
Abstract
Postnatally acquired cytomegalovirus (CMV) is commonly acquired via breast milk, with premature infants more frequently developing symptoms of CMV infection in comparison to term infants. Meningitis is a rare clinical manifestation of CMV infection. The diagnosis of meningitis is difficult to make in infants, particularly those who are preterm. Consequentially, broad-spectrum empiric antimicrobial coverage is often administered for several days while waiting for current gold standard CSF testing to result. The BioFire FilmArray (BFA) simultaneously tests for 14 different pathogens, including CMV, allowing for quicker diagnosis and shorter time to definitive treatment. Here, we report a very low birth weight infant with postnatally acquired CMV meningitis, the first to our knowledge to be diagnosed using the BioFire FilmArray.
Abbreviations
Cytomegalovirus BioFire FilmArray Cerebrospinal fluid Gestational age Day of life Polymerase chain reaction Aspartate aminotransferase Alanine aminotransferase
Introduction
Postnatal CMV in preterm infants is usually acquired via breast milk, with an annual rate of up to 30% of very low birth weight infants who were fed untreated breast milk [1]. Additional modes of perinatal transmission include genital secretions during birth, blood transfusions and horizontally by close contact [2]. Approximately 96% of sero-positive women will have reactivation of the virus in breast milk within several days following delivery [3]. In preterm infants, postnatal CMV can manifest as a variety of clinical presentations, including thrombocytopenia, sepsis, hepatitis, anemia, lymphocytosis, cholestasis, pneumonitis, colitis, and meningitis [2, 5]. However, diagnosis, particularly meningitis, can be challenging in this population [6].
The BFA is an in vitro diagnostic test designed to expedite diagnosis from cerebrospinal fluid (CSF) samples [7]. The BFA is able to detect fourteen different pathogens, including CMV, enterovirus, herpes simplex viruses 1 and 2, human parecho-virus, varicella-zoster virus, Escherichia coli K1, Haemophilus influenza, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae, and Cryptococcus neoformans/Cryptococcus gattii from CSF samples [7]. Turnaround time for BFA ranges from one to three hours, which is shorter than standard cultures that typically result 24–48 hours after collection [8–10]. Sensitivity and specificity of BFA is 100% and 99.8%, respectively [7]. Use of the BFA, especially in clinically uncertain cases, can significantly reduce unnecessary broad empiric antibiotic coverage and expedite definitive therapy [7, 10].
Case presentation
A symmetric, appropriate for gestational age (GA), singleton female was born at 26 weeks GA via vaginal delivery to a gravida four, para four 41year old Hispanic woman. The pregnancy was complicated by intrauterine growth restriction, severe pre-eclampsia and fetal bradycardia. Apgars were 2, 5, and 7 at 1, 5 and 10 minutes of life, respectively. Weight at birth was 700 g (26th percentile), length was 33 cm (47th percentile) and head circumference was 21.8 cm (12th percentile). She was intubated at five minutes of life and given surfactant in the delivery room. She was immediately started on synchronized intermittent mechanical ventilation and caffeine. A second dose of surfactant was given on day of life (DOL) two. She was first extubated on DOL eight. CMV saliva polymerase chain reaction (PCR) was negative on DOL two. Microcephaly was noted within the first week of life (Fig. 1). While routine head ultrasound on DOL seven was unremarkable, head ultrasound on DOL 30 was notable for ventriculomegaly (Fig. 2).
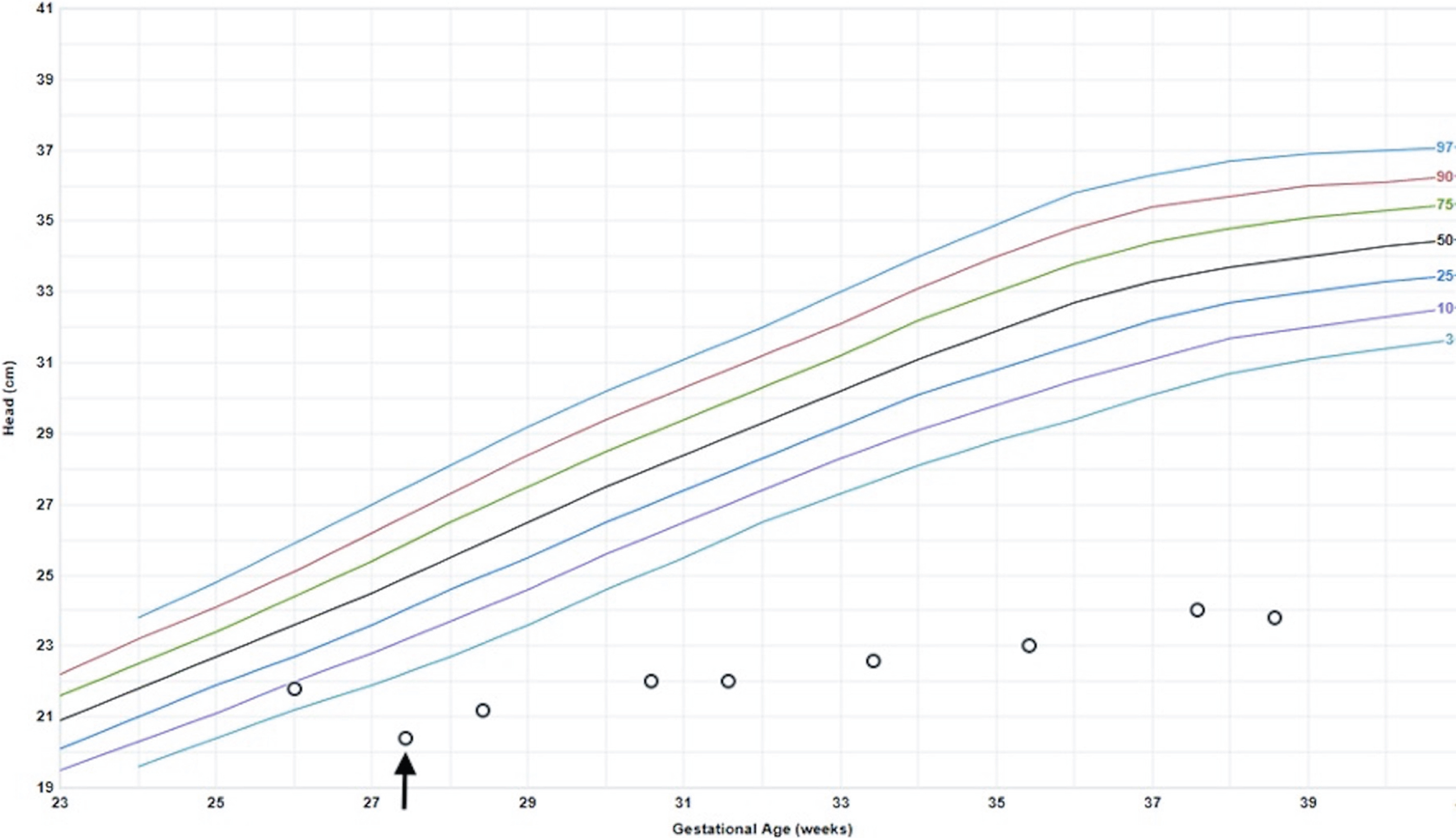
Olsen Premature Girls head circumference. The infant was born with a head circumference in the 12th percentile and was microcephalic thereafter. The arrow points to her DOL 7 head circumference.
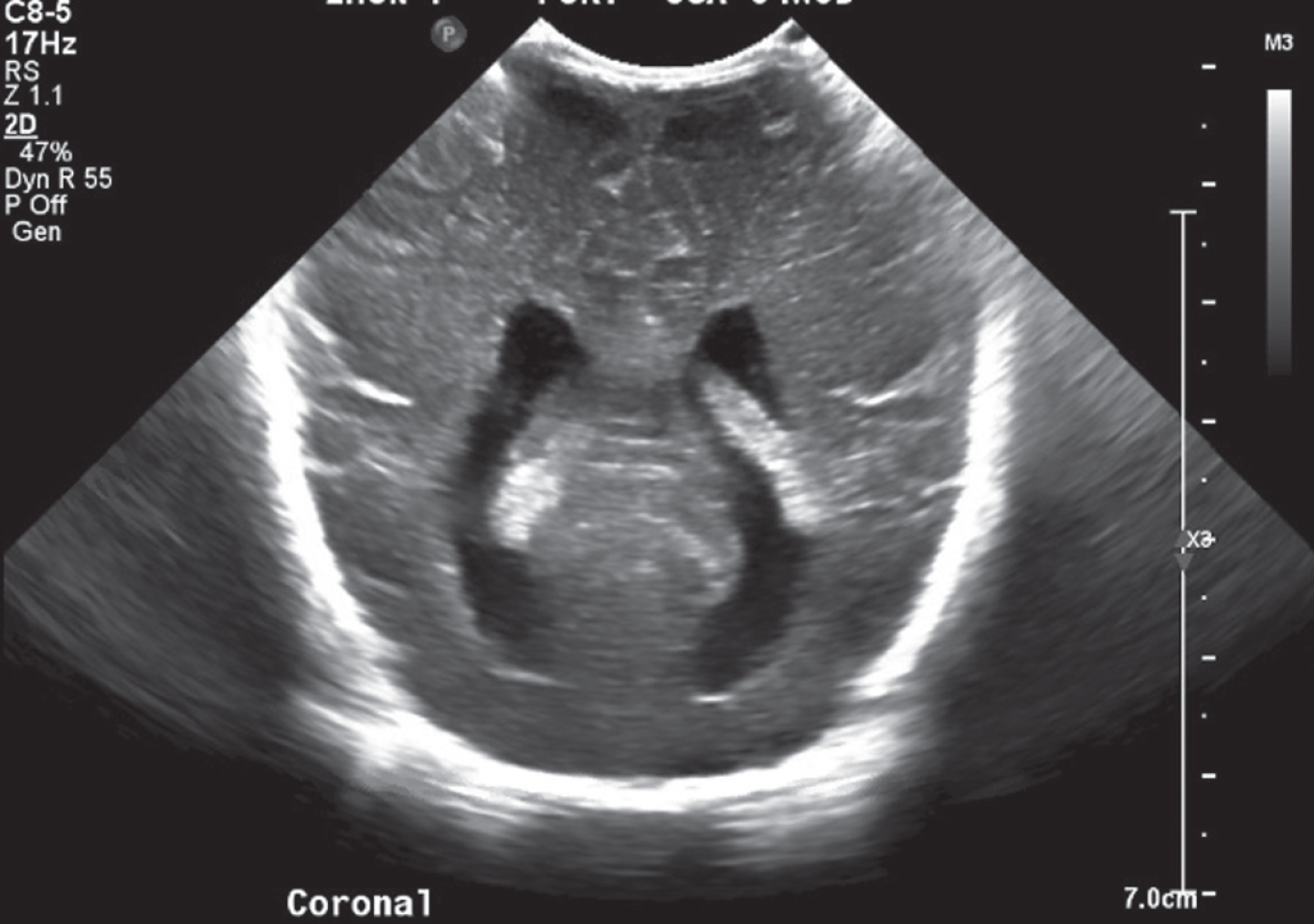
Head ultrasound showing significant ventriculomegaly on DOL 30.
After being stable on high flow nasal cannula by DOL 37, the infant was reintubated due to persistent apneic events, bradycardia and desaturations on DOL 54. Chest x-ray was notable for heterogeneous pulmonary opacities suggestive of atelectasis and edema superimposed on previously identified evolving chronic lung disease (Fig. 3). Liver enzymes were elevated with aspartate aminotransferase (AST) of 307 U/L and alanine aminotransferase (ALT) of 191 U/L. She was empirically started on a sepsis rule-out with vancomycin, gentamicin and fluconazole later that same day (DOL 54). Two days after the decompensation, AST and ALT levels peaked to 482 U/L and 308 U/L, respectively, on DOL 56. Thus, an abdominal ultrasound was performed and revealed cholecystolithiasis and sludge without sonographic evidence of cholecystitis. Her platelet count, initially 352,000 10∧9/L on DOL 38, decreased to a nadir of 42,000 10∧9/L on DOL 57. She remained thrombocytopenic until DOL 69 (Fig. 4).
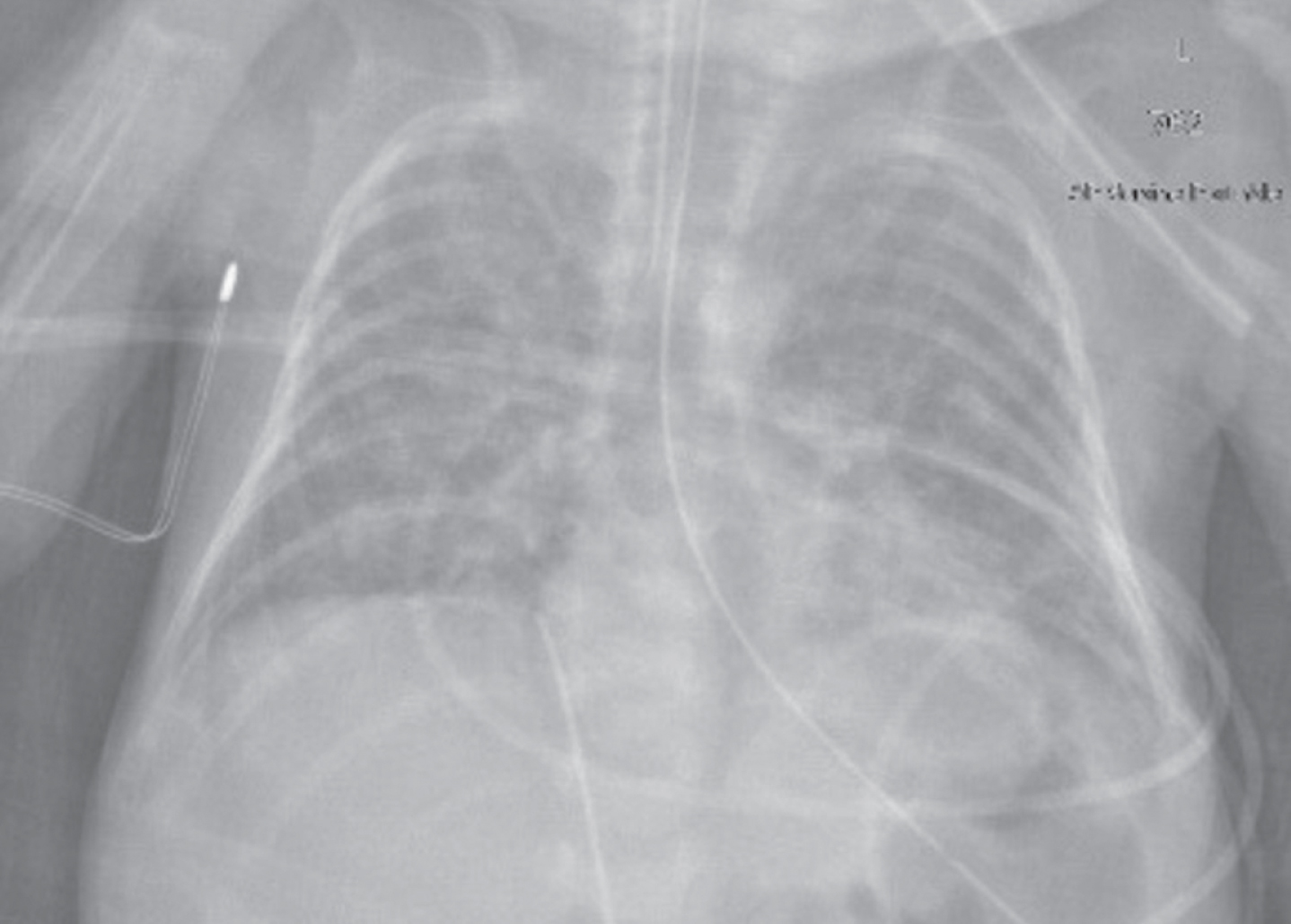
X-ray of the chest on DOL 54 showing ongoing chronic lung disease and pneumonitis. Infant was able to be extubated on DOL 58 and weaned completely off respiratory support on DOL 202.

Platelet count demonstrating thrombocytopenia. After reaching a nadir of 42,000 on DOL 57, platelet count began to recover with treatment.
Due to further clinical deterioration, a lumbar puncture was performed on DOL 58. CSF showed glucose of 51 mg/dL, protein of 37 mg/dL, nucleated cell count of 3 per uL (68% lymphocytes, 10% variant lymphocytes, 2% macrophages, 9% monocytes, 2% neutrophils), and 620 per uL red blood cells. CSF culture showed no organisms and rare WBCs. Additional lab results are detailed in Fig. 5. The BFA resulted positive for CMV within two hours of CSF analysis. CMV saliva PCR was sent one day prior to LP (DOL 57) but resulted positive two days after the BFA results were returned. The infant was immediately started on IV ganciclovir and discontinued off empiric antibiotic and antifungal therapy. Serum CMV PCR viral load was 476,000 IU/ml at initiation of therapy and demonstrated a downward trend with therapy. She was monitored weekly for adverse effects of ganciclovir, including neutropenia and liver dysfunction.

Additional laboratory analysis taken the day of LP.
Despite developing CMV pneumonitis requiring prolonged respiratory support and enterocolitis with feeding intolerance, she was extubated on DOL 58 and worked up to full enteral feeds by DOL 132. Repeat ultrasound of the gallbladder on DOL 142 showed no cholelithiasis and alkaline phosphatase on DOL 176 was mildly elevated at 473 U/L. She passed two hearing screens, and a brain MRI on DOL 139 showed no evidence of parenchymal calcifications or re-demonstration of ventriculomegaly (Fig. 6). She was transitioned to valganciclovir once she reached full feeds on DOL 132 for a total of six months of antiviral therapy. CMV viral load was undetectable prior to finishing treatment.
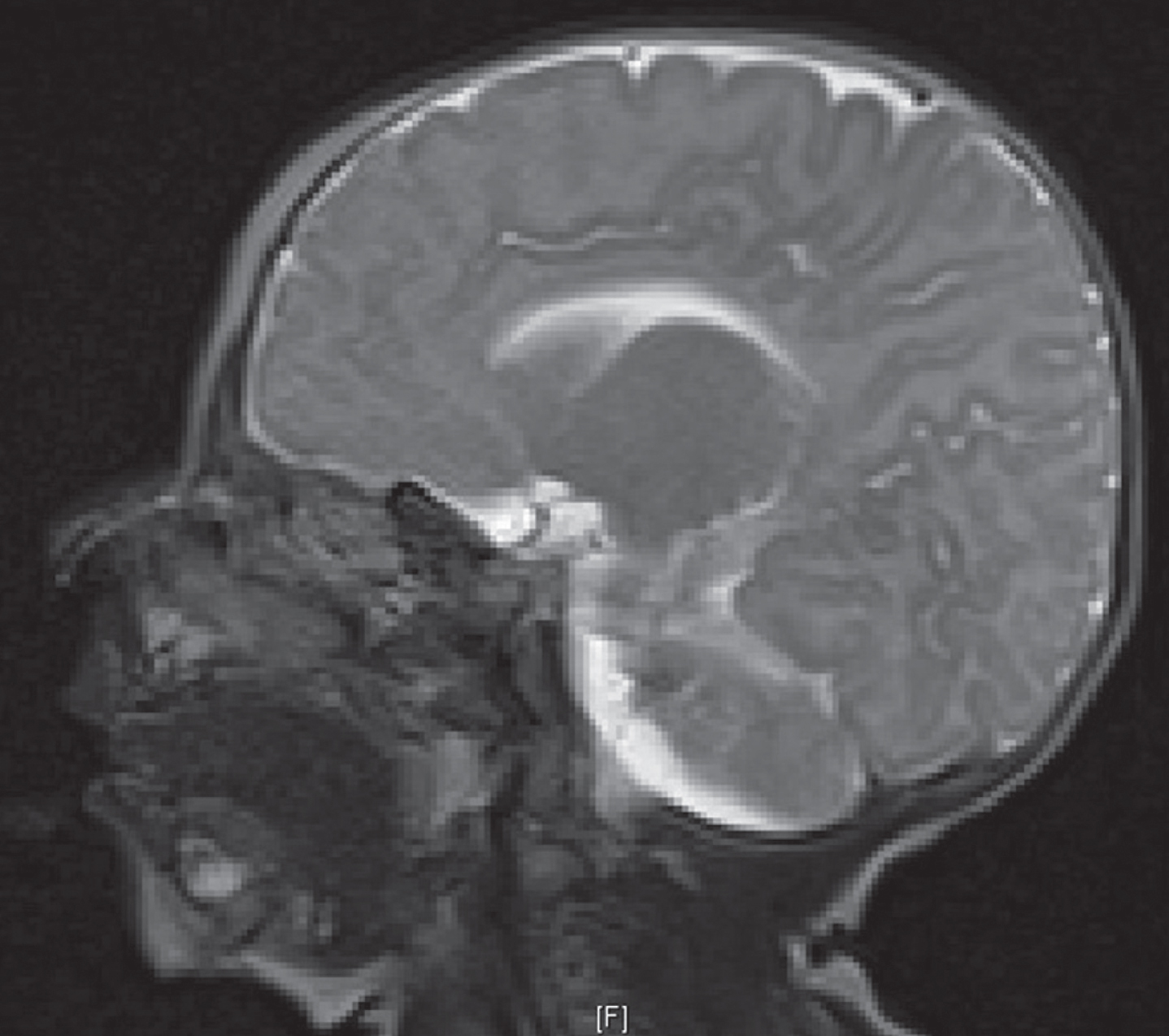
MRI of the brain with and without contrast, performed on DOL 139, approximately three months after initiation of antiviral treatment. Although parenchymal calcification is typically seen in CMV meningitis, it was not seen in this infant.
At her one-year follow-up, physical exam was notable for moderate generalized hypotonia and mild head lag. She was able to roll to both sides, reach for and transfer objects, turn her head to noise, smile, track, sit with support, and bear weight on legs with support. She is receiving weekly physical, occupational and speech therapy. She has no respiratory support requirements. Anthropomorphic measurements were notable for a head circumference in the less than 1st percentile, weight in the 2nd percentile, and length in the less than 1st percentile. She failed her hearing screen at one year of age with concern for conductive hearing loss due to lack of bilateral tympanic mobility and largely absent bilateral otoacoustic emissions, requiring placement of bilateral tympanostomy tubes.
To our knowledge, this is the first reported case of an infant diagnosed with postnatally acquired CMV meningitis via BFA. Postnatal CMV is typically acquired via breast milk, and while symptoms are more likely to manifest in VLBW infants, diagnosis of meningitis remains challenging. Freezing and pasteurizing breast milk to reduce the burden of CMV remains controversial. Freezing reduces, but does not eliminate, the rate of postnatal CMV, and pasteurization can prevent CMV transmission, but both processes reduce transmission at the expense of decreasing the immunological and nutritional quality of breast milk [1, 3]. Additionally, adequate storage temperature and required length of time for freezing to maximally reduce CMV is unknown [1]. In our case, transmission was assumed to be postnatal as the infant’s CMV saliva was negative shortly after birth. Urine PCR was not done near birth, thus, there is a chance, albeit very unlikely, that congenital CMV was missed [11]. Although sensitivity and specificity of CMV saliva testing has not been established in preterm infants, in term infants it is 100% and 99.9%, respectively [12]. The infant was clinically stable prior to decompensation, with normal head circumference, platelet and AST/ALT levels at birth, making a false negative less likely. Maternal CMV status was unknown, and the infant had received maternal breast milk and multiple red blood cell transfusions.
Meningitis is a difficult diagnosis to make in the neonate, as classic meningitic signs, including bulging fontanelle and seizures, are often not seen until late in the disease course [6]. Early signs of men-ingitis, including apnea, bradycardia, lethargy and temperature instability in neonates are often non-specific and have a broad differential [6, 7]. Additionally, the degree of prematurity and variability in meningitic signs by birthweight and oftentimes initial normal cell count on testing adds to the complexity of diagnosis [6, 7]. Although initial cellular and chemistry panels may strongly suggest what type of meningitis is suspected (i.e. bacterial versus fungal versus viral), these results are not specific [7]. Postnatal CMV in preterm infants can present with multisystem involvement, most notably with thrombocytopenia, sepsis, and hepatitis, but can also include anemia, lymphocytosis, cholestasis, pneumonitis and colitis [2, 13]. Preterm infants are at higher risk proportional to their degree of immaturity secondary to their lack of protective maternal antibodies that are typically transferred during the third trimester [4]. Our infant showed evidence of thrombocytopenia, hepatitis, cholestasis and pneumonitis. However, given that these clinical findings are often nonspecific, she was started on empiric antibiotics for four days prior to lumbar puncture and BFA testing. Of note, initial CSF cell count was not clearly indicative of meningitis. Upon return of BFA results, empiric antibiotic and antifungal therapy were discontinued, and she was transitioned to definitive antiviral therapy with ganciclovir.
The BFA provides much promise to neonatal care as conventional methods of testing often require significant CSF volumes that are oftentimes not available in neonates [7]. Additionally, the BFA has potential for increased target detection in addition to significant cost reduction [14]. Given that the BFA has only been recently introduced to clinical practice, much research has been conducted to evaluate its accuracy [7, 16]. Notably, none of the testing was conducted in preterm infants, thus data must be extrapolated for this unique population [7, 16]. Sensitivity for the BFA ranges from 57.1–100% while its specificity ranges from 99.8–100% [7, 15]. A meta-analysis detailing the accuracy of the BFA calculated its false positive rate at 5.6% and its false negative rate at 100% [16]. The wide diversity, particularly in published reports of the BFA sensitivity, and poor false positive and false negative rates is likely secondary to the incredibly small number of meningitic patients infected with CMV. Given our patient’s clinical presentation consistent with CMV and BFA positivity, we did not feel that confirmatory testing with PCR was required at the time of diagnosis.
Indications for treatment of postnatally acquired CMV are commonly cited to treat the acute illness and potentially reduce the morbidities associated with CMV, such as bronchopulmonary dysplasia and neurodevelopmental impairment [17–19]. Although postnatally acquired CMV is not typically associated with sensorineural hearing loss as is congenitally acquired CMV, recent reports have suggested an increased risk of hearing screen failure in infants with postnatally acquired CMV at discharge [20]. Long-term studies have indicated that although preterm infants with postnatally acquired CMV initially show normal neurodevelopmental status, beginning at approximately age six years, significant differences are observed [21, 22]. Additionally, IQ scores in adolescents are significantly decreased in comparison to their preterm peers without infection, particularly in males [23]. There are currently no clear guidelines regarding which infants should receive treatment for postnatally acquired CMV, nor for the duration of treatment. However, symptomatic CMV infection, particularly meningitis, warrants serious consideration for treatment with antivirals. Active agents against CMV include ganciclovir and its prodrug, valganciclovir, foscarnet and cidofovir [2]. Multiple case studies have shown positive treatment outcomes with ganciclovir with transition to valganciclovir once the infant is tolerating oral feeds [2, 5]. Indications for treatment with these two drugs are commonly cited to reduce the morbidities associated with CMV, such as hearing loss, neurodevelopmental impairment and increased mechanical ventilation [17–19]. Treatment durations in the literature have ranged from 4 to 14 weeks [2, 5]. More studies are needed to guide management for symptomatic postnatally acquired CMV [24].
Our infant passed all hearing screens until follow-up at 12 months of age, which could be related to CMV infection, medications received in the NICU or a consequence of preterm birth. Her moderate to severe developmental delay is likely secondary to preterm birth compounded by severe CMV meningitis. She had no adverse outcomes related to her antiviral therapy.
Although postnatally acquired CMV meningitis has been described in the literature before, to our knowledge this is the first infant to be diagnosed utilizing the BFA. Use of the BFA in CSF analysis allowed definitive therapy for our infant to be implemented much earlier than if only current gold standard analyses had been used. The BFA should be utilized in all CSF analyses, particularly in cases of clinical uncertainty, in order to limit the exposure to empiric antimicrobial therapy and allow earlier definitive therapy to begin. Given the paucity of data regarding which infants with postnatally acquired CMV should be treated and for what duration, multi-center prospective studies are needed to provide evidence and decrease potentially unnecessary antimicrobial exposure.
Statement of ethics
IRB approval was not required for this study. Written informed consent was obtained from the patient’s guardian.
Disclosure statement
The authors declare no conflict of interest.
Funding sources
No funding sources were used to conduct this study.
Author contributions
Drs. Stark and Hornik had full access to all the data in the study and take full responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Stark and Hornik
Acquisition, analysis and interpretation of data: All authors
Drafting of manuscript: Stark
Critical revision of the manuscript for important intellectual content: All authors
Administrative, technical, or material support: Stark and Hornik
Supervision: Peterson, Weimer and Hornik