
Abstract
BACKGROUND:
Bilateral choanal atresia in patients with CHARGE syndrome becomes symptomatic immediately after birth. A prompt diagnosis, the implementation of sufficient preliminary measures, and the delivery of surgical therapy are crucial. This article is intended to assist in terms of diagnostics and a therapy recommendation.
METHODS:
We performed a retrospective study using the medical records of all newborns in the University Hospital in Bonn, diagnosed with bilateral choanal atresia and CHARGE syndrome and underwent surgery at the Department of Otorhinolaryngology, Head and Neck Surgery.
RESULTS:
A total of 21 patients have been treated with a unilateral or bilateral choanal atresia. 14 patients were primarily treated with transnasal endoscopy or underwent transnasal endoscopic surgery as a follow-up intervention (73.68%). Nine patients had a syndromal appearance, which was considered a definite diagnosis in six patients (five with CHARGE syndrome). All five patients with CHARGE syndrome received transnasal endoscopic treatment and a stent was inserted.
DISCUSSION:
Bilateral choanal atresia can be a life-threatening situation requiring acute measures. The therapeutic trend goes towards transnasal endoscopic resection. Primary intervention should be: minimally invasive, one-stage surgery, functional, and associated with low complication rates. Patency can be increased by saline irrigations, topical corticosteroids, endoscopic controls, and regular dilatation. The insertion of stents is controversially discussed but can be useful in syndromal patients. However, adjuvant therapy with a stent and mitomycin C is increasingly being abandoned. A significantly higher recurrence rate must be expected in association with CHARGE syndrome. Stenting should be considered on an individual basis. Continuous training and support of the parents are obligatory.
Introduction
Choanal atresia describes the congenital and complete anatomical closure of the posterior nasal cavity by atresia plates (Fig. 1a and 1b). The computed tomography image (CTI)-assisted evaluation of 63 patients by Brown et al. included almost exclusively descriptions of bony choanal occlusions. These are structurally homogenous in 29% of the cases but show a mixed bony cartilaginous structure in 71% of cases [1]. This distribution ratio can be described as following a 2 : 1 rule. It is also applicable to the ratio of right- to left-sided (71% / 29%) and uni- to bilateral atresia (67% / 33%) [2]. The gender ratio of affected female and male infants is also 2 to 1 [2]. Overall, uni- and bilateral choanal atresia is rare and affects 1 in 5,000– 7,000 newborns [3]. It occurs together with other malformations in 73.6% of cases, and in more than half of the cases (51.2%) it can be attributed to a malformation syndrome (e.g., CHARGE (25.6%), Treacher Collins, Pfeiffer, and trisomy syndrome) [4, 5]. Since almost every bilateral obstruction of the choanae can be assigned to a malformation syndrome (98.4%), a CHARGE syndrome (Coloboma, Heart defects, Atresia of the choanae, Retardation of growth and/or development, Genital and/or urinary defects, Ear anomalies and/or deafness; Fig. 2a) is found in every second infant with syndromal appearance [5]. Due to the CHARGE syndrome, mortality is significantly increased, regardless of surgery [6]. Unilateral choanal atresia tends to occur sporadically and independent of syndromes [5]. If one considers the clinical dynamics of bilateral choanal atresia, it becomes clear that, due to the immediate postpartum manifestation, a rapid diagnosis is essential for the implementation of immediate airway protection measures (e.g., McGovern tube, continuous positive airway pressure (CPAP), orotracheal intubation, tracheotomy) [2, 7]. In contrast to unilateral choanal atresia, which can be occult for years (unilateral nasal obstruction, persistent unilateral rhinorrhea, chronic recurrent sinusitis) [8], the bilateral blockage of the choanae can manifest within minutes as a dramatic airway emergency and represents a life-threatening situation [2, 6]. Due to the congenitally high-positioned larynx, newborns are obligate nasal breathers [8]. Postnatally, they are characterized by dyspnoea attacks, drops in saturation, a reduced Apgar score, and paradoxical cyanosis (Table 1).

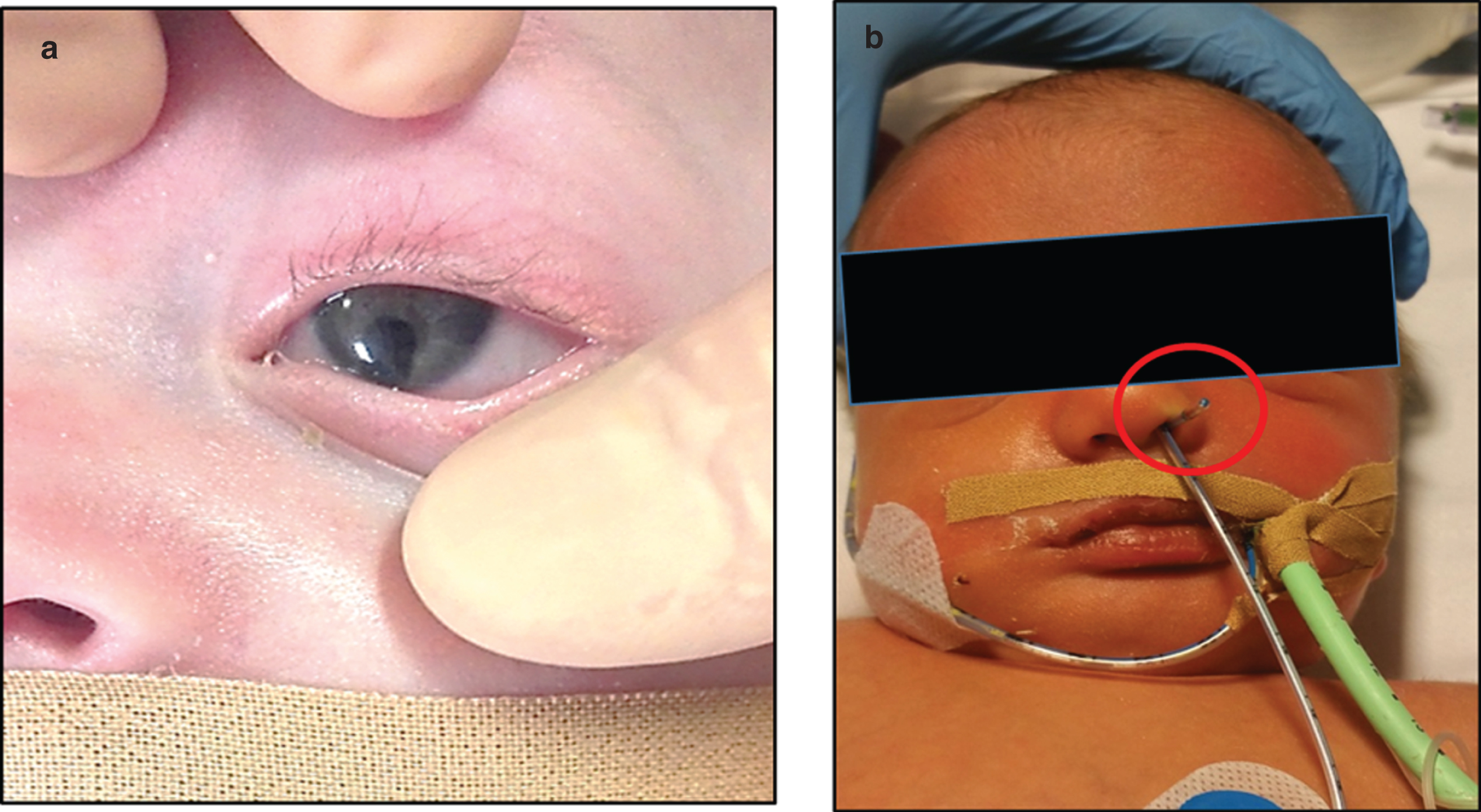
(a) Infant with bilateral choanal atresia associated with CHARGE syndrome: visible, left-sided fissure in the iris. Additional fissure of the choroidea and the papilla of the optic nerve. (b) Phenomenon of folding gastric rube (red circle).
Leading symptoms of uni- and bilateral choanal atresia

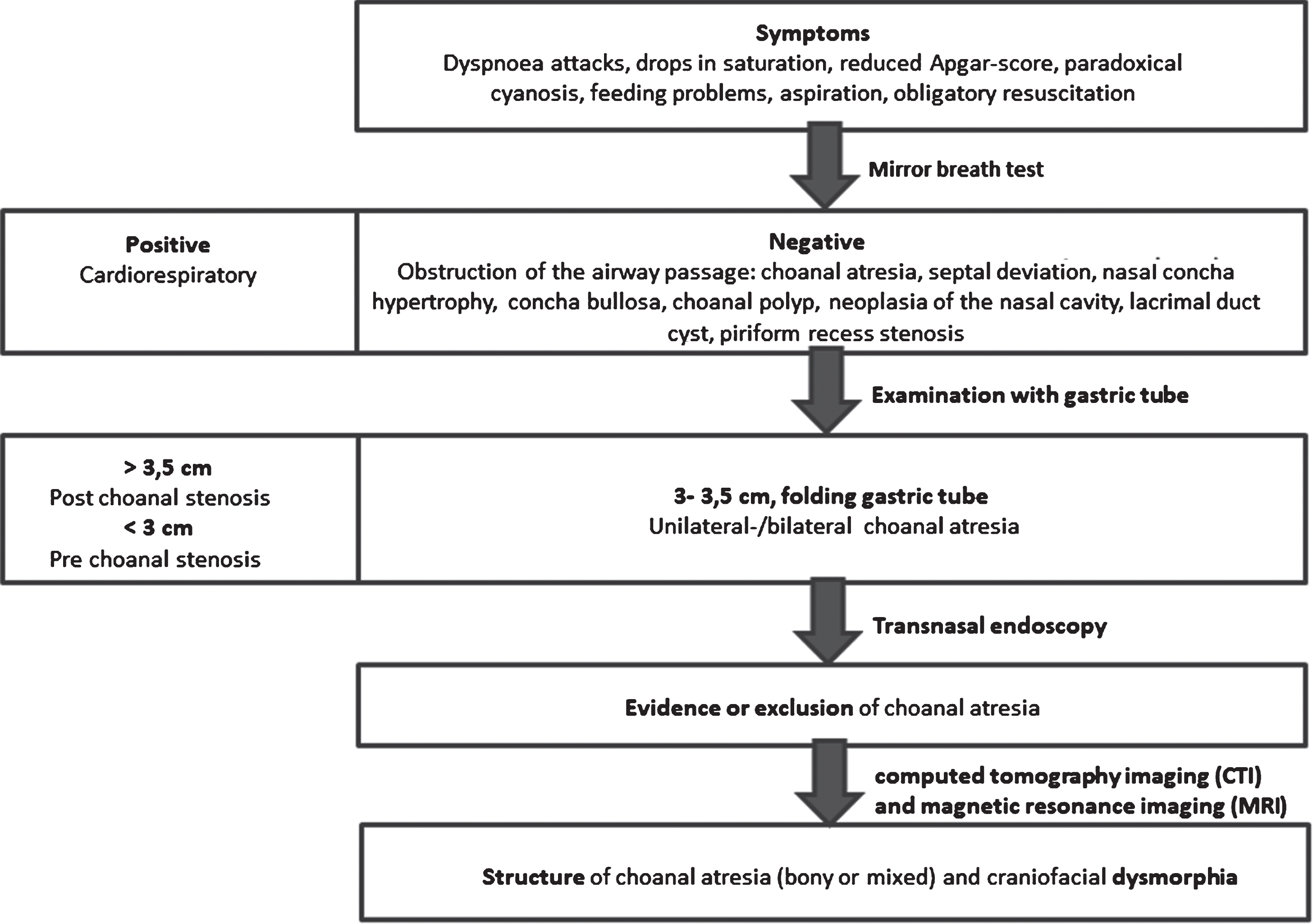
Feeding problems and aspiration events, which may reach the point where resuscitation becomes obligatory, are the avoidable dangerous developments, which must be adequately treated after a successful diagnosis (Tables 2 and 3) [8]. The bilateral examination of the nasal cavity with a thin gastric tube should be performed in symptomatic children. Thus, unilateral choanal atresia may remain unnoticed [7]. An obstruction of the passage, which can be observed at 3– 3.5 cm distance from the alar rim (lower edge of the nostril), and the occurrence of a folding gastric tube are indicative (Fig. 2b) [8]. A negative mirror breath test is considered indicative but not proof. Therefore, in case of abnormal findings, a transnasal endoscopy with a 0° or 30° pediatric endoscope should be regarded as obligatory (Fig. 3a). In some exceptional cases, CTI should be performed as an option to confirm the diagnosis definitively and to exclude differential diagnoses, and determine the thickness as well as the structure of an atresia plate. This can vary between 1 and 12 mm [9, 10]. In syndromal phenotypes, however, CT can provide information on further craniofacial dysmorphia (in 21%), nasopharyngeal constriction, the diameter of the choanae (approximately 0.67 mm in newborns), muscle mass or tension of the pharynx, and the frequently accompanying respiratory abnormalities (in 34%, e.g. tracheomalacia, laryngomalacia, subglottic stenosis) [6, 10].
Diagnostic algorithm
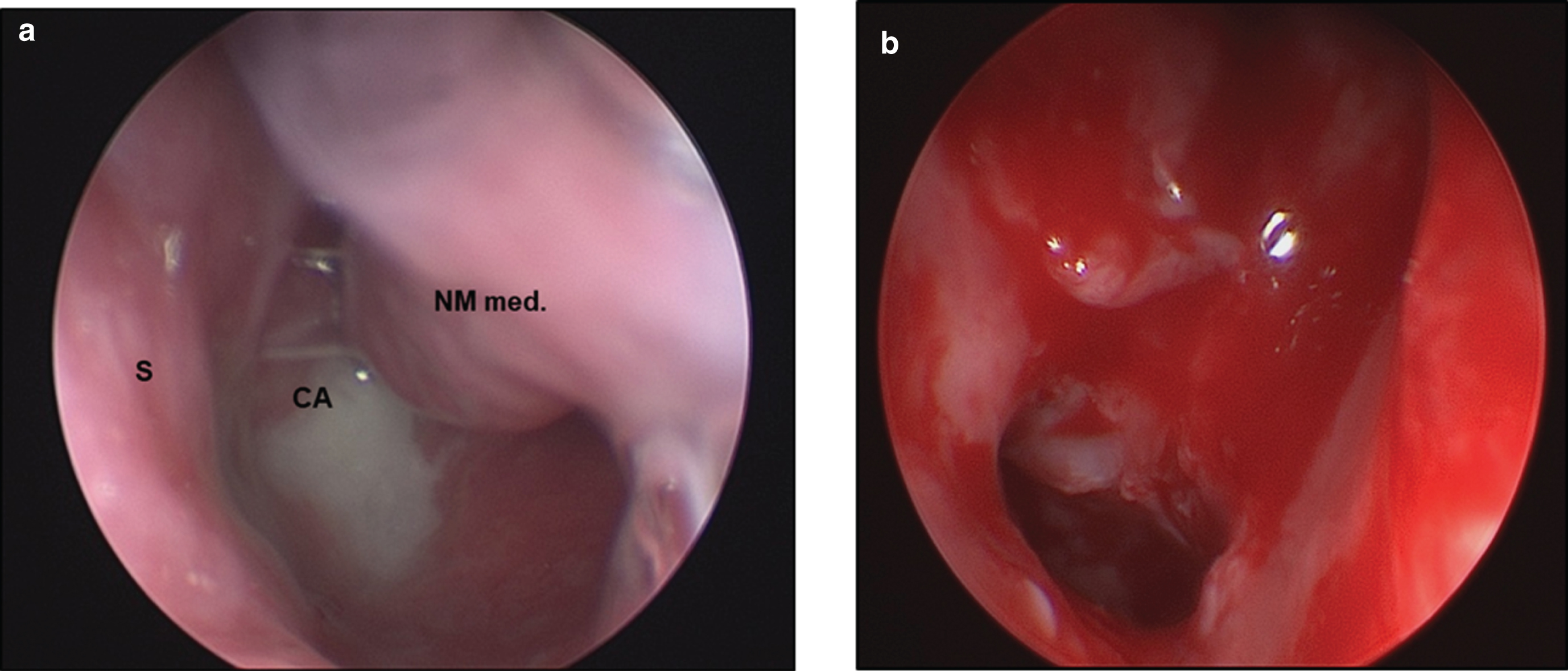
(a) Transnasal endoscopic verification of a choanal atresia (here: left-sided; S = nasal septum; CA = choanal atresia; NM med. = middle nasal concha). (b) Left-sided surgically created nasopharyngeal shunt.
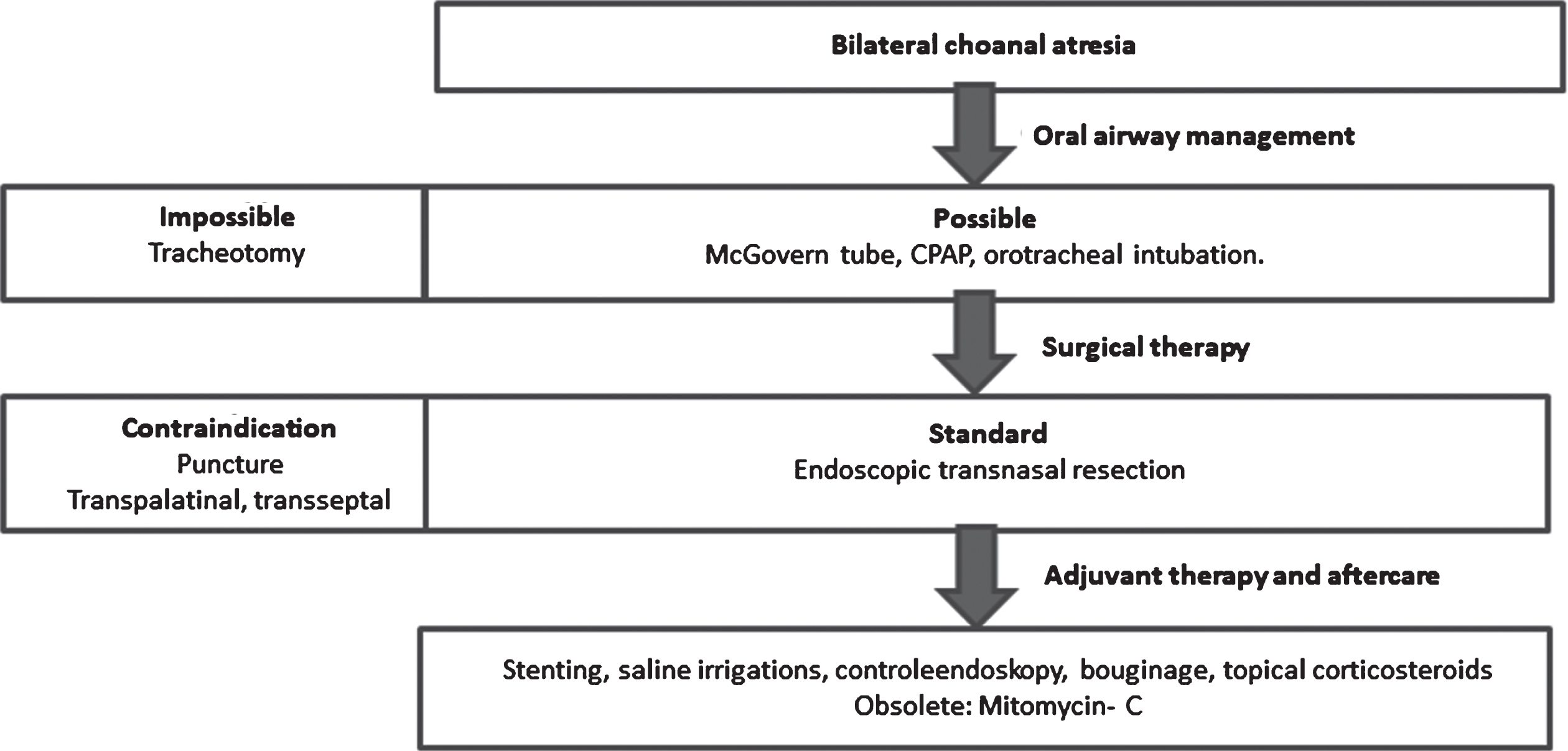
Therapeutic algorithm
Based on extensive research in the medical records of the entire patient population of the University Hospital in Bonn since 2003, we collected the data from patients with bilateral choanal atresia under CHARGE syndrome who were treated and underwent surgery at the Department of Otorhinolaryngology, Head and Neck Surgery.
The analysis of the patient histories was performed retrospectively while also adding the medical records from our Center for Pediatrics, Neonatology, and Pediatric Intensive Care.
Ethical considerations
This study was registered with the ethics committee of the University of Bonn under ongoing file number 129/19. The ethics committee waived the need for informed consent because the study was limited to sole data collection during regular standard practice. Further, there were no changes in treatment as a consequence of this investigation. We got the written consent of the parents concerning the used images.
Results
Since 2003, a total of 21 patients have been treated with a unilateral or bilateral choanal blockage at the University Hospital Bonn. Nineteen of these cases were congenital and two acquired (scar formation). Based on reliable data, we were able to identify 14 patients who were primarily treated with transnasal endoscopy or underwent transnasal endoscopic surgery as a follow-up intervention (73.68%) among the 19 congenital choanal atresia cases. Nine patients had a syndromal appearance, which was considered a definite diagnosis in six patients (five with CHARGE syndrome and one with Crouzon syndrome). All five patients with CHARGE syndrome received transnasal endoscopic treatment, and a stent was inserted in each case. In recent times (2017/2018), we observed a total of three sufficiently documented cases of newborns with CHARGE syndrome and bilateral choanal atresia. If we compare this figure with the current birth rate figures of the registry office of the City of Bonn (3,587 live births in 2015), we can assume that in this area only every 1.39– 1.95 (ø 1.67) years a child with choanal atresia and only every 4.17– 5.85 (ø 5.01) years a child with bilateral atresia is born.
In the cases of bilateral choanal atresia with CHARGE syndrome, the airway was secured using a McGovern tube, CPAP ventilation, or, finally, orotracheal intubation. A tracheotomy was not necessary. Transnasal endoscopic resection of both atresia plates was performed in all cases (Fig. 3a and b). After decongesting the nasal cavity mucosa with privin, the optical adjustment of the atresia plates was achieved using the 0° and 30° pediatric endoscope. While protecting the nasopharynx with the large laryngeal mirror, the mucosa was detached from caudomedial to craniolateral. The underlying atresia plate was treated with the Blakesley forceps or the retrograde punch, and the choana was dilated. The use of a diamond drill was not necessary in any case. Care was taken to ensure that the resection areas were afterward sufficiently covered with mucosa. Subsequently, an I- or U-shaped nasal stent was inserted using the Seldinger technique. Fixation was performed on the bridge of the nose to prevent an ante- or postnasal dislocation (Fig. 4a and b).

(a) Insertion of I-shaped replacement tubes on both sides after surgical repair of choanal atresia. (b) U-shaped Protex intubation tube (size: 4.0) before fixation as adjuvant therapy after endoscopic repair of bilateral choanal atresia.
A male premature baby (36 + 6 weeks of pregnancy, uncomplicated birth) was born in an external hospital. Immediately after birth, it showed a bad oxygenation saturation as well as a reduced Apgar score (1’ 08/ 5’ 04/ 10’ 02) and required cardiopulmonary resuscitation. Both choanae were blocked. Orotracheal intubation was performed without any problems. The detection of a mutation in the CHD7 gene helped to confirm the diagnosis of CHARGE syndrome later. Further diagnoses included congenital heart defects (e.g., persistent foramen ovale, ventricular septal defect, persistent ductus arteriosus) and an iris/choroidal coloboma. The transfer and further care were provided by our neonatal, pediatric intensive care unit. Already on the day of the transfer, the patient was brought to our Department of Otorhinolaryngology, Head and Neck Surgery. On the 5th day of his life, the bilateral choanal atresia was surgically repaired. Two placeholding tubes (seize 2.5 on the right and 3.0 on the left side) were inserted for splinting (Fig. 4a). In the course of time and after temporary removal, they were replaced by 3.5 (after 25 days) and 4.0 (after approx. 3 months) Portex tubes. The endoscopic control inspections were performed in the surgical intervals. They showed well epithelialized choanal channels but overall a clear tendency to shrinking after the removal of the splint material. Due to the lack of persistence of the main nasopharyngeal shunt, re-dilatation, expansion of the choanae, or downgrading to a smaller tube size was necessary twice. Suctioning was performed several times a day, saline irrigations and topical corticosteroids were employed. After six months, the patient was gradually weaned from the tube inserts. A short-term replacement in 2-day intervals was practiced. The parents were instructed to change the tubes on their own.
Discussion
Bilateral choanal atresia is a rare disease. Studies show a low number of cases. There is a controversial discussion about surgical and postoperative therapy and no guideline recommendation, particularly for the use of nasopharyngeal stents in association with CHARGE syndrome [9]. The conflict between the necessary early emergency intervention and the age-correlated recurrence and complication rate (septum injuries, injuries of the nasal concha and the clivus, synechia, cribriform plate ruptures, meningitis, growth retardation, bony malformation), which decreases with increasing intervention age, is problematic [8, 11]. None of our syndromic patients (n = 6) had any severe complications due to surgery. A tendency to restenosis following the primary intervention may result in the need for another surgical intervention. Due to the invariable occurrence of restenosis in patients with CHARGE syndrome, no patient can benefit from the transnasal puncture, whereas 27.3% of the patients can profit from a transpalatal approach and at least 14.3% from a transnasal endoscopic resection [12]. Serious complications such as deformities of the palate in the case of a transpalatal approach (40– 100%) must be considered significantly higher than in the case of a transnasal endoscopic approach (25%). Injuries of the clivus, rhinoliquorrhea, meningitis, and septal damages predominate in endonasal puncture [13, 14]. In all procedures, the transnasal approach proved to be low in bleeding and complications, visually and tactilely well controllable, well executable given the narrow anatomical conditions, and preferable from a cosmetic point of view [15–17].
Asher et al. state that the success rate of early intervention in children with associated CHARGE syndrome is rarely promising. They recommend early tracheotomy as therapy of choice [11]. We do not consider this a sensible approach. In the patients treated by us, a tracheotomy was not necessary in any case, thanks to an early surgical intervention during the first days of life. The postoperative use of topical corticosteroids and topical mitomycin C remains controversial. We used topical corticosteroids, e.g., to prevent an increased granulation or scar formation in association with an inflammatory reaction [18, 19]. Due to its unclear advantages and the detection of its carcinogenic properties, Mitomycin C is no longer recommended [7, 21]. Hence, we did not use it. The initial endoscopic success rate varies widely in the literature and is said to be between 62% and 85.2% [9, 22]. Some studies consider it to be significantly lower [7]. Statistically, the use of stents cannot be associated with a significantly better outcome (e.g., 65% primary success rate for postoperative stenting vs. 64% primary success rate without stenting by Stychowsky et al.) [2, 21].
Stent-associated complications (epistaxis, discomfort and dislocation, infection, granulation, ulcerations, necroses of the columella and the nasal septum, vestibular stenoses) prevail over the cost-benefit considerations, so that their use can no longer be recommended [19]. In association with CHARGE syndrome, however, revision surgery is used more frequently. It is unclear whether the use of stents is preferable [9]. Generally, the duration and form of stenting should be considered. In particular, short-term stenting (<7 days) seems to have a more promising patency probability ratio (82%) compared to long-term stenting (up to 16 weeks) (60%) [9]. The complication rate of the shorter variant is comparable with the lack of stenting [9]. Basically, soft intubation tubes can serve as stents. They are introduced transnasally using the Seldinger technique and can either prevent slipping into the nasopharynx as a U-shape below the columella (Fig. 4b) or a dislocation out of the nose as a U-shape along the posterior edge of the vomer. If the risk of dislocation is considered low, we used two unconnected individual stents that can be sufficiently secured over the bridge of the nose. Overall, there was a postoperative tendency towards a shrinking of the choanal opening. As it could be observed that there was a clear restenosis tendency within the first six months without any nasopharyngeal stent or after its removal, we recommend the individual consideration of short-term stenting in children with CHARGE association. The insertion time and tube size can be easily adjusted during the endoscopic control examinations. The daily use of nasal saline irrigations, regular suctioning, and second-look examinations are obligatory [7, 19] and could replace stenting if meticulously applied [17]. Training the parents in the handling of these measures, including self-bouginage with the tube, is an integral part of our aftercare.
Conclusion
Bilateral choanal atresia is a life-threatening situation requiring acute measures. The treatment of choanal atresia aims at curative therapeutic strategies. The current therapeutic trend goes towards transnasal endoscopic resection, and the primary intervention should be minimally invasive, one-stage surgery, functional, and associated with low complication rates. Patency can be increased by saline irrigations, endoscopic controls, and regular bouginage. The insertion of stents is controversially discussed but can be useful in syndromal patients. However, adjuvant therapy with a stent and mitomycin C is increasingly being abandoned. A significantly higher recurrence rate must be expected in association with CHARGE syndrome. Here, stenting should be considered on an individual basis. Continuous training and support of the parents are obligatory.
Authorship contribution
TS & TK collected data, wrote the manuscript. DB & TK & TS analyzed data, MJ proofread, TS & AM & TD & FB treated and recruited and examined the patients, provided graphical material and proofread, TS & TK initiated the project.
Conflict of interest
No conflict of interest.