
Abstract
BACKGROUND:
Therapeutic hypothermia reduces mortality and neurological injury for neonates with hypoxic ischemic encephalopathy (HIE). The aim of this meta-analysis is to evaluate use of servo-controlled devices during transport to the referral hospital.
METHODS:
PubMed and Medline (Ovid) searches were used to identify studies comparing HIE patients’ temperatures on arrival
RESULTS:
Eight published studies with total of 573 patients met the inclusion criteria, with a “B” grade of recommendation overall. A significantly higher proportion of infants cooled with a servo-controlled device arrived in the target temperature range (pooled relative risk = 2.47, 95% confidence interval: 1.46–4.17, p < 0.001). The arrival temperature in the device cooled group was on average 0.82°C lower (95% CI: 0.29–1.35°C, p = 0.002) with an 82% lower temperature variance.
CONCLUSIONS:
Although the predominance of observational studies and presence of some risks of bias somewhat limits the strength of recommendation, the existing research consistently indicates that using a servo-controlled device during transport of neonates with HIE increases the probability of arriving at the referral hospital in the target temperature range, with a lower body temperature and less variability. Future research is needed to investigate differences in mortality and neurological impairment.
Keywords
Abbreviations
\begin tabbing CI Confidence interval\\ HIE \\ greaterthan Hypoxic ischemic encephalopathy\\ RE \\ greaterthan Random effects\\ RR \\ greaterthan Relative risk or risk ratio\\ TH \\ greaterthan Therapeutic hypothermia \end tabbing
Introduction
Occurrence of hypoxic ischemic encephalopathy (HIE) in neonates brings high risk of neurological impairment or death. Therapeutic hypothermia (TH) is the standard of care for patients with moderate to severe HIE. A meta-analysis of seven randomized controlled trials comparing TH to normothermia for newborns with HIE showed that TH reduced the risk of death or major neurological impairment at 18 months by 33% [1]. But TH is only available at specialized neonatal intensive care units (NICUs), so transfer to a higher level neonatal intensive care unit (NICU) is needed for most infants experiencing HIE who are born at hospitals with lower level NICUs [2].
Prompt initiation of TH is essential for preventing neurological disability [3] so providing this treatment during transportation of the infant to the referral hospital should be done whenever possible. Servo-controlled devices (e.g., Blanketrol, and CritiCool) which operate based on the patient’s temperature, have become available in recent years for use during transportation to the referral hospital. Servo-controlled devices compare the patient’s measured temperature to a value specified by the physician. If the patient’s temperature is above the physician-specified value, the water in the servo-controlled device will be cooled to reduce the patient’s temperature. Otherwise, if the patient’s temperature is below the specified value, the water in the servo-controlled device will be heated to increase the patient’s temperature. Hospitals that do not have devices for cooling during transport can instead use passive cooling (disconnecting all external heat sources) or active cooling with cold packs.
Numerous studies have been conducted to compare cooling with and without a servo-controlled device but no meta-analytic synthesis of these studies exists. The purpose of this study is to perform a meta-analysis to compare infants’ body temperatures on arrival at the referral hospital when cooled with a servo-controlled device versus without a device during hospital transfer. Specifically, the three objectives of this study were to conduct a meta-analysis of observational, quasi-experimental and experimental studies in order to compare a servo-controlled device to no device during transport of neonates with HIE to the referral hospital in terms of: 1) the proportion of infants arriving in the target (33–34 °C) temperature range, 2) the mean arrival temperature, and 3) the variability in the arrival temperature.
Methods
Literature search, screening and data extraction
Institutional Review Board approval for this study was not required since no patients were enrolled and individual patient records were not examined. Although no review protocol was registered for this meta-analysis, the 27 items in the PRISMA Statement were addressed [4] (Supplemental Figure 1). The author performed the literature search, screening and data extraction. All studies published in any language, whether observational, quasi-experimental or experimental (i.e., randomized controlled trials), that compared the body temperatures of neonates cooled with a servo-controlled-device vs. cooled without a device during transportation from the birth hospital were eligible.

Literature search and record screening results.
The inclusion criteria restricted the meta-analysis to studies comparing HIE patients’ temperatures on arrival for those cooled with servo-controlled devices versus no device during transport from the birth hospital. A PubMed (1946-2020) search was performed using the MESH terms “infant” and “hypothermia” (with corresponding text word synonyms) and the text word “transport”. The resulting publications were then screened to exclude studies not comparing the body temperatures of neonates with HIE treated with servo-controlled device assisted cooling vs. cooling without a device after transportation from the birth hospital. Initially the titles and abstracts were examined to see if the publication was relevant to the meta-analysis. Those appearing to potentially meet the study inclusion criteria were further screened by examining the full text article. A Medline (Ovid) all fields search of the terms “((infant or neonate) and hypothermia and transport)” was also done. (The original literature search was performed in January 2019, but the two databases were checked again in March of 2020 to identify any new records. The consort diagram in Fig. 1 displays the combined results of the initial search and the updated search.) When a study was identified that met the inclusion criteria for this meta-analysis, the reference list was examined in an attempt identify any additional potentially eligible studies, including non-published studies or studies that might have been missed by the literature search due to the journal not being indexed by PubMed or Ovid.
For studies meeting the inclusion criteria of comparing servo-controlled devices to no device during transport of the neonate with HIE to the referral hospital, data extraction forms were completed in order to collect relevant information. Variables for which data were sought for each study in the meta-analysis included study design (retrospective cohort study, quasi-experimental or randomized controlled trial), level of evidence (according to the guidelines provided by The Oxford Centre for Evidence-based Medicine at www.cebm.net), risk of bias, study patient inclusion criteria, patient gestational ages, main study findings, number of centers included in the study, nationality of study, start and stop time of patient enrollment, sample size for each group, number within the target temperature range on arrival for each group, mean temperature on arrival for each group, and standard deviation of temperature on arrival for each group. Corresponding authors of three studies that appeared to collect data on at least one of the three meta-analysis outcomes but not report the results needed in the publication were contacted to request the missing information. The corresponding author for [5] provided the group means and standard deviations of temperature on arrival needed for the comparison of means and comparison of variances, but the corresponding author for [6] did not respond to a request for this information. The corresponding author of [7] did not reply to an email request for the number with body temperatures over 34° C needed to ascertain the group proportions in the target temperature range for that study.
The publications meeting the inclusion criteria were assigned a level of evidence assessed using the guidelines provided by The Oxford Centre for Evidence-based Medicine [8]. The author performed an unblinded assessment of the risk of bias for each of the 8 studies meeting the meta-analysis inclusion criteria. The Newcastle-Ottawa Scale [9] was used to assess the risk of bias in the 7 non-randomized studies while the RoB 2 tool [10] was used to assess the randomized controlled trial [11]. The risk of bias assessments were not incorporated into the quantitative analysis, but the information is provided in conjunction with the level of evidence so that readers can make informed interpretations of the meta-analysis results. Additionally, ad hoc sensitivity analyses were performed to see if interpretations of results for the primary outcome changed when [12] and [6] were excluded from the RE model due to differences in the composition of the control group (mostly cooled with adjuvants) and outcome definition (ever in target temperature range before admission to the unit), respectively.
The primary outcome compared for servo-controlled device assisted cooling vs. cooling without a device in this meta-analysis was being in the target temperature range (33–34°C) on arrival at the receiving hospital, with risk ratios (relative risks, RR) used as the summary measure. Meta-analytic methods were also used to compare the mean temperature and variability in temperature when arriving at the receiving hospital between the two groups, as summarized by the difference in means and log variance ratio, respectively.
Statistical analysis
A meta-analysis was performed to compare treatment with a servo-controlled device vs. cooling without a device in terms of the dichotomous outcome of being within the target temperature range of 33–34°C upon arrival at the receiving hospital, in addition to the continuous outcome of the temperature on arrival at the receiving hospital for studies providing the mean and standard deviation of the temperature for both groups.
For the temperature in target range and mean temperature outcomes, random effects (RE) models with DerSimonian and Laird [13] estimation were used to test for an association of cooling with versus without a servo-controlled device, while Cochran’s Q test was used to test for significant between-study heterogeneity. To assess consistency of results across studies, the I2 statistic was computed to quantify the percentage of variation in the outcome across studies above that expected due to random sampling variation. Forest plots were used to summarize RE model results across studies. A funnel plot and Egger’s test were used to investigate potential publication bias. Additionally, aspects of study design, outcome definition used and composition of the no device group were considered when assessing bias across studies. An a priori decision was made to use RE models, instead of fixed effects, to obtain pooled results because the results were obtained from different study designs (i.e., observational, quasi-experimental and experimental), with some differences in treatments across studies (e.g., cooling with ice packs or passive cooling in the no device group) and outcome definitions (e.g., temperature in the target range upon arrival at the receiving hospital for five studies versus one hour after initiation of cooling for one study and ever in the target temperature range before admission to the unit for another study). A meta-analysis using the log variance ratio (lnVR) to compare the variability in body temperature upon arrival at the referral hospital for the servo-controlled device versus no device group was performed by the method described by [14] using the R code from the data repository provided by [15]. R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria) was used for data analysis. The “rma” function was used to fit RE models for the temperature in target range and mean temperature upon arrival outcomes and the “rma.mv” function was used for the temperature variance outcome. The “metaphor” package was used to generate forest plots and funnel plots and the “regtest” function was used to apply Egger’s test for publication bias.
Results
The PubMed search yielded 101 records and the Medline (Ovid) search yielded 146 records. After removing 93 duplicate records, the abstracts and titles of 154 articles were perused to identify studies comparing cooling with versus without a servo-controlled device, with 19 articles warranting full text review to assess eligibility. Ultimately, eight published studies [2, 17] were found that met the meta-analysis inclusion criteria, with none of the 164 articles referenced by these eight studies found to be additional studies meeting the meta-analysis inclusion criteria. Of the eight studies included in the meta-analysis, seven were analyzed to compare the proportion of patients in the target temperature range on arrival at the receiving hospital, and four were analyzed to compare the mean and variability of temperatures on arrival (Fig. 1).
Of the eight studies included in the meta-analysis, with publication year ranging from 2011–2019, five were retrospective cohort studies, two quasi-experimental and one randomized controlled trial (Table 1). In total there were 573 patients included in the meta-analysis, with 286 patients in the servo-controlled device cooling group and 287 in the no device group. Gestational ages were similar for the six studies reporting descriptive statistics for patient gestational age. There were four studies conducted in the United Kingdom and four studies in the United States. The beginning of patient enrollment ranged from April 2008 to January 2015 and the end of patient enrollment ranged from October 2009 to May 2016. Four of the studies involved multiple cooling centers to which neonates were transported. All studies had a 2b level of evidence except one study having 1b [8]. Descriptive statistics summarizing results for the studies included in the meta-analysis are provided in Table 2.
Characteristics of the studies analyzed
Characteristics of the studies analyzed
*Results for this outcome were obtained via personal communication with the corresponding author since they were not reported in the published article. †Oxford Centre for Evidence-Based Medicine (https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/).
Descriptive statistics for all studies’ outcomes
*Not reported.
Seven of the eight studies reported the proportion in the target temperature range for the two groups. (The corresponding author of [7] did not reply to an email request for information needed to compute the group proportions in the target temperature range for that study.) Six of the seven studies had a 2b level of evidence and one had 1b, providing a grade of “B” for the strength of evidence related to the proportion of patients in the target temperature range comparison. Infants cooled with a servo-controlled device were 2.47 times as likely to be in the 33–34° C target temperature range on arrival at the receiving hospital when pooling the results across all seven studies providing data for this outcome (RR = 2.47, 95% CI: 1.46 –4.17, Z = 3.4, p < 0.001, Fig. 2). There was not significant variation in the probability of being in the target temperature range across studies (I2 = 0.0%, Q = 1.4, df = 6, p = 0.968). Neither visual inspection of the funnel plot (Supplemental Figure 2) nor a formal hypothesis test (Z = –0.7, p = 0.466) indicated significant asymmetry, so publication bias does not appear to be a concern for this outcome.

Forest plot of risk ratios for being in the target temperature range when cooling with versus without a servo-controlled device.
Three of the eight studies reported the group means and standard deviations of arrival temperatures, and the corresponding author for [5] provided this information via email, so four studies were included in the comparison of mean temperatures on arrival. (Note that, although it appeared that they collected these data, no reply was received from an email to the corresponding author for [6] requesting group means and standard deviations of arrival temperatures.) All four studies had a 2b level of evidence providing a “B” grade for the strength of evidence for the comparison of mean body temperatures on arrival. The pooled results showed the arrival temperature in the servo-controlled device cooled group was 0.82°C lower (95% CI: 0.29–1.35°C, Z = –3.0, p = 0.002) on average compared to patients cooled without a device (Fig. 3). There was significant variation in the effect size across studies (I2 = 86.2%, Q = 24.3, df = 3, p < 0.001). There was not significant asymmetry in the mean temperature on arrival results so publication bias was not indicated for this outcome (Z = –1.1, p = 0.252, Supplemental Figure 3).
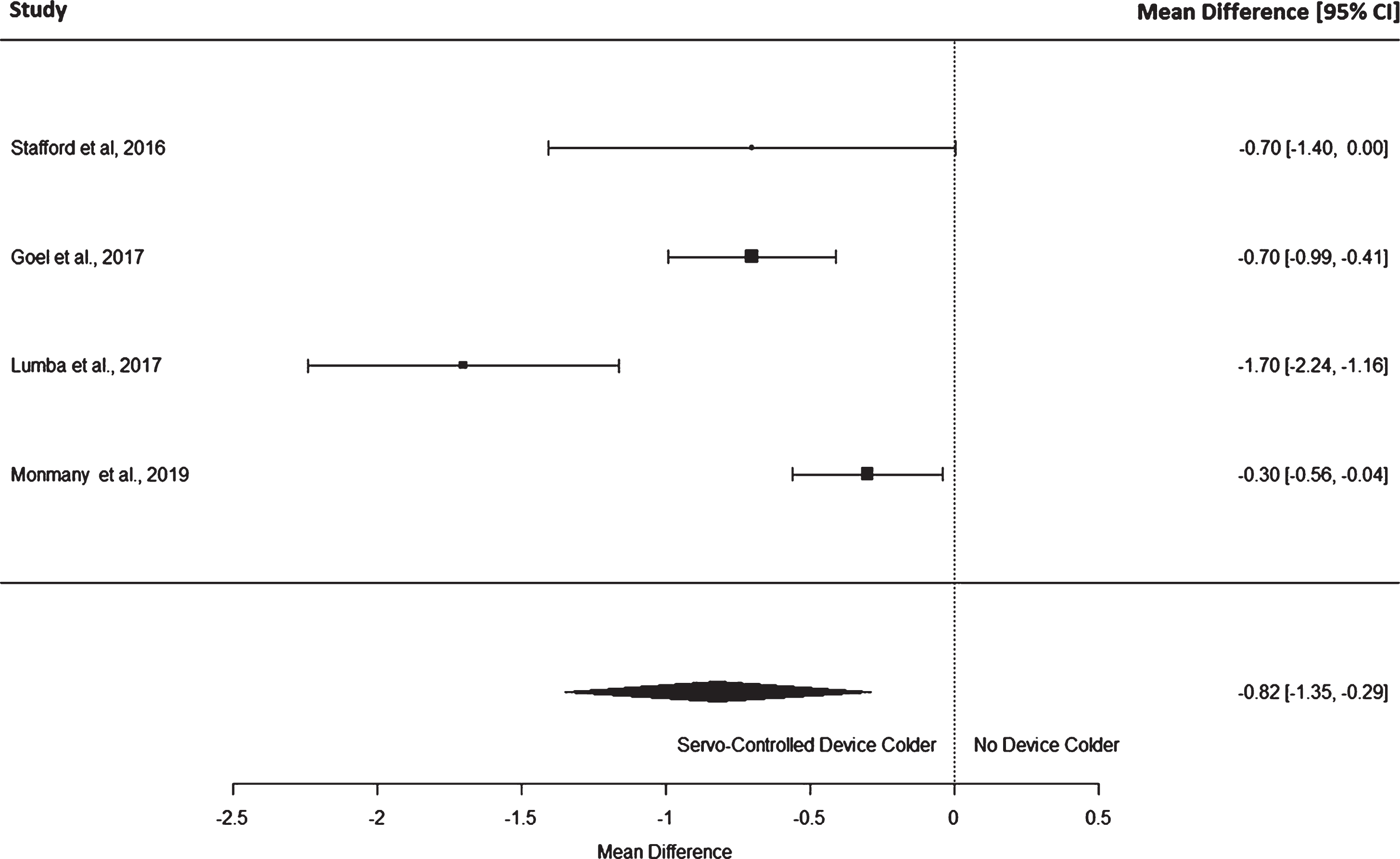
Forest plot of the mean differences in arrival temperatures for patients cooled with versus without a servo-controlled device.
The same 4 studies analyzed for the comparison of mean temperatures outcome (above) reported the results needed for the comparison of variability in temperature on arrival. Again, each of the 4 studies had a 2b level of evidence providing a “B” grade for the strength of evidence for this comparison. The variance in body temperature measurements on arrival at the referral hospital was 82% lower in the device group when pooled across studies (Z = –9.7, p < 0.001) in addition to being significantly lower for each of the four individual studies that reported standard deviations (Fig. 4). The weighted average variance (standard deviation2) of body temperatures on arrival across studies was 0.26 in the device group and 1.38 in the no device group. The log variance ratios (lnVRs) were homogenous across the four studies analyzed (Q = 0.8, df = 3, p = 0.846). The funnel plot of lnVRs did not indicate asymmetry that would be expected in the presence of publication bias (Supplemental Figure 4).
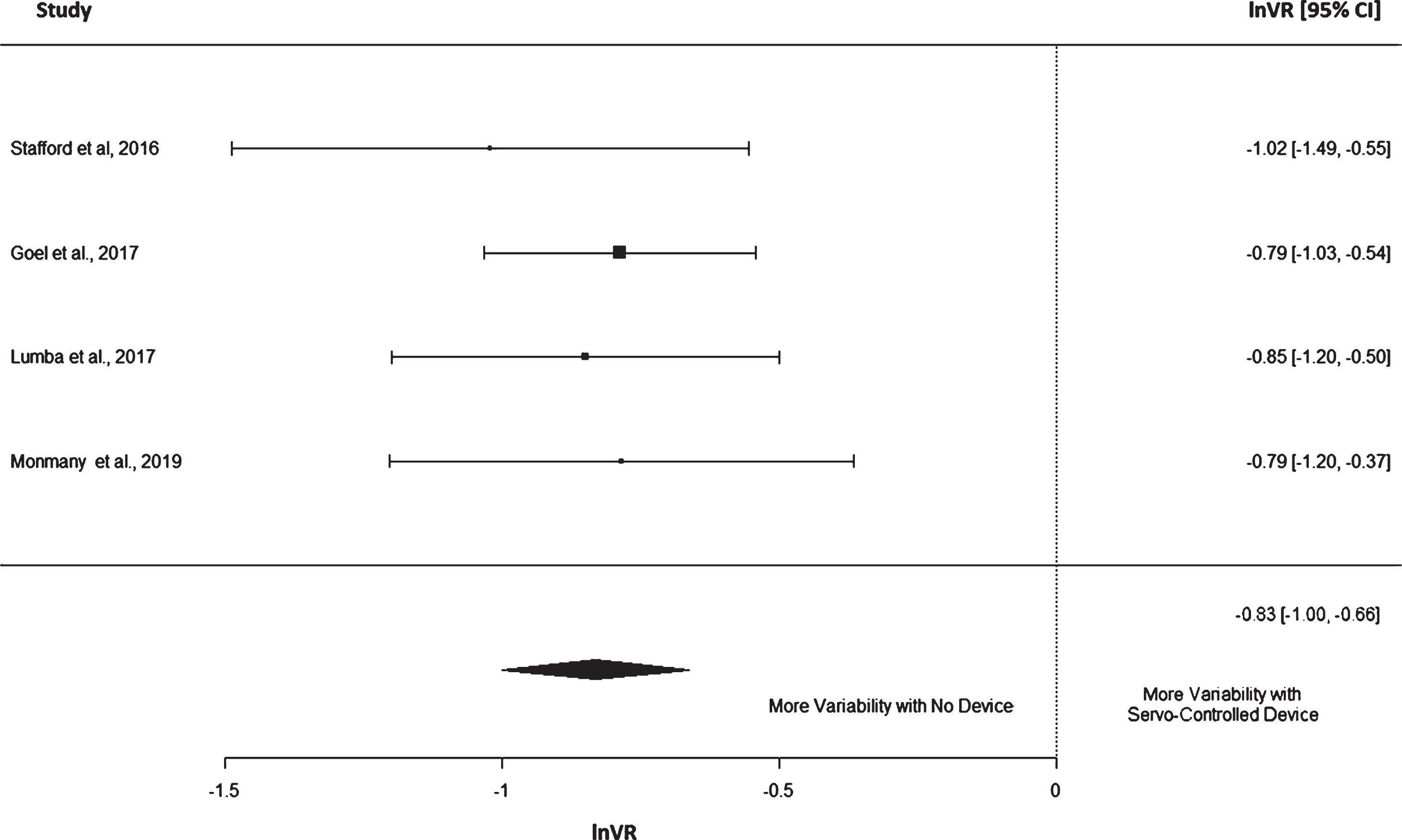
Forest plot of log variance ratios (lnVRs) for arrival temperatures of patients cooled with versus without a servo-controlled device.
Regarding risk of bias for individual studies, there were some concerns about missing outcome data in the randomized controlled study [11] because temperatures one hour after initiation of cooling were missing due to transport being completed before one hour for 8/49 = 16% of controls and 12/51 = 24% in the servo-device cooled group. However there were no concerns about bias related to the randomization process, deviations from the intended interventions, measurement of the outcome or selection of the reported results for this study (Supplemental Table 1). Only one of the seven non-randomized studies [2] controlled for potentially confounding covariates so “comparability of cohorts on the basis of the design or analysis” was a concern for the other 6 non-randomized studies (Supplemental Table 2).
When looking at the studies included in the meta-analysis, there are some methodological inconsistencies that should be considered when assessing concerns about bias across studies. For example, the primary outcome of interest is a dichotomous “arrival within the target temperature range” (yes/no), although two studies’ outcomes did not exactly fit this definition. For [11] the outcome “within temperature range 1 hour after initiation of cooling” was used instead of arrival temperature in range. Their outcome definition could actually be considered more desirable because it is standard (the same for every patient), which is a luxury resulting from their randomized controlled trial study design, whereas the other studies in the meta-analysis did not have access to such outcome data. For [6] a higher proportion of patients were in the target range in both groups because they assessed the outcome as ever achieving the target temperature (33–34°C) before admission to the receiving unit. In an ad hoc sensitivity analysis, results were nearly identical when the [6] study was removed from the RE model (RR = 2.52, 95% CI: 1.48–4.30, Z = 3.4, p = 0.001).
In addition to inconsistencies across studies in the outcome definition, there were inconsistencies in how the “no device” group was defined. Three of the eight studies mentioned some form of non-servo-controlled active cooling (e.g., ice packs) in a subset of patients in the “no device” arm, whereas the other five studies appeared to use strictly passive cooling in the no device arm since no mention of other cooling methods were mentioned (see Table 1 “Hypothermia Treatment in No Device Group” column for a description for each study). However the percentage of patients in the no device group who were exposed to non-servo-controlled active cooling during transport was small, with the exception of [12] in which 17/27 = 63% of these patients were exposed to “adjuvants” such as cold packs. The results from [12] were not included in the comparison of temperature mean or variability meta-analyses, and an ad hoc sensitivity analysis did not yield a different interpretation of the proportion in the target temperature range results when [12] was excluded from the RE model (RR = 2.59, 95% CI: 1.48–4.52, Z = 3.3, p = 0.001). Note that when an additional sensitivity analysis was performed removing both [12] and [6] studies due to concerns about the control group (mostly cooled with adjuvants) and outcome definition (ever in target temperature range before admission to the unit), respectively, the RE model analyzing the remaining five studies was consistent with the original analysis, showing a significantly higher likelihood of arriving in the target temperature range for patients in the servo-controlled device group (RR = 2.65, 95% CI: 1.50–4.70, Z = 3.4, p = 0.001). There could be differences in patient characteristics across studies that influence pooled estimates. For example, smaller infants would be more likely to exhibit temperature dysregulation. Although gestational ages were similar across the six studies reporting descriptive statistics for patient gestational age, the potential influence of other patient factors that differed across studies cannot be ruled out. But the finding that all of three of sensitivity analyses yielded results very similar to the initial RE model results, in conjunction with the value of zero for I2 and the non-significant Cochran’s Q test largely assuage concerns about inconsistencies between studies when interpreting pooled results for the proportion of patients in the target temperature range outcome.
Discussion
This meta-analysis shows that infants with HIE cooled with a servo-controlled device during transport from the birth hospital are more than twice as likely to arrive in the target temperature range, with a significantly cooler temperature and with significantly less variation in body temperature upon arrival at the receiving institution compared to infants for whom servo-controlled devices were not used. Looking at the point estimates of the summary measures for the patients in the target range, and mean temperature and standard deviation of the temperature on arrival at the referral hospital outcomes, every individual study analyzed provides some degree of evidence to support each of these three conclusions, but when the results are synthesized via meta-analysis the evidence is very convincing. Only the mean difference in the arrival temperature outcome displayed significant variation across studies, with [7] exhibiting a relatively extreme mean difference, despite no obvious study design or measurement anomalies.
Now that the superiority of cooling with a servo-controlled device during transport has been established in terms of these body temperature outcomes, the question is, how does this benefit the patient? The benefits of TH compared to normothermia are clear. As mentioned previously, a meta-analysis [1] showed that TH for newborns with HIE decreased the risk of death or major neurodevelopmental disability at 18 months of age by 33%. But the optimal temperature for TH is not well established. A study using a neonatal rat model of unilateral HIE [18] showed a U-shaped relationship between treatment temperature and area loss in the frontal cortex and mid- hippocampus, with minimal area loss occurring with treatment temperatures of 32°C to 33.5°C and loss increasing with temperatures above or below this range. Similarly, [19] found a U-shaped curve for the relationship between temperature and delayed brain cell death in newborn pigs with HIE, with the greatest reduction in delayed cell death occurring at 33.5°C to 35°C. A randomized clinical trial [20] did not find a benefit from deeper cooling to 32°C compared to 33.5°C. In addition to neurological complications being associated with temperatures outside the target temperature range, body temperature during TH has also been shown to be associated with other adverse outcomes such as coagulopathy [21], cardiovascular instability [22] and even death [23].
The importance of quickly starting TH with regard to mitigating neurological impairment has been demonstrated. [3] found that infants with perinatal asphyxia for whom TH was initiated within three hours after birth had a median Bayley Scales of Infant Development II psychomotor developmental index score of 90 compared to 78 when TH was initiated more than three hours after birth (p = 0.033). The randomized clinical trial [11] included in this meta-analysis showed that newborns with encephalopathy cooled with a servo-controlled device during transport to the receiving neonatal intensive care unit reached the target temperature within 44 minutes on average compared to 63 minutes when no device was used.
So taking these findings together, the servo-controlled devices cool patients faster and increase the probability that patients arrive in the target temperature range. Faster cooling and being in the target temperature range have been shown to be neuroprotective for HIE patients. Therefore, use of servo-controlled devices during transport to the referral hospital should provide neuroprotective benefits. But randomized controlled studies comparing neurological outcomes for TH with versus without servo-controlled devices are lacking. A quasi-experimental study [24] comparing 72 hours of servo-controlled cooling to manual cooling with ice packs found that the cooler rectal temperatures and higher probability of being in the target temperature range associated with servo-controlled cooling did not translate into a statistically significant difference in death or neurological disability, although the study was not powered to address this hypothesis.
Our finding that the variability in body temperatures is lower for device-cooled infants is consistent with previous research. Previous studies [25, 26] have found less variation in rectal temperatures of newborns cooled with servo-controlled devices compared to other modes of TH. The degree to which variation in body temperature influences the neuroprotective benefits of TH is largely unknown and should be the subject of future study.
Uncertainty in the degree to which the higher probability of achieving the target range with less variability in body temperature associated with servo-controlled device cooling translates into improved survival and neuroprotection precludes a formal cost-benefit analysis. Nevertheless, given that neonatal HIE is among the largest causes of disability globally, accounting for 10% of disability-adjusted life years, [27] even a relatively small reduction in mortality and neurological impairment would result in tremendous benefits at the societal level. The high cost of servo-cooling devices is a disincentive to more institutions using them during transportation of neonates with HIE. Lower cost devices for application of a full TH protocol have been studied [24, 28] but exploration of such alternatives during transportation of the neonate is an area in need of future investigation.
Risk of bias for individual studies is somewhat of a concern in this meta-analysis. A non-negligible percentage of patients in both treatment groups had missing outcome data in the one randomized controlled trial included. However this would only result in biased results if there are systematic differences in the groups’ probability of a missing outcome. There is no obvious reason why this would be true given that, for both groups, patients for whom transport times were less than one hour had missing arrival temperature data in this study. Only one of the non-randomized studies [2] attempted to address concerns about comparability of groups by controlling for the effects of potential confounders. In [2], the increased odds of being in the target temperature range associated with using a servo-controlled device was statistically significant both before and after controlling for potentially confounding covariates, although the magnitude of this association increased substantially when covariates were adjusted for. Taking this into consideration in conjunction with the observation that the randomized controlled trial [11] showed the greatest increase in likelihood of being in the target temperature range among the seven studies reporting this outcome suggests that potential confounding might have biased results toward the null hypothesis of no difference in the groups’ proportions of patients arriving in the target temperature range. Relative risks across the seven studies are fairly consistent, with all having point estimates greater than one indicating higher odds of being in the target temperature range in the servo-controlled device group, with all studies’ relative risks falling in the 1.35 to 3.68 range. Despite the consistency across studies for the proportion arriving in the target temperature range outcome, the I2 statistic and Cochran’s Q test results indicated substantial heterogeneity in the mean temperature on arrival outcome across studies. Examination of the four studies analyzed for this outcome reveals a relatively extreme mean difference of –1.7 degrees for [7] compared to consistent results of –0.7, –0.7 and –0.3 degrees for the other three studies. There is no obvious difference in study design or measurement that would cause a larger difference for [7], and the observation that the direction of the mean difference is consistent with the other studies provides some assurance that interpretations are correct for the pooled results showing a significantly lower mean arrival temperature in the servo-controlled device group.
Although publication bias does not appear to be an issue, study limitations include combining observational, quasi-experimental and experimental studies for this meta-analysis. Ideally, all studies included in a meta-analysis would be randomized controlled trials, but only one such study comparing cooling with versus without a device has been published. The preponderance of observational studies on the topic only accentuates the need to synthesize results across all available studies in order to derive a coherent conclusion regarding the relative benefits of cooling with a servo-controlled device. Despite the fact that the quality of the studies does not yield the strongest possible evidence, the consistency of the findings across studies and outcomes facilitates the clear interpretations that cooling with a servo-controlled device increases the probability of arriving in the target temperature range with a lower body temperature on average, and with less variability in arrival temperatures. Although these findings can assist health care providers and hospital administrators in weighing the benefits versus cost to decide whether or not to purchase such a device for their institution, future randomized studies that include long-term neurological assessment are needed to fully evaluate the impact of servo-controlled cooling. All of the published studies to this point that were available for meta-analysis only compared short-term outcomes, so the effect on long term morbidity is unknown.
In conclusion, the published research consistently shows that newborns with HIE who are cooled with a servo-controlled device during transport to the receiving hospital are more likely to arrive within the target temperature range, with cooler temperatures and having less variability in temperatures. The degree to which cooling with a servo-controlled device during transport translates into a reduction in mortality and neurological morbidity requires future investigation, preferably using a randomized controlled study design to assess long-term neurological assessment.
Disclosure of funding
No funding support was received for this research.