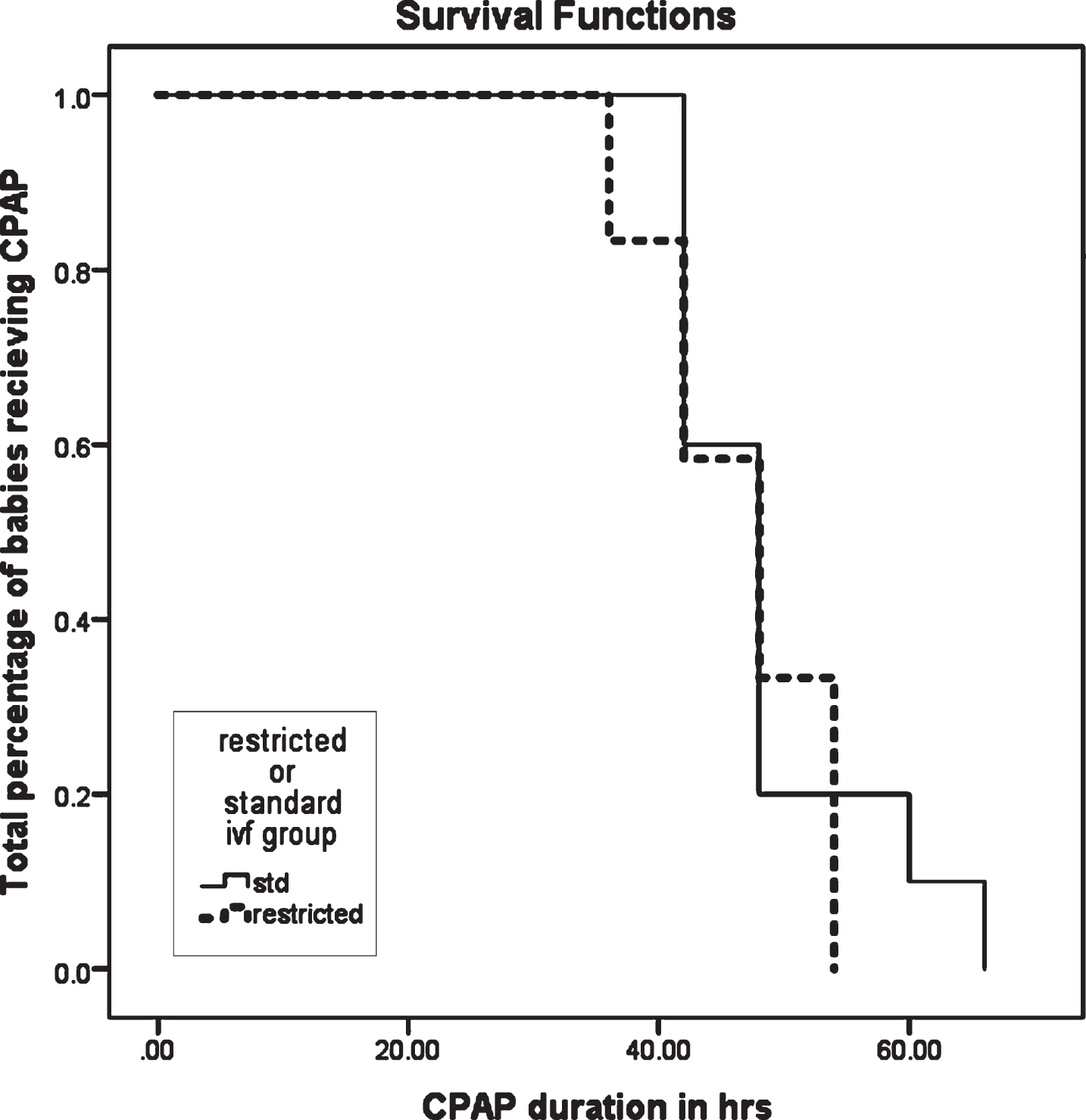
In the subgroup analysis, both late preterm and term infants exhibited greater weight loss at the end of 72 hrs in the restricted group. In late preterm infants, urine output and serum Na and BUN levels at 24 hr differed significantly between the two arms. No significant difference was observed in these parameters at the end of days two and three, except that the serum Na level in the restricted group at 72 hr was higher. However, in term infants, only BUN levels were higher in the restricted group at 24 hr, 48 hr, and 72 hr. Urine output and serum Na and creatinine levels were not different in term babies allocated to the different treatment groups. However, the primary outcome was different in the late preterm and term infants. In late preterm, CPAP duration was significantly less in the restricted group (45.36±11.49 hr vs 59.74±22.98 hr, p = 0.007). However, no significant difference was observed in CPAP duration in term infants allocated to the restricted and standard arms (54[48,54] hr vs 54[48,66] hr, p = 0.183) (Table 4). A Kaplan – Meier analysis of the effect of fluid management on CPAP duration for term infants revealed no significant difference (Fig. 2). However, a Kaplan- Meier analysis for late preterm infants demonstrated significant reduction in CPAP duration (Fig. 3). In both term and late preterm infants, the incidence of CPAP failure, post- CPAP O2 requirement, phototherapy, and exchange transfusion rates did not differ between the two treatment groups.
Subgroup analysis
U. O – urine output, S- serum, BUN- Blood urea nitrogen, result of continuous variables are shown as mean±standard deviation for normally distributed data and as median(Interquartile range) for skewed data and result of categorical variables are shown as number(percentage).
Kaplan – Meier analysis of the effect of restricted fluid management on duration of CPAP (hrs) in term babies. Note: No significant difference in the duration of CPAP (p 0.183).

Kaplan–Meier analysis of the effect of restricted fluid management on duration of CPAP (hrs) in late preterm babies. Note: Significant difference in the duration of CPAP (p 0.007).
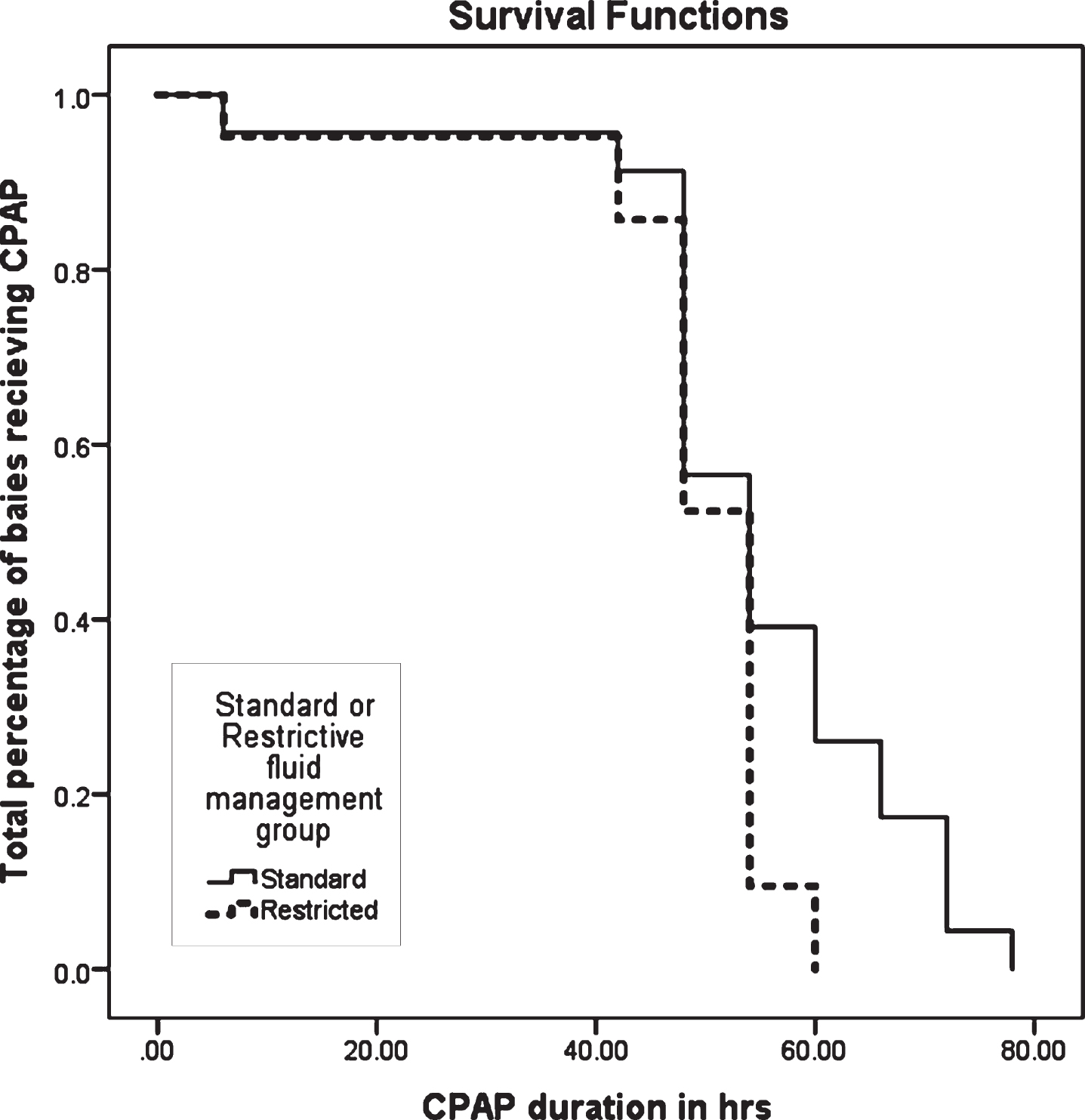
We further analysed the primary outcome in late preterm babies. In our cohort, less than 50% of eligible late preterm babies received antenatal steroid (43.47% in the standard arm and 48% in the restricted arm, p = 0.753) (Table 2). In recent trials, antenatal steroid reduced respiratory morbidity and the requirement of respiratory support in late preterm babies. In our study, fluid restriction did not reduce CPAP duration in late preterm babies exposed to antenatal steroid (46.5±6.83 hr in the restricted arm vs 48.6±8.22 hr in the standard arm, p = 0.519). However,in babies not exposed to antenatal steroid, fluid restriction reduced CPAP duration (44.31±14.81 hr in the restricted group vs 68.30±27.11 hr in the standard group, p = 0.009) (Table 5). A survival analysis of late preterm babies with and without antenatal steroid revealed no significant benefit with respect to CPAP duration in late preterm babies with steroid (Fig. 4). However, a significant reduction in CPAP duration was noted in late preterm babies without steroid (Fig. 5).
CPAP duration in different subgroups
Result of continuous variables are shown as mean±standard deviation for normally distributed data and as median (interquartile range) for skewed data.
Kaplan–Meier analysis of the effect of restricted fluid management on duration of CPAP (hrs) in late preterm exposed to antenatal steroid. Note: No significant difference in the duration of CPAP (p 0.519).
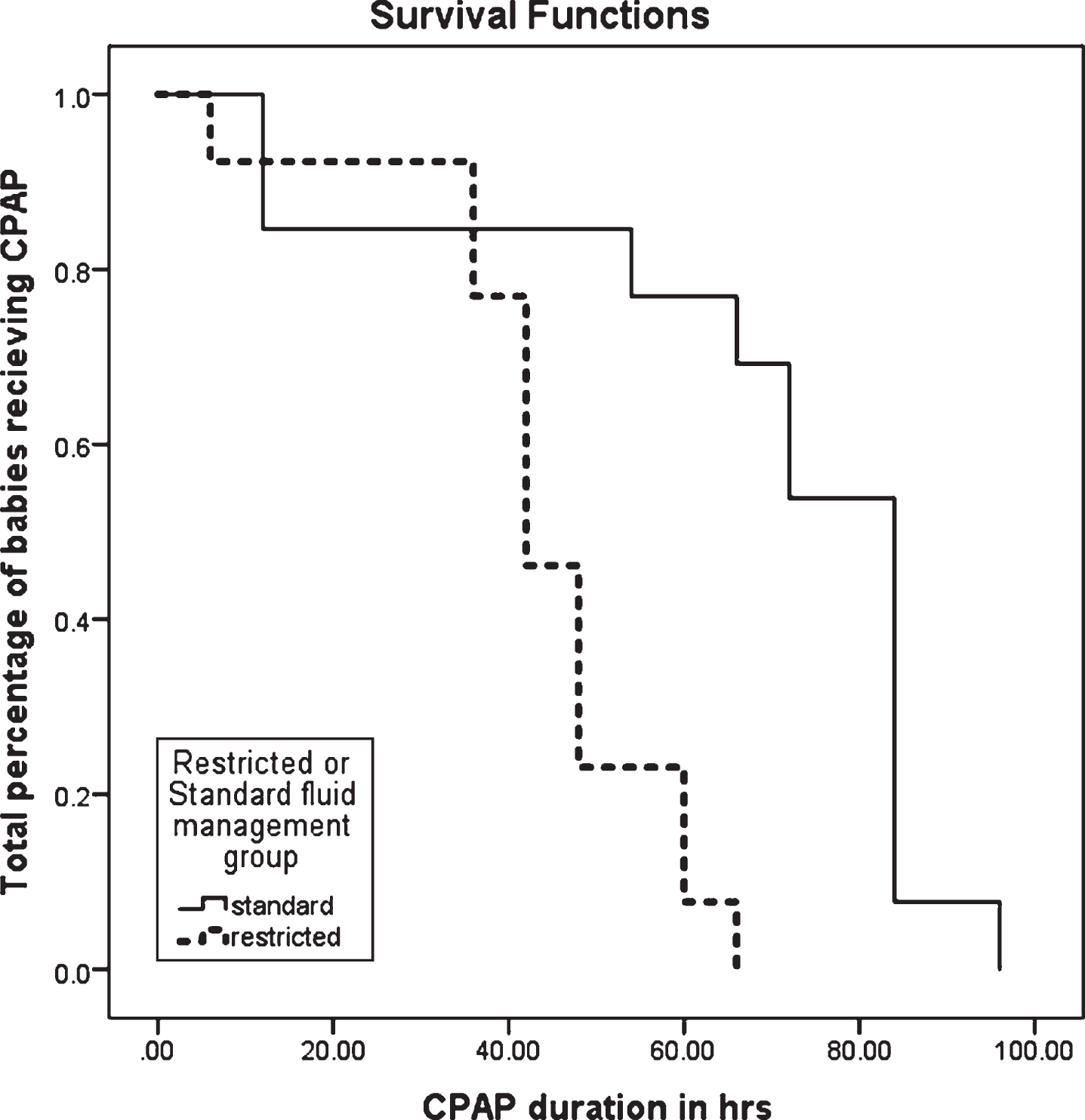
Kaplan–Meier analysis of the effect of restricted fluid management on duration of CPAP (hrs) in late preterm not exposed to antenatal steroid. Note: Significant difference in the duration of CPAP (p = 0.009).
This randomized controlled trial revealed some intriguing results. First, fluid restriction in late preterm and term babies with TTNB and requiring CPAP reduced the duration of respiratory support. Second, treatment was more beneficial in late preterm babies than in term babies, and finally, restricted fluid management was more effective in late preterm babies not exposed to antenatal steroid than in those exposed to antenatal steroid. The issue of safety should be addressed first because restricted fluid might predispose these babies to dehydration. However, these babies are usually cared under supervision and provided measured feed or fluid in the intensive care unit. Physiologically, term healthy babies in the first 72 hr after birth are in a state of dehydration because of inadequate breast milk intake by the babies and inadequate breast milk production by the mothers. Mimicking normal extra uterine physiology should not be harmful to babies. However, a higher fluid intake in the first few days of life is associated with a higher risk of BPD and symptomatic PDA in preterm newborns [18, 21]. Several studies and meta-analysis have confirmed the safety of restrictive fluid strategy in the first few days of life [18, 22]. In our study, no difference was observed in the adverse effects between the two groups. Because the pathophysiology of TTNB is excess fluid in the lungs and its delayed absorption, creating less burden for the baby by restricting fluid in the first 72 hr of life seems logical. One interesting finding was the lack of apparent benefit of fluid restriction on CPAP requirement in term babies and in late preterm babies exposed to antenatal steroid. The answer lies in the pathophysiology of fetal lung fluid secretion and clearance that occurs in three distinctive stages. In the fetal stage,the lung epithelium remains in the secretory mode, relying on active Cl– secretions through Cl– channels and relatively low reabsorption activity of Na+ channels. In the transitional stage, a reversal in the direction of ion and water movement is observed due to an increased expression of Na+ channels in the lung epithelium. The net increase in Na+ movement into the cell can also cause a change in the resting membrane potential, thus leading to a slowing and eventually reversal of the direction of Cl– movement through the Cl– channel. The adult stage represents the lung epithelium with predominant Na+ reabsorption through Na+ channels and possibly Cl– reabsorption through Cl– channels [23]. After birth, lung fluid is rapidly cleared by a two-step process. The first step is the passive movement of Na+ from the lumen across the apical membrane into the cell through Na+ permeable ion channels, and the second step involves the active extrusion of Na+ from the cell across the basolateral membrane into the serosal space. Epithelial Na+ channels (ENaC) that regulate the first step are rate-limiting in this process [24]. ENaC is developmentally regulated with peak expression achieved only at term gestation. Thus, late preterm infants are born with a lower expression of ENaC, which reduces their lung fluid clearance after birth, than term babies [25]. However, the use of antenatal steroid increases the expression of ENaC in late preterm infants, making them more efficient at lung fluid clearance after birth [26]. Thus, late preterm infants, especially those not exposed to antenatal steroid, are at a physiologically challenged state after birth, which could be exacerbated further by volume overload. Thus, these subgroups of babies are the most benefitted by restrictive fluid strategy. However, term and late preterm babies exposed to antenatal steroid are born with sufficient ENaC to handle residual lung fluid, even in the absence of a restrictive fluid regimen.
One of the strengths of the study was the strict objective criteria of CPAP weaning and failure to minimize subjective decisions of physicians regarding CPAP requirement. Another strength was regular monitoring of biochemical and physiological parameters(weight change, urine output, BUN, and creatinine) to determine the clinical status of babies. We followed strict randomization and allocation concealment to minimize bias in our study. However, blinding was not possible due to the nature of intervention.
Our study has several limitations. Being a single-center study, our results might not be generalized to every TTNB baby in all hospital types, especially in rural areas where there is no provision of CPAP. The effect of fluid restriction on babies with TTNB who required respiratory support other than CPAP (only oxygen, or mechanical ventilation)was not investigated. Our study was not adequately powered to detect a difference in the primary outcome (CPAP duration) in different subgroups (term, and late preterm babies with and without steroid exposure). The trend of improved outcome in late preterm babies, especially in those who did not receive antenatal steroid, requires further confirmation in an adequately powered randomized controlled trial. We did not consider the duration of hospital stay and hospital costs in different groups. Stroustrup et al. [20] demonstrated significant cost savings per patient with severe TTNB who received restricted fluid. However, they did not observe any difference in the NICU stay duration between the two groups. Another study from Iran revealed no differences in the hospital stay between the two groups, but they did not comment on any difference in the hospital costs [22]. Although few studies have been conducted in other developing countries, this randomized controlled trial is the first from India to explore differential fluid strategy in babies with TTNB requiring CPAP [22, 27]. Despite few limitations, this study showed that restrictive fluid strategy can be safe and effective adjunct in treating babies with TTNB who require CPAP. Overall, this study confirms the findings of Stroustrup et al. [20] in an Indian population.
Conclusion
This randomized controlled trial demonstrated the safety and effectiveness of restrictive fluid strategy in reducing CPAP duration in late preterm and term babies with TTNB. Late preterm babies, especially those not exposed to antenatal steroid, are the most benefitted by this strategy.
Disclosure statement
Financial disclosure
All of the authors have no financial interest relevant to this article.
Human research statement
Informed consent was taken from the parents of eligible babies before enrolment and permission from the institutional Ethical Committee was obtained.
Funding
None.
Conflict of interest
The authors declare no conflict of interest.
Contribution of authors
SKS-Protocol preparation, literature search, manuscript editing and review, approval of the final manuscript.
SP- Protocol preparation, literature search, conduct of the study, data acquisition, data analysis, manuscript preparation, editing and review, approval of the final manuscript.
RM- Protocol preparation, conduct of the study, data analysis, statistical analysis, approval of the final manuscript.
Footnotes
Acknowledgments
The authors deeply appreciate the contributions and help of the nursing staffs of the neonatal unit of IPGME & R and SSKM Hospital, Kolkata, India. This manuscript was edited by the editing India.