
Abstract
BACKGROUND:
Congenital pulmonary airway malformation (CPAM) is the most common prenatally-diagnosed lung malformation. This lesion, classified as macrocystic or microcystic, can lead to significant fetal compromise. Management options include observation, maternal antenatal steroid administration, and fetal surgical intervention. Current evidence suggests that microcystic (but not macrocystic) lesions and those with a cyst volume ratio (CVR) >1.6 are responsive to steroid therapy. The objective of this study was to identify patterns of prenatal steroid administration for the management of CPAMs and to identify characteristics of CPAMs prompting steroid administration.
METHODS:
An 18-question survey was distributed to obstetricians from the Pregnancy-Related Care Research Network (PRCRN) and the North American Fetal Therapy Network (NAFTNet), from January to April 2019, to capture antenatal steroid prescribing patterns.
RESULTS:
Response rates were 28.3% (138/487) for PRCRN and 63.3% (19/30) for NAFTNet. Among PRCRN members, 16.8% administered prenatal steroids, with most (77.2%) doing so for both microcystic and macrocystic CPAMs; corresponding percentages for NAFTNet members were 90.9% and 52.6%. Two thirds (65.6%) of obstetricians who administer steroids do so for a CVR > 1.6, without evidence of mediastinal shift or hydrops fetalis.
CONCLUSIONS:
There is a lack of consensus among obstetricians as to the CPAM characteristics that should prompt administration of prenatal steroids. Many surveyed obstetricians do not use cyst type or CVR to guide decision-making regarding steroid therapy.
Introduction
Congenital pulmonary airway malformations (CPAMs) are cystic hamartomas resulting from abnormal branching morphogenesis in the lung. They arise from tracheal, bronchial, bronchiolar or alveolar tissue [1], and represent the most common congenital lung lesion [2, 3]. With the widespread availability of ultrasound imaging, CPAMs are now frequently diagnosed prenatally [2, 4]. During fetal life, the lesion typically grows rapidly from diagnosis at 18–20 weeks gestation until approximately 28 weeks’ gestation, followed by a period of stabilization, and in many cases, spontaneous regression [5, 6]. In severe cases, however, the lesion continues to grow and ultimately may cause severe lung compression, mediastinal shift, hydrops fetalis, and/or fetal demise [7, 8].
Prenatal treatment options for CPAMs range from close observation with serial ultrasounds to open fetal surgery for lesion resection. Historically, the rate of spontaneous regression for congenital lung lesions ranged from 8–49% [9, 10], depending on associated features. However, lesions associated with hydrops fetalis had a universally fatal prognosis [7]. The early 2000’s saw the advent of open fetal surgery with lesion resection for CPAMs causing fetal hydrops, which reduced mortality by 50% [11–14]. Because of the risk of preterm labor associated with open fetal surgery, women undergoing the procedure were given prophylactic steroids to promote fetal lung maturation. Incidentally, it was noted that the fetuses exposed to prenatal steroids and not undergoing lesion resection demonstrated a remarkably high incidence of CPAM regression and resolution of fetal hydrops [11]. The discovery that a noninvasive, relatively benign medical intervention could dramatically reduce fetal morbidity and mortality led to the rapid clinical adoption of prenatal steroid administration, and was further reinforced by subsequent retrospective studies documenting a mortality rate of <20% among hydropic fetuses with microcystic CPAMs receiving antenatal steroids. It is important to note, however, that macrocystic CPAMs did not respond as favorably to antenatal steroid administration, and there was no evidence of a survival benefit for this sub-population [7, 13]. This relatively rapid practice change in the absence of prospective studies evaluating the optimal timing, dosing, and patient population most responsive to steroid therapy has left it to the individual practitioner to determine when, and for whom, steroids should be prescribed. A cyst volume ratio (CVR) >1.6 and presence of mediastinal shift or hydrops fetalis are associated with poorer fetal and neonatal outcomes [8, 16], and are often, though not universally, used as criteria to prompt steroid administration. We hypothesized that steroid prescribing practices would vary significantly among obstetricians, and sought to evaluate this hypothesis by analyzing survey data from a national sample of general and subspecialty-trained obstetricians.
Methods
Survey development and piloting
We developed an 18-question survey to characterize obstetrical practice patterns in the prenatal management of CPAMs [Appendix 1]. The goal of the survey was to determine the extent of practice variability or consensus among a national sample of obstetricians, representing both general practitioners and subspecialists. The survey collected information about (1) obstetrician level of training, (2) CPAM characteristics prompting prenatal steroid administration), (3) earliest gestational age at which steroids would be administered, and (4) how additional prenatal findings, including CVR and presence of mediastinal shift or hydrops fetalis, influence the decision to administer steroids.
The survey was piloted among practicing obstetricians at Johns Hopkins University School of Medicine, in Baltimore, Maryland, for accuracy, clarity, and consistency. The pilot group included general obstetricians (residents, fellows, and attending physicians) and specialists (maternal fetal medicine and fetal therapy). Once the pilot group approved the survey, we sought and received approval from the Institutional Review Board at Johns Hopkins School of Medicine (IRB 00186426).
Survey administration
The survey was administered from January 4, 2019 through April 4, 2019 to members of two national organizations – the Pregnancy-Related Care Research Network (PRCRN) and the North American Fetal Therapy Network (NAFTNet) – which represent general obstetricians and fetal medicine subspecialists respectively. The PRCRN is a research network of academic and non-academic institutions throughout the United States conducting collaborative research examining pregnancy-related care. The group maintains a contact list of approximately 500 practicing obstetricians who have agreed to be surveyed regarding their practice patterns. NAFTNet is a consortium of medical centers in the United States and Canada with expertise in fetal surgery and other fields related to the multidisciplinary care of complex fetal disorders. A large percentage of the membership are obstetricians with additional training in maternal fetal medicine (MFM).
The survey was sent to members of the PRCRN via the network’s administrative staff, based at the University of Washington. Members received a cover letter explaining the research study and an email link to the survey, which was administered via Qualtrics. Three subsequent email reminders were sent to non-responders over a one-month period. The survey was also distributed to the subset of NAFTNet members who were obstetricians, at the organization’s annual conference in Chicago, Illinois, on April 4, 2019. Individuals received a cover letter explaining the research study, and a paper version of the survey.
Statistical analysis
Results were analyzed using descriptive and exploratory statistics with SPSS, version 24 (Armonk, NY).
Results
Survey response
A total of 138 PRCRN members and 19 NAFTNet members returned the survey, yielding response rates of 28.3% (138/487) and 63.3% (19/30), respectively. Within the PRCRN group, there were seven incomplete surveys which were discarded, leaving 131 completed surveys for analysis. Within the NAFTNet group, there were four incomplete surveys; however, respondents wrote in their answers (with their preferred answer choice being easily discernable), or only neglected to answer demographic questions, and thus were included in the analysis.
When comparing demographic characteristics between respondents, we noted three salient differences: (i) all NAFTNet members were MFM specialists, whereas only 15% of PRCRN members were MFM specialists, (ii) NAFTNet members predominately practiced in academic medical settings, while PRCRN members predominately practiced in community settings, and (iii) most NAFTNet members were male (74%), whereas most PRCRN members were female (70%) (Table 1).
Comparison of professional profiles and demographics between general practitioners (PRCRN) and sub-specialists (NAFTNet). Data presented are numbers and percentages
Comparison of professional profiles and demographics between general practitioners (PRCRN) and sub-specialists (NAFTNet). Data presented are numbers and percentages
Among PRCRN members, 17% (22/131) report administering antenatal steroids for the management of CPAM, and all of whom are MFM physicians. For those PRCRN members who do not administer steroids, 15/109 (14%) report continuing to manage patients with CPAMs; the rest either refer these patients (56/109, 51%) or otherwise do not manage their prenatal care (38/109, 35%).
Conversely, nearly all NAFTNet members (17/19) administer steroids for fetal management of CPAMs, and all report subspecialty training in maternal-fetal medicine. With respect to choice of steroids, all 22 PRCRN members report administering betamethasone, while 68% (13/19) of NAFTNet members administer betamethasone (Table 3).
Comparison of administration of maternal steroids for management for CPAMs between general practitioners (PRCRN) and sub-specialists (NAFTNet)
Comparison of administration of maternal steroids for management for CPAMs between general practitioners (PRCRN) and sub-specialists (NAFTNet)
1Data presented are numbers and percentages. 2If the participant answered “no”, the survey ended, as all subsequent survey questions pertained to steroid administration. 3One participant hand wrote they would administer steroids only for hydrops.
Comparison of decision making about prenatal management of CPAMs between general practitioners (PRCRN) and sub-specialists (NAFTNet)
1Data presented are numbers and percentages. 2n = 22 based on built-in skip pattern for electronic survey.
Among PRCRN members who administer steroids, most (68%) report they do not use CVR in their decision-making regarding steroid administration (Table 3). Consistent with this finding, nearly three quarters (16/22) report that they would administer steroids for a CVR < 1 without evidence of mediastinal shift or hydrops fetalis (Fig. 1). This percentage did not change for larger CPAMs (CVR 1–1.6 or >1.6) without evidence of mediastinal shift or hydrops fetalis, (16/22), or in the presence of mediastinal shift alone (15/22).
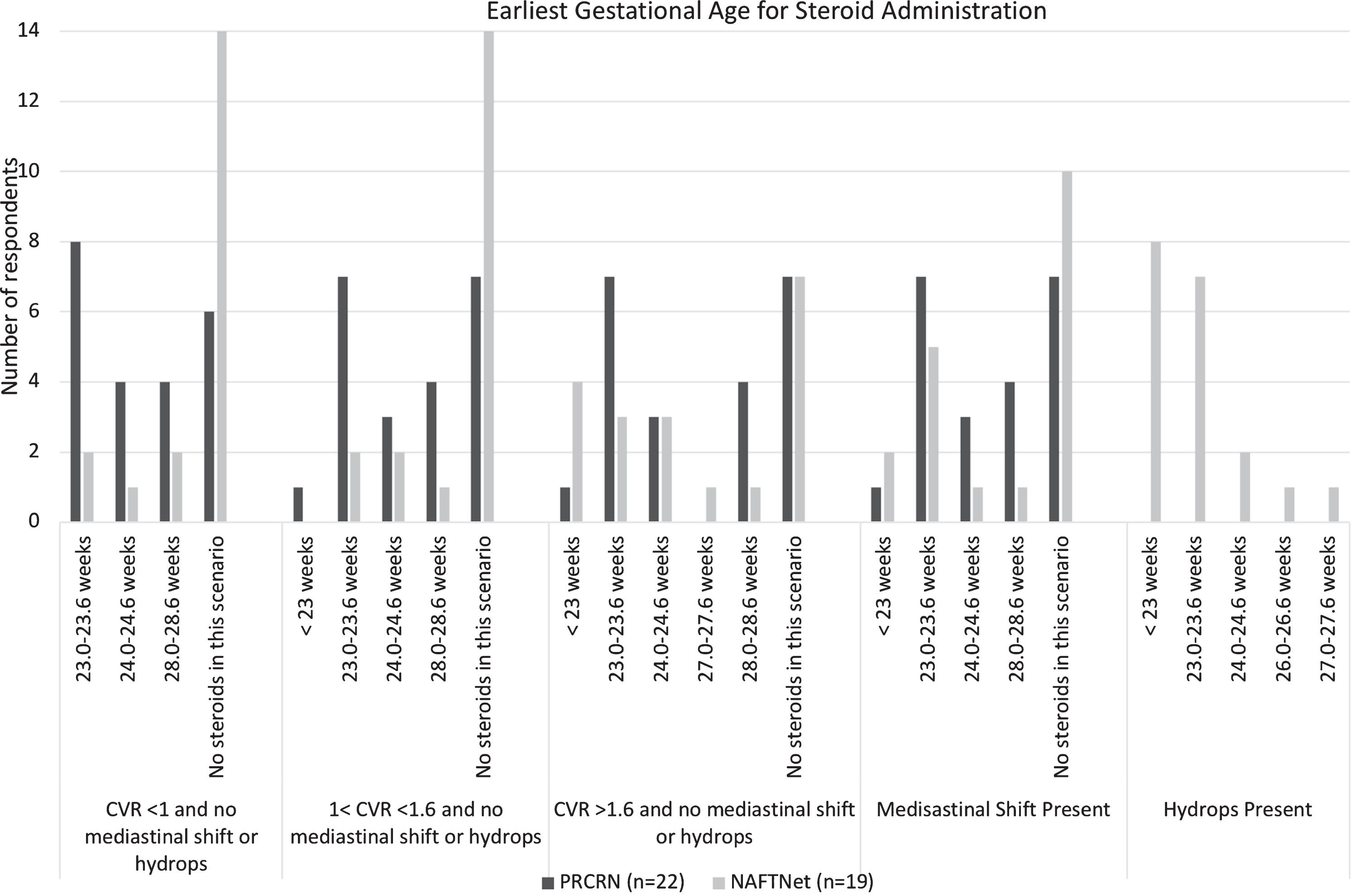
Variations in earliest GA for steroid administration, according to health of the child and between general obstetricians (PRCRN) and national experts (NAFTNet). Note that PRCRN responses are consistent across increasing CVR measurements. NAFTNet members are more likely to administer steroids for a CVR > 1.6. There is no consensus in gestational age for steroid administration.
NAFTNet members were twice as likely as PRCRN members to use CVR measurements when deciding whether to administer steroids (68% versus 32%) (Table 3). Among NAFTNet members, 26% (5/19) would administer steroids for a CVR of <1.6 without evidence of mediastinal shift or hydrops fetalis, and 63% would administer steroids for a CVR of >1.6 without evidence of mediastinal shift or fetal hydrops.
Both PRCRN and NAFTNet members were less likely to use CVR in their decision-making for steroid administration when there was evidence of hydrops or mediastinal shift (Table 3). Of the 22 PRCRN members who report administering steroids, 77% would give steroids for both microcystic and macrocystic CPAMs (Table 2). In comparison, among the 19 NAFTNet members who administer steroids, 11 (53%) would give steroids for a CPAM regardless of cyst type, and six (32%) would administer steroids for microcystic CPAMs alone (Table 2). Three PRCRN members and zero NAFTNet members report administering steroids exclusively for macrocystic lesions.
Steroids were administered at gestational ages ranging from 23.0 to 28.6 weeks among PRCRN and NAFTNet members; there was no gestational age at which antenatal steroids were most frequently administered (Fig. 1). If necessary, both PRCRN and NAFTNet members would administer a second course of steroids for microcystic CPAMs (68% and 63% of respondents, respectively). The NAFTNet members were more likely to use third trimester MRIs to evaluate CPAMs than were the PRCRN members (58% versus 45% respectively).
Discussion
Our survey results demonstrate marked variation in steroid prescribing patterns for the prenatal management of CPAMs among PRCRN and NAFTNet members. We speculate that this variability has been driven by three key factors: (1) the absence of guidelines delineating when and under what circumstances steroids should be administered, (2) lack of familiarity with the literature supporting the efficacy of and indications for antenatal steroid administration in the management of prenatally diagnosed CPAM, and (3) an assumption that regression of the CPAM after steroid administration reflects its expected (untreated) trajectory, and would have occurred regardless of steroid administration.
Our results indicate that most obstetricians who prescribe antenatal steroids agree that the presence of hydrops fetalis should prompt steroid administration. However, cyst type does not appear to influence the decision to administer steroids, as many obstetricians will prescribe them for either type, despite a paucity of evidence demonstrating efficacy in macrocystic lesions. There does not appear to be provider consensus regarding the use of CVR or the presence of mediastinal shift in determining which women have the highest likelihood of deriving therapeutic benefit from antenatal steroids. This finding was surprising given that mediastinal shift traditionally occurs in the presence of an enlarging CPAM, which may subsequently progress to hydrops fetalis or fetal death [15, 18].
We noted marked differences between PRCRN and NAFTNet physicians in their use of CVR measurements in informing prenatal management strategies. Approximately one third of PRCRN physicians and two thirds of NAFTNet physicians used CVR measurements to inform their decision to administer antenatal steroids. Among PRCRN physicians, steroid administration practices remain consistent as CVR increases, whereas for NAFTNet physicians, steroid administration more than doubles when the CVR is >1.6 without evidence of hydrops fetalis or mediastinal shift.
The CVR, a measure of the relative size of the CPAM, is a useful tool in predicting the risk that a lesion will progress to the development of mediastinal shift or hydrops fetalis. A CVR of >1.6 is associated with an increased risk of hydrops fetalis and subsequent fetal demise, and thus, many obstetricians will use this value as an indication for steroid administration. However, once hydrops or mediastinal shift have occurred, it is unclear whether CVR measurements remain relevant to clinical decision-making. We found that obstetricians do consider CVR when deciding whether to administer steroids in the presence of mediastinal shift (17/41) or hydrops fetalis (15/41), which suggests that many, but not all obstetricians will administer steroids independent of CVR when hydrops fetalis or mediastinal shift are present. However, this also highlights differences in the extent to which CVR informs medical decision-making, and how it can increase or mitigate clinician perceptions of risk of poor neonatal outcome in the presence of other independent risk factors [5, 19].
There is no consensus regarding the optimal number of steroid courses to be administered and the earliest gestational age at which steroid administration should begin. Published studies report that for high risk CPAM lesions (CVR > 1.6, presence of mediastinal shift or hydrops fetalis) where an initial course of steroids has failed, a second course of steroids may be effective in improving outcomes (reduction in CVR, resolution of mediastinal shift or hydrops fetalis) [8, 12]. This demonstration of potential benefit, coupled with a relatively benign side effect profile and high morbidity and mortality associated with open fetal surgery, mediastinal shift or hydrops fetalis, may make some providers more amenable to administration of additional steroid courses.
We also found that there was no clear consensus as to the use of third trimester fetal MRI. MRI offers better tissue characterization, spatial resolution, and enhanced morphologic and volumetric measurements of the fetal lungs, as well as more clearly delineating the CPAM margins compared to ultrasound, especially during the third trimester [20]. The lack of consensus most likely stems from the variable availability, higher costs and longer study times associated with fetal MRIs compared to ultrasound, and advances in ultrasound quality and availability that make diagnosis and monitoring of CPAM lesions throughout pregnancy accurate, informative, and relatively easy [2].
Most of the 131 PRCRN members surveyed, 83%, did not administer steroids for the management of fetal CPAMs. The low frequency of steroid administration among the PRCRN members is most likely because these patients are largely referred or managed elsewhere.
Interestingly, this study identified a subset of providers (∼11%) who would not administer steroids for prenatally diagnosed CPAMs yet continue to manage their prenatal care. Although this represents a minority of practitioners, we hypothesize that the willingness to expectantly manage prenatally-diagnosed CPAMs arises from their known natural evolution, and the significant proportion of lesions that spontaneously regress without intervention. As the rate of spontaneous regression ranges from 8–49% [9, 10], some obstetricians may feel that most patients will have an uncomplicated prenatal course with a low risk of fetal compromise, and therefore feel comfortable providing ongoing obstetrical management. The decision to continue expectant management or refer to another provider may be influenced by individual obstetrician experience, parental preferences, and ease of access to subspecialty care.
Overall, the results of this study highlight a national lack of consensus among obstetricians, regardless of training background, as to the circumstances under which steroids should be administered for the prenatal management of CPAM lesions. The study describes the prevalence of obstetrician practices regarding maternal steroid administration, and highlights some differences in management strategies between general obstetricians and those with additional training in maternal fetal medicine. Furthermore, it emphasizes the lack of data to inform clinical practice decisions. Because of this lack of data, the ability of obstetricians to develop evidence-based clinical management algorithms and guidelines for the prenatal management of CPAMs is severely curtailed, and results in marked variability in practice patterns. However, our survey also indicates that the results of clinically-relevant observational studies may not be widely known and have not been uniformly incorporated into routine obstetrical care. This suggests that educational interventions informing obstetricians of the current evidence addressing antenatal steroid use for management of CPAMs, the utility of serial CVR measurements in assessing and managing CPAMs, and the importance of cyst type in predicting response to steroids could have a significant impact on standardizing provider prescribing practices and the prenatal management of CPAMs.
A key strength of this study is the inclusion of members from both PRCRN and NAFTNet, which allows for comparisons between practices prevalent within the general obstetric community versus practices prevalent among specialists specifically trained in the prenatal management of congenital malformations, including CPAMs. Other strengths of the study included physician participants representing a range of years in practice and type of practice (academic vs community).
This study has several limitations. Although the response rate for the PRCRN and NAFTNet members was 28.3% and 63.3% respectively, the sample size of obstetricians reporting administration of antenatal steroids was small – only 41 respondents. Because we were specifically interested in the practices surrounding steroid administration, we did not investigate other modes of prenatal management such as shunts and resection. Additional concerns include partially completed surveys and technical difficulties in obtaining primary data for one question from the PRCRN group.
There are three key conclusions from our study: (i) there is considerable variability in the application of CVR to inform clinical decision-making in the prenatal management of CPAM, which may reflect a knowledge gap or lack of confidence in the clinical utility of the measurement, (ii) among obstetricians who administer antenatal steroids for CPAM, most use the presence of hydrops fetalis as an indication for administration, and (iii) a large proportion of physicians will administer antenatal steroids for macrocystic CPAMs despite a paucity of evidence to support this practice.
Our study highlights the need for collaborative prospective clinical trials to answer important clinical questions that directly inform provider management decisions in caring for fetal CPAMs. Specifically, there is very little information available to assist clinicians in identifying the patient population for whom steroid administration is the most effective, and to identify the optimal timing of steroid administration to achieve the best postnatal outcomes. Future studies should prioritize addressing this knowledge gap, with the goal of generating the evidence necessary to create rigorous, evidence-based consensus guidelines for the prenatal management of congenital lung lesions.
Disclosure statements
Funding
No funding was received for this work.
Ethical approval
This study was approved by the Institutional Review Board at Johns Hopkins School of Medicine (IRB 00186426).
Conflicts of interest
The authors have no conflicts of interest.
Footnotes
Appendix 1
Thank you for participating in this study. We are conducting a survey to help understand current practice patterns with regard to the maternal administration of steroids for fetal congenital pulmonary airway malformations (CPAMs). This study and survey has been approved by the institutional review board (IRB). This survey should take approximately 5 minutes to complete. Participants, their responses, and their individual practices will be kept confidential. Your completion of the survey will serve as your consent to be in this research study.
How many years have you been practicing as an OB/GYN physician? <5 years 5 years to 10 years 11 years to 15 years >15 years
Do you have any subspecialty training in Obstetrics/Gynecology? Yes – Maternal Fetal Medicine Yes – Other No
In what Health Resources and Services Administration (HRSA) region do you practice? HRSA Region 1: Maine, New Hampshire, Vermont, Massachusetts, Rhode Island, and Connecticut HRSA Region 2: New York and New Jersey HRSA Region 3: Pennsylvania, Maryland, Delaware, Virginia, and West Virginia HRSA Region 4: Kentucky, Tennessee, North Carolina, South Carolina, Georgia, Florida, Alabama, and Mississippi HRSA Region 5: Minnesota, Wisconsin, Illinois, Indiana, Michigan, and Ohio HRSA Region 6: New Mexico, Texas, Oklahoma, Arkansas, and Louisiana HRSA Region 7: Nebraska, Kansas, Iowa, and Missouri HRSA Region 8: Montana, North Dakota, South Dakota, Wyoming, Colorado, and Utah HRSA Region 9: Nevada, California, Arizona, and Hawaii HRSA Region 10: Washington, Oregon, Idaho, and Alaska
How would you describe your practice setting? Academic institution Community practice Mixed
Please specify your sex Female Male I do not wish to answer
Please specify your ethnicity or race White or Caucasian Black or African American Hispanic or Latino Asian or Asian American American Indian or Alaska Native Native Hawaiian or other Pacific Islander Another race
Do you ever administer maternal steroids for the management of fetal congenital pulmonary airway malformations (CPAMs)? Yes, for all CPAMs Yes, only for microcystic CPAMs, but not macrocystic Yes, only for macrocystic CPAMs, but not microcystic No, I do not administer steroids for CPAMs and I continue to manage these patients No, I do not administer steroids for CPAMs and I refer these patients to another institution/practice, or provider No, I do not see these patients
Which steroid do you administer for the management of CPAM? Betamethasone Dexamethasone Other
Do you use cyst volume ratio (CVR) measurements when deciding to administer maternal steroids for the management of CPAMs? Yes No
Does the CVR factor into your decision for administering steroids if there is evidence of Yes No
Does the CVR factor into your decision for administering steroids if there is evidence of Yes No
Do you ever administer a Yes No
What is the I would not administer steroids <23 weeks 23.0–23.6 weeks 24.0–24.6 weeks 25.0–25.6 weeks 26.0–26.6 weeks 27.0–27.6 weeks 28.0–28.6weeks 29.0–29.6weeks 30.0–30.6weeks 31.0–31.6weeks >32 weeks
What is the I would not administer steroids <23 weeks 23.0–23.6 weeks 24.0–24.6 weeks 25.0–25.6 weeks 26.0–26.6 weeks 27.0–27.6 weeks 28.0–28.6 weeks 29.0–29.6 weeks 30.0–30.6 weeks 31.0–31.6 weeks >32 weeks
What is the I would not administer steroids <23 weeks 23.0–23.6 weeks 24.0–24.6 weeks 25.0–25.6 weeks 26.0–26.6 weeks 27.0–27.6 weeks 28.0–28.6 weeks 29.0–29.6 weeks 30.0–30.6 weeks 31.0–31.6 weeks >32 weeks
What is the I would not administer steroids <23 weeks 23.0–23.6 weeks 24.0–24.6 weeks 25.0–25.6 weeks 26.0–26.6 weeks 27.0–27.6 weeks 28.0–28.6 weeks 29.0–29.6 weeks 30.0–30.6 weeks 31.0–31.6 weeks >32 weeks
What is the I would not administer steroids <23 weeks 23.0–23.6 weeks 24.0–24.6 weeks 25.0–25.6 weeks 26.0–26.6 weeks 27.0–27.6 weeks 28.0–28.6 weeks 29.0–29.6 weeks 30.0–30.6 weeks 31.0–31.6 weeks >32 weeks
Do you use MRI in the 3rd trimester to evaluate/follow for CPAM? Yes No
Thank you for completing this survey. Your responses will help us understand practices for CPAMs. Our goal is to share this information with the scientific and medical community through publication.
Acknowledgments
We would like to thank all the survey participants. The Pregnancy-Related Care Research Network is supported by the Health Research and Services Administration Grant UA6MC31609.