
Abstract
OBJECTIVES:
This study was conducted in order to explore and analyze the status of gestational diabetes (GDM) amongst pregnant women in Dubai, United Arab Emirates (UAE); a country with high prevalence of diabetes. We aimed to describe GDM-associated risk factors and clinical outcomes of pregnant women and their neonates. Our objective was to contribute to the broader literature on reproductive health disparities and to inform efforts to improve GDM care at our region.
METHODS:
Chart review of case records were used to collect data on both maternal and neonatal parameters and outcomes during the specified study period from two main maternity hospitals in Dubai.
RESULTS:
UAE national women with GDM were more prone to be obese or overweight compared to non-UAE women (p < 0.0001, and p < 0.0001 respectively). In addition, UAE national women with GDM had higher history of GDM in previous pregnancies (p < 0.0001) and more family history of diabetes (p < 0.0001).
The neonate admission into NICU was significantly associated with cesarean section (p < 0.0001), twins (p < 0.0001), preeclampsia (p = 0.02), receiving MgSO4 (p = 0.02), birth weight less than 2500 g (p < 0.0001), low Apgar scores (p < 0.0001), baby with congenital anomaly (p < 0.0001), and neonatal hypoglycemia (p < 0.0001).
CONCLUSIONS:
Our results demonstrate that pregnant women with GDM who are UAE nationals and have higher parity need to be under special attention during their pregnancy in order to improve both maternal and neonatal outcomes.
Introduction
Diabetes has reached epidemic proportions worldwide, and the United Arab Emirates (UAE) is no exception [1]. The rising tide of diabetes is evident in our antenatal services with an ever increasing number of pregnancies complicated with diabetes and gestational diabetes mellitus (GDM) accounts for the majority of cases. GDM is a condition characterized by glucose dysregulation of variable severity with onset or first recognition in pregnancy. Pregnancies with GDM are categorized as high risk as they carry a heavy burden on both the mother and neonate if not optimally managed. Accordingly, efforts need to be in place to ensure that outcomes in mothers with GDM are similar to the general population [2].Accurate data to define the prevalence of GDM in the UAE are not yet available, but in Al Ain, a diagnostic rate of at least 8% amongst UAE Nationals has been shown, with a screen positive rate of 19.8% amongst a multi-ethnic expatriate population. Figures of 11% from Saudi Arabia and 5.4% from Bahrain for diagnostic GDM have been reported, but with differing methodology. The difficulty in getting accurate prevalence estimates lies in the varying methods of diagnosis. This has led to varying statistics across different centers within the same region and across the world. The World Health Organization (WHO) adopted criteria developed by the International Association of Diabetes and Pregnancy Study Group (IADPSG) in 2013 for the diagnosis of GDM [3, 4]. However, since the release of the IADPSG consensus guidelines there has been some uniformity in screening, diagnosis and management of GDM.GDM is associated with adverse maternal and fetal outcomes such as macrosomia, subsequent delivery risks, birth trauma, and increased need for cesarean delivery in the short term [5, 6]. In the long term, mothers with GDM and their offspring are at an elevated risk for obesity, type two diabetes mellitus (T2DM) and other cardiovascular diseases [7 –9]. Prompt diagnosis of GDM is the first step towards effective management and prevention of adverse outcomes. Many low- and middle-income countries are experiencing demographic, nutritional and epidemiological transitions that have resulted in a surge of non-communicable diseases. Shifts in dietary patterns, urbanization and a decrease in physical activity are key elements in these transitions [10]. The emirate of Dubai in the UAE has two main government hospitals that cater for maternal and child health care. Both hospitals implement the same protocol for screening and management of GDM. However, there has been no comparative data on maternal and neonatal outcomes from these two hospitals. Our main objective was to estimate the prevalence of GDM and assess both maternal and neonatal outcomes in these two tertiary care hospitals (Dubai hospital and Latifa hospital) following the adoption of a unified screening, diagnostic, and management protocol. We aimed to assess the rate of cesarean sections, pre-eclampsia, and prevalence of macrosomia, intrauterine growth restriction (IUFGR)/intrauterine fetal death (IUFD), stillbirths and neonatal hypoglycemia in GDM patients.
Methods
Study design
This descriptive retrospective study was conducted among pregnant women visiting maternity clinics in two main maternity hospitals in Dubai: Latifa hospital (LH) and Dubai hospital (DH). The subjects were women diagnosed with GDM from all nationalities; from 2012 until 2017.
Study participants and procedure
Chart reviews of case records were used to collect data on both maternal and neonatal parameters and outcomes during the specified study period from both hospitals. The inclusion criteria mandated participants to be pregnant women with GDM. Exclusion criteria were pregnancies complicated with any of the following: pre-existing diabetes (type 1/type 2), pre-existing hypertension (HTN), thyroid disorders, renal diseases, cardiac pathologies, and autoimmune conditions.
Data collection
Several maternal parameters and outcomes were collected from the patient’s files. These parameters are as follow: Maternal age at delivery, nationality, body mass index (BMI) at beginning and late pregnancy, GDM treatment: Diet/met for min/insulin, previous history of GDM, family history of diabetes, parity, gestational age at delivery (weeks), mode of delivery, reason for cesarean delivery (C/S), HbA1c during pregnancy, number of antenatal visits, induction of labor, instrumental delivery, postpartum hospital care of seven days or more. Neonatal outcomes were also collected as follows: Birth weight, large/appropriate/small for gestational age, IUFD/Stillbirth, congenital anomalies, Apgar score, neonatal hypoglycemia, admission to neonatal intensive care unit (NICU). All data on GDM women in DH & LH from year 2012-2017 were collected.
Screening for GDM in Latifa and Dubai hospital
Universal screening for all low risk women at booking by fasting blood sugar (FBS) and oral glucose tolerance test (OGTT) at 24–28 weeks is performed. Detailed obstetric, medical and family history to detect risk factors to develop GDM in current pregnancy is taken. If identifiable risk factors present; OGTT at 14–16 gestational week was implemented. If OGTT results were normal, then it was repeated again at 24–28 gestational week (Table 1).
Screening and diagnosis of Gestational Diabetes Mellitus (GDM) in Dubai Health authority (DHA)
Screening and diagnosis of Gestational Diabetes Mellitus (GDM) in Dubai Health authority (DHA)
All collected data were entered into STATA version 15 (Stata Corp. 2017. Stata Statistical Software: Release 15. College Station, TX: Stata Corp LLC) for statistical analysis. Descriptive statistics were computed for the socio-demographic variables. The percentage differences in the total responses were determined using the Chi-square test and statistical significance recorded for non-parametric data. For all analyses, alpha (α) was set at 0.05.
Ethics statement
The study was approved by the institutional review boards of Dubai Health Authority, Dubai (Approval # DSREC-12/2016-03). Aggregate reporting of data assured to enhance confidentiality and accurate reporting. Independent and blinded data analysis was performed.
Results
Participant characteristics
Out of around 5000 medical files of women with GDM requested, we were able to get information from 3805 patients. That was due to inaccessible files for GDM women or not enough documentation within the files. Majority of our GDM pregnant women were between 25–35 years, UAE national, had ≤2 parity, with gestational age at delivery around 37–40 weeks, having BMI more ≥30 (Table 2). The evaluation of antenatal history of diabetes and pregnancy outcome for pregnant women in this study revealed that the majority of the women with GDM were treated by diet modifications, did not have previous history of diabetes but had positive family history of diabetes, did not have preeclampsia, did not receive MgSO4, and did not receive anti hypertension (anti-HTN) (Table 3). The majority of GDM pregnant women had HbA1c during pregnancy of less or equal to 6.1 %; and less than 10 antenatal visits. The main stream of GDM pregnant women did not receive induction of labor and had normal vaginal delivery (Table 2). When evaluating the rate of C/S among pregnant women with GDM, it was 40.5% with the most common reason being having previous scar. The postpartum hospital care for GDM pregnant women was ≤7 days in the majority (98%) of the women.
Descriptive demographic characteristics of pregnant women (n = 3805). * BMI: Body Mass Index is considered underweight if it is <18.5; normal if it is 18.5–24.9; overweight if between 25–29.9; and obese if ≥30
Descriptive demographic characteristics of pregnant women (n = 3805). * BMI: Body Mass Index is considered underweight if it is <18.5; normal if it is 18.5–24.9; overweight if between 25–29.9; and obese if ≥30
Antenatal history of diabetes and pregnancy outcome of pregnant women participants (n = 3805)
The postnatal outcome of neonates in this study were favorable in the majority (99%), with Apgar score of ≥7 in the mainstream of delivered babies, congenital anomaly was detected only in 2% of the neonates, and admission to the NICU in 8% (Table 4). The most common reason for admission in the NICU was prematurity of the neonate (36%). The correlation assessment of pregnant women with GDM and the pregnancy and neonatal outcome showed significant association between reason for C/S and women age (p < 0.0002), gestational age (p < 0.0001), and preeclampsia (p < 0.0001). The neonate admission into the NICU was significantly more in Latifa hospital (p < 0.0001), more associated with C/S (p < 0.0001), twins (p < 0.0001), having preeclampsia (p = 0.02), receiving MgSO4 (p = 0.02), birth weight less than 2500 g (p < 0.0001), Apgar score in 1 minute and 5 minutes less than 7 (p < 0.0001), baby with congenital anomaly (p < 0.0001), and neonatal hypoglycemia (p < 0.0001).
Postnatal outcome of neonates (n = 3805). * Neonatal intensive care unit. Low birth weight (<2500 g), Normal birth weight (2500–4000 g), High birth weight (>4000 g). RDS: Respiratory distress syndrome.
Postnatal outcome of neonates (n = 3805). * Neonatal intensive care unit. Low birth weight (<2500 g), Normal birth weight (2500–4000 g), High birth weight (>4000 g). RDS: Respiratory distress syndrome.
Pregnant women receiving MgSO4 or anti-HTN medication were more prone to deliver in earlier gestational age (p < 0.0001) and having C/S (p < 0.0001). Parity of GDM pregnant women was significantly associated with nationality (p < 0.0001), with UAE national women with GDM having higher parity then non-UAE national (Fig. 1). Pregnant women with GDM who had higher parity, tend to be more obese or overweight at the beginning and late pregnancy compared to those with lower parity (p < 0.0001), tend to have more positive history of previous GDM (p < 0.0001), and less induction of labor (p = 0.0002).Maternal age was significantly associated with gestational age of the baby. Mothers with GDM who aged >35 were more prone to deliver premature baby (p < 0.0001), having higher BMI at beginning (p < 0.0001), and late pregnancy (p = 0.02); more frequent previous history of GDM (p < 0.0001), higher rate of C/S (p < 0.0001), and higher rate of receiving MgSO4 (p = 0.03) or anti-HTN (p < 0.0001). On other hand, women between 25–35 years of age were having uncontrolled GDM measured by HbA1c (p = 0.04). Rate of C/S in GDM pregnant women was significantly associated with not inducing the labor (p = 0.02), having preeclampsia (p = 0.03), receiving MgSO4 (p < 0.0001) or anti HTN (p < 0.001), baby birth weight less than 2500 g (p < 0.0001), and Apgar score on 1 minute less than 7 (p < 0.0001). UAE national women with GDM were more prone to be obese or overweight compared to non-UAE women (p < 0.0001, and p < 0.0001 respectively). In addition, UAE national women with GDM had a higher history of GDM in previous pregnancies (p < 0.0001) (Fig. 2) and more family history of diabetes (p < 0.0001). Induction of labor was higher in non-UAE women with GDM (p = 0.001) while C/S was higher in UAE national women with GDM (p = 0.04) (Table 5).
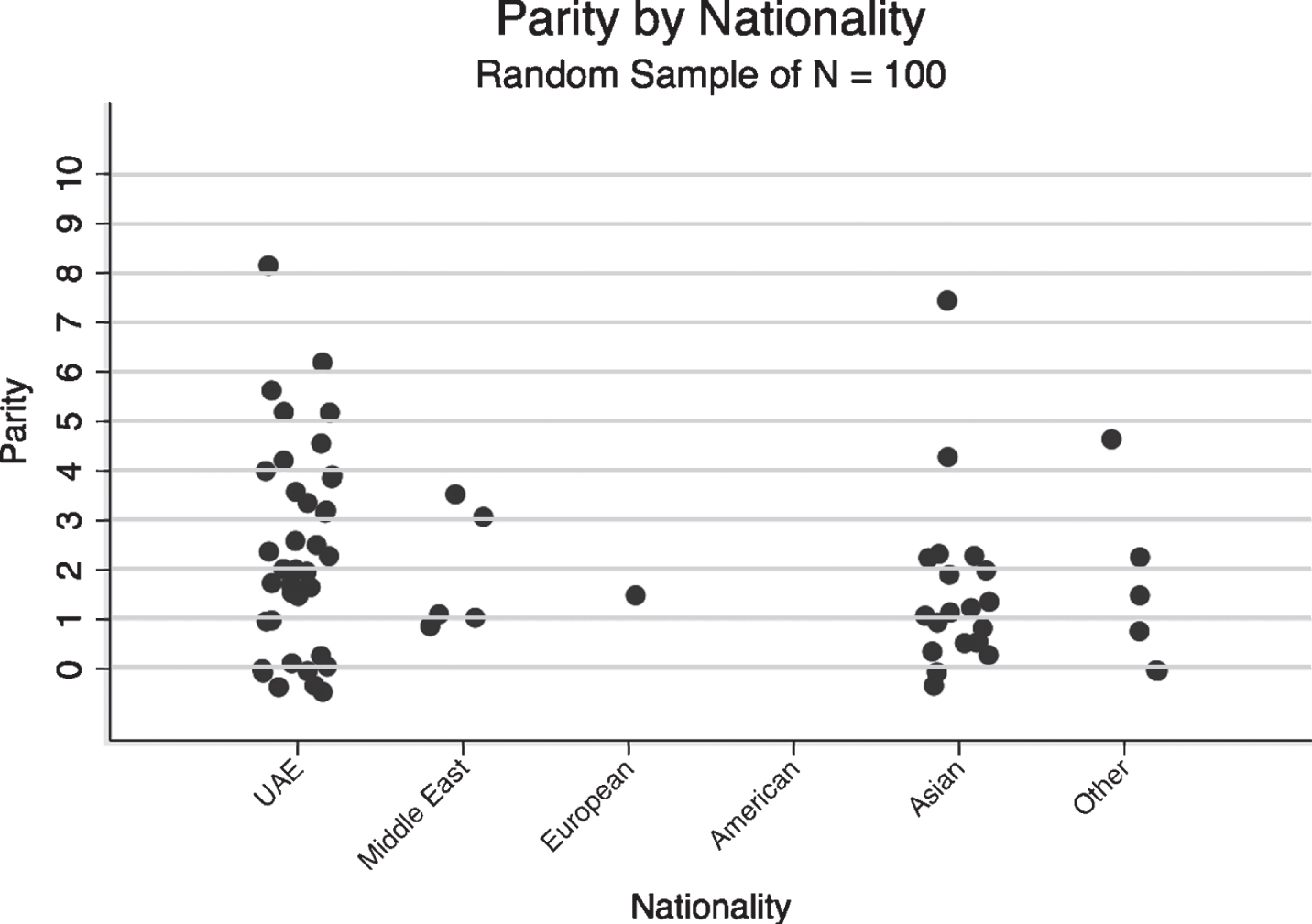
Presenting the pattern of parity predicted by nationality of pregnant women.
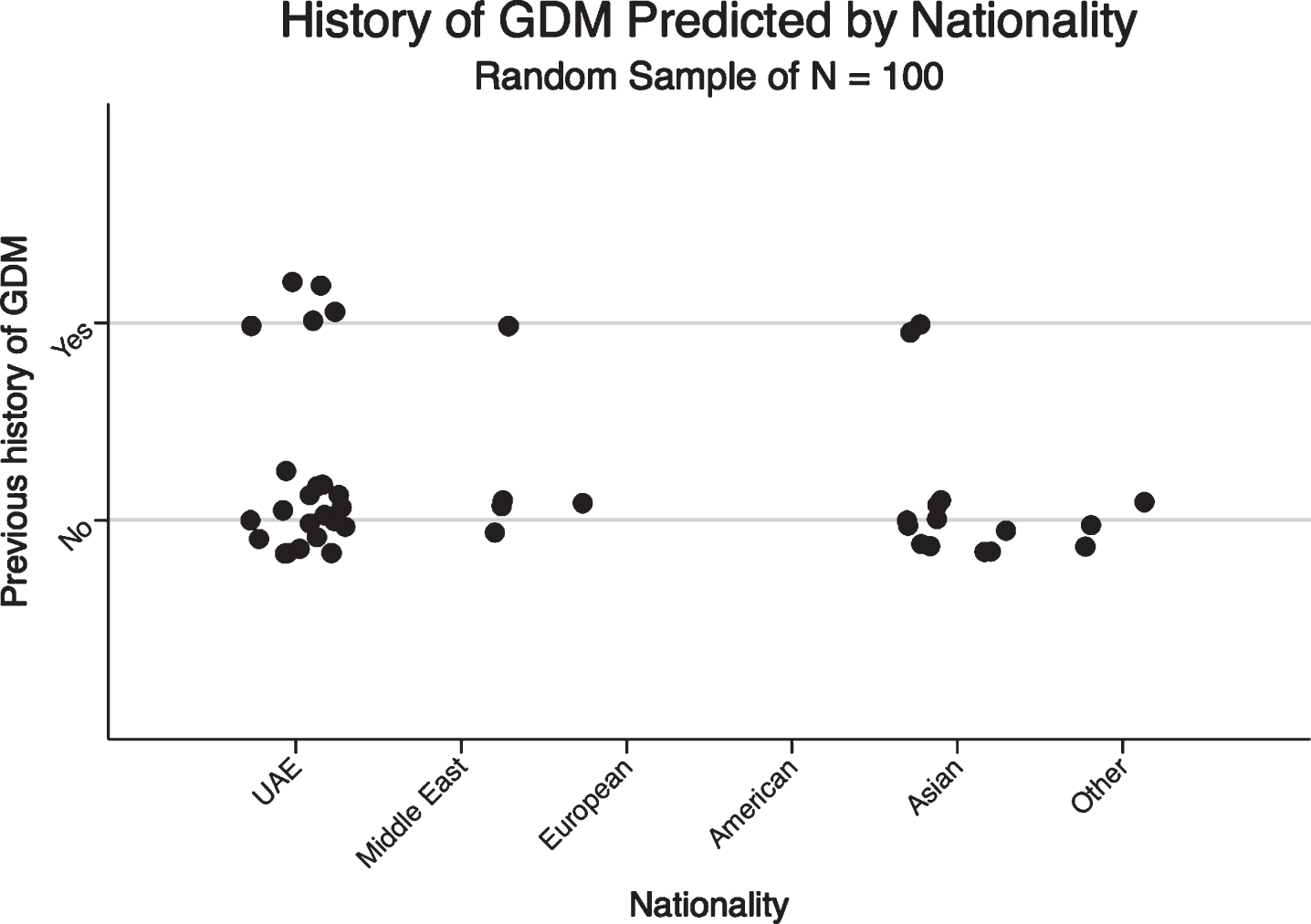
Presenting the history of GDM predicted by nationality of pregnant women.
Factors associated with GDM among pregnant women in UAE (n = 3805). *p < 0.05, significance determined using Montecarlo 2 tailed significance at 95% CI. Only significant results are presented, significance at 95% CI. Only significant results are presented. UAE: Untied Arab Emirates, BMI: Body Mass Index, NVD: Normal Vaginal Delivery, HTN: Hypertension
GDM is a common metabolic alteration, which is defined as any degree of glucose intolerance with an onset or first recognition during pregnancy [11]. GDM increases worldwide and becomes a global health problem with the same risk factors seen for type two diabetes, such as obesity and increased maternal age [11]. The primary aim of diagnosing GDM is to identify women and infants at risk of short or longer term adverse outcomes because GDM is independently associated with an increased risk of maternal-fetal complications, such as preeclampsia, macrosomia, neonatal hypoglycemia, hyperbilirubinemia, and shoulder dystocia [6, 12].
This study was conducted to assess the management of pregnant women with GDM in two major maternity hospitals in Dubai, UAE. The present study shows that higher parity, older age, having pre-eclampsia, and receiving MgSO4 or anti-HTN are associated with unfavorable pregnancy and neonatal outcomes. This is in line with other researches exploring the risk factors in GDM [12, 13]. We have noticed that UAE national women with GDM have higher BMI at beginning and late pregnancy, higher previous history of GDM and family history of diabetes, and higher rate of C/S. This corresponds to the high prevalence of overweight and DM in the general UAE population [14]. A recent study conducted in UAE shows that the rate of C/S is highly increasing among UAE national women [15]. This is an alarm for policy makers to further focus on BMI in UAE national women, especially those with positive family history of DM. UAE national women need critical and urgent awareness on increased weight and its effects on the pregnancy outcomes for both mother and neonate.
Another modifiable risk factor was HbA1c in pregnant women with GDM. Women in age group 25–35 years were more prone of having uncontrolled HbA1c during their pregnancy. We do not believe that this is due to less awareness, rather because this category of women usually are employed women who have less time for self-healthcare than their peers do. A recent study conducted by Ogge K and colleagues [16] showed that women with an elevated HbA1c level were more likely to develop adverse neonatal events compared with those with normal HbA1c level. They further showed that elevated maternal HbA1c was associated with increased incidences of adverse fetal and neonatal events, including neonatal respiratory distress syndrome, pneumonia and jaundice. It is well established that improved glycemic is associated with a lower perinatal mortality and morbidity, and, specifically, a reduction in the risk of macrosomia and shoulder dystocia [17, 18]. Hence, the healthcare providers for pregnant women with GDM need to emphasize on importance of HbA1c and BMI control. More efforts are required to educate women with GDM on how to control these risk factors and improve their pregnancy outcomes. This knowledge must be transferred to pregnant women and further enlighten them of the undesirable consequences of these two parameters on pregnancy outcome. Finally, we need to stress on the effects of nationality and parity on pregnancy outcome.
Limitation of study
The results of this study are limited due to descriptive retrospective study design. The findings of the study cannot be generalized for the whole UAE as the GDM pregnant women were recruited only from Dubai health authority, but could be considered indicative of the context measured. However, this study gives a good insight on GDM management in the UAE, with risk factors associated with unfavorable neonatal outcomes. This study had several strengths; including relatively large sample size and the high prevalence of gestational diabetes give us statistical power to study the associations of interest. However, some limitations must be considered when interpreting the results of our study. First, a family history of diabetes was assessed based on self-report; therefore, we cannot rule out recall bias. Additionally, participants in this study were pregnant women living in Dubai, and the results may not be generalizable to the whole UAE population. Future studies that collect objective measures potentially associated with GDM on the national level may overcome concerns about these potential errors.
In conclusion, pregnant women with GDM who are UAE nationals and have higher parity require closer monitoring during their pregnancy in order to improve both maternal and neonatal outcomes.
Conflicts of interest
No potential conflict of interest was reported by the authors.
Footnotes
Acknowledgments
Appreciation is expressed to all participants in this study.