
Abstract
BACKGROUND:
The intrauterine environment is a key determinant for long-term health outcomes. Adverse fetal environments, such as maternal diabetes, obesity and placental insufficiency are strongly associated with long-term health risks in children. Little is known about differences in fetal cardiac output hemodynamics of diabetic mothers (DM) vs. non-diabetic mothers (NDM). Our study aims to investigate the left-sided, right-sided, and combined cardiac output (CCO) in fetuses of DM vs. NDM.
METHODS:
Retrospective data were collected in fetuses of DM (N = 532) and NDM (103) at mean gestational age 24 weeks. Examination included 2D echo and pulse wave Doppler. Wilcoxon rank sum tests and Chi-square tests were used to test for distribution difference of maternal and fetal continuous and categorical measures respectively between DM and NDM. Intraclass correlation coefficients were calculated to assess intra-observer reliability of fetal cardiac measurements.
RESULTS:
DM mothers had higher mean weight (89.7±22.2 kg) than NDM (76.8±19.8 kg), p < 0.0001 and higher mean BMI (33.4±7.5) than NDM (28.3±5.8), p < 0.0001. C-section delivery occurred in 66% of DM vs. 35% of NDM fetuses. Fetuses of DM mothers had significantly larger semilunar valve diameter, higher left ventricular (LV) output, higher combined cardiac output and lower right ventricle /left ventricle ratio compared to NDM.
CONCLUSION:
The greater CCO (adjusted for fetal weight), left sided cardiac output in the fetuses of DM, compared to NDM, represent differences in cardiac adaptation to the diabetic environment.
Keywords
Introduction
The intrauterine environment is a key determinant for long-term health outcomes in children [1, 2]. Poor maternal lifestyle, diabetes, metabolic disease, and placental insufficiency are associated with negative effects on the long-term development of the child’s health [1–4]. It is estimated that 422 million adults are affected with diabetes worldwide [5]. Among this, 129.4 million women aged 20–49 years are diagnosed with diabetes and the global prevalence of live births affected by maternal diabetes is approximately 20.9 million [6].One of the health risks observed in fetuses of DM is myocardial hypertrophy [1, 4]. Hornberger reported myocardial hypertrophy in fetuses of DM as early as 20 weeks of gestation, even in the presence of reasonably controlled blood glucose levels [7]. There is no sufficient data to support the assumption that changes to the fetus resolve postnatally within months. The potential effects of the prenatal cardiac output (CO) during the second trimester have not been previously studied in a large sample size. Recent data in 30 diabetic mothers, fetal CO data from Kutty et al. shows decreased stroke volume and CO for RV and LV [8]. However Lisowski et al. found the combined ventricular output, both absolute and per kg estimated fetal weight in fetuses of DM were significantly higher and increased with advancing gestational age compared to NDM [3].
Although there has been evidence of health risks for fetuses with poor metabolic state, little is known about the differences in fetal CO between DM and NDM, due to limitations of studies concerning functional and structural cardiac changes that occur in fetuses of DM. The objective of this study was to investigate the left-sided, right-sided, and CCO in fetuses of DM versus NDM.
Methods
A retrospective review of the University of Minnesota Division of Pediatric Cardiology fetal database was performed and granted exempt status by the Institutional Review Board. A total of 9200 fetal echocardiograms were performed during the study period, of which 635 fetal data were chosen with the inclusion and exclusion criteria. Of the 635 fetal data, 532 were of DM (study group) and 103 of NDM (control group). Of the 532 DM, 175 had gestational diabetes, 165 had Type-1 diabetes, 188 had Type-2 diabetes, and 4 had unknown type as seen in (Table 1). Inclusion criteria were mothers diagnosed with history of diabetes and a normal fetal echocardiogram. Exclusion criteria were fetuses diagnosed with cardiac defects, chromosomal anomalies and extracardiac defects. NDM indications for echocardiogram were with a variety of diagnoses including family history of heart defects, 2 vessel umbilical cord and increased nuchal translucency. Maternal data includes age, height, weight, delivery type, body mass index (BMI), race and ethnicity. Study group and control group were controlled for age. Measurements of glycosylated hemoglobin level (HbA1c %) were documented during the second or third trimester of DM. The normal HbA1C range in our laboratory was 4.3 –6%. The studies were de-identified, reviewed by a single investigator and blinded to the DM vs NDM status at the time of data interpretation.
Summary statistics for diabetic mothers (DM), non-diabetic mothers (NDM)
Summary statistics for diabetic mothers (DM), non-diabetic mothers (NDM)
Great artery valve diameters were measured in systole on real time echocardiography. Doppler sample volumes were located in the great arteries immediately distal to the semilunar valves with a Doppler beam parallel to the long axis of the aorta or pulmonary artery Fig. 1. These measurements are average of 3 consecutive beats which includes aortic valve (AV) annulus and pulmonary valve (PV) annulus diameters, aortic and pulmonary velocity time integral and heart rate (HR). AV and PV annulus diameters and velocity time intervals measurements were repeated by the same observer on a randomly selected subset of 10% of the analysis sample for evaluation of intra-observer reliability.

Fetal echocardiography image: Aortic velocity time integral and aortic valve annulus diameter.
Right and left sided CO calculated from fetal echocardiogram data and CCO were normalized by estimated fetal weight [9–11]. The fetal weight was calculated using the Hadlock formula [11]. CO was calculated using the following formula = [0.785* (d∧2) * time integral velocity * heart rate] / weight.
Descriptive statistics including the mean, standard deviation and median for continuous measures and percent for categorical measures were calculated for all fetuses and separately for fetuses of DM and NDM. The Wilcoxon rank-sum test is a nonparametric alternative to the two-sample t-test which is based on the ranks of the observations rather than actual values so test results are not unduly influenced by outlier values, which may be present in variables with skewed distributions. Box plots were generated for several fetuses and maternal measures to provide visual descriptions of the distributional differences Fig. 2. The intraclass correlation coefficient (ICC) was calculated for repeated measurements to assess intra-observer reliability. Alpha significance level of 0.05 was used to assess statistical significance. All analyses were carried out using SAS v9.4 software.
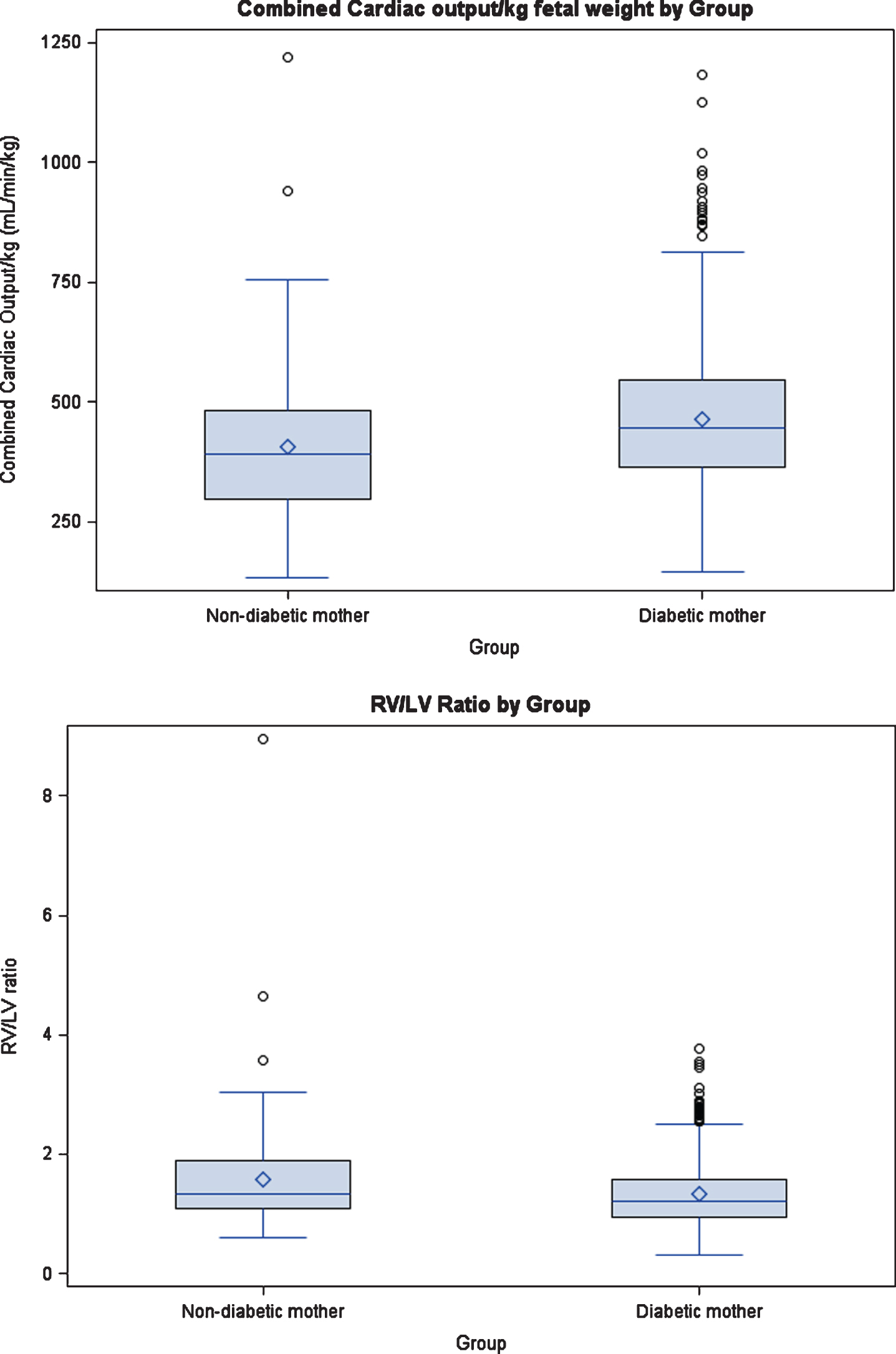
Box plots shows significant differences in fetal measures of the combined cardiac output and RV/LV ratio between non-diabetic mother and diabetic mother.
Maternal data
DM had higher weight, and BMI than NDM. Of the 428 DM with BMI data, a significantly higher percent were obese (BMI≥30) than NDM (64.3% vs. 30.9%, p < 0.0001). The percent of DM who met the BMI criteria for obesity varied by type of diabetes with the highest obesity rate for Type-2 DM (78.5%), followed by gestational (69.1%), and lowest for Type-1 DM (42.2%). Significantly more DM had a C-section delivery than NDM (66% vs. 35%, p < 0.0001). There were no significant differences between DM and NDM in parity (primiparous (33% vs. 42%, respectively, p = 0.09), or race (white 75% vs. 79% p = 0.5).
Fetal measures
All fetuses had normal cardiac anatomy. The fetuses of DM and NDM had similar mean gestational age, fetal heart rate and weight at the time of fetal echocardiography. PV and AV diameter were greater in DM than NDM fetuses. ICCs for repeated measures of AV and PV diameters were 0.87; ICCs for aortic and pulmonary velocity time intervals were 0.91 and 0.94, respectively [12]. The (CCO) ml/min/kg was higher in DM versus NDM fetuses. RV/LV ratio was lower in DM vs. NDM, p = 0.002. (Table 2), Fig. 2.
Summary statistics for diabetic mothers (DM), non-diabetic mothers (NDM) fetuses
Summary statistics for diabetic mothers (DM), non-diabetic mothers (NDM) fetuses
Our descriptive data show that in fetuses of DM mean left ventricular output was significantly higher than in NDM. In addition the mean combined ventricular output, both absolute and per kg estimated fetal weight, were greater in the fetuses of DM. The difference observed in aortic and pulmonary valve diameters may also represent cardiac adaptation to the diabetic environment.
Placenta reflects the metabolic milieu of both mothers and fetus. It is a valuable tool for studying the metabolic perturbations that may take place during pregnancy, such as diabetes mellitus. The extent to which maternal glycemic control contributes to placental abnormalities remains unclear [13]. Several studies have identified histopathologic placental abnormalities among women even with well-controlled pregestational and gestational diabetes. Huynh et al did a comprehensive systematic review of the relevant literature on placental pathology in maternal diabetes and they found that, the common placental findings in pregestational diabetes and in GDM are increased villous immaturity and angiogenesis. Placenta from pregnancies complicated by dysglycemia may display increase in branching and non-branching angiogenesis [13]. In GDM, increased placental weight, fibrinoid necrosis, chorangiosis, ischemia and villous immaturity were reported. Placental changes may vary based on the gestational period during which the diabetic insult occurred. Several studies have shown that the correction of hyperglycemia might not prevent the development of placental abnormalities, because the placental histopathologic changes persisted even in pregnancies with well-controlled diabetes. These changes in placenta in maternal diabetes might affect the developing cardiovascular adaptation in the fetus. Since the placenta is positioned between maternal and fetal circulation, it is exposed to diabetes-associated endocrine and metabolic derangements of both the mother and fetus [14].
Fetal hypoxemia may occur because of a relative immaturity of the placenta. These changes in fetal circulation might be a compensatory reaction to the existence of a possible chronic hypoxemic situation [7, 15]. Correct placental development and function are essential for fetal growth and long-term well-being of the offspring [16]. A peak period of sensitivity to lack of glycemic control has been identified as 8–16 weeks of human gestation [17]. Studies in mice models of DM vs.NDM revealed times of onset and progression of functional differences in adaptations of maternal and fetal CV systems that appear to be attributable to hyperglycemia. Even with the advent of screening and aggressive management of diabetes, the incidence of neonatal complications ranges from 12–75%. Similarly despite optimal blood glucose control increased incidence of macrosomia and intrauterine growth retardation (IUGR) were reported in fetuses of DM [2, 18].
Our results were similar to those of Lisowski et al., longitudinal study who found that the blood flow across the tricuspid and mitral valve orifices of 17 fetuses of type-I diabetic women were significantly higher and increased more with advancing gestational age than those in normal pregnancies. This study showed that even in well-controlled diabetic pregnancies the combined ventricular output, both absolute and per kg estimated fetal weight, was greater in the fetuses of diabetic women. These data indicate significant differences in the fetal circulation between normal pregnancy and well-controlled type-I diabetic pregnancies and suggest the existence of a compensatory mechanism which increases cardiac output and causes cardiac hypertrophy [3]. A study from Henriques-Coelho T et al. on fetal cardiac function utilizing speckle tracking demonstrated that fetuses of mothers with diabetes present in the third trimester signs of biventricular diastolic dysfunction, demonstrated by lower diastolic strain rate values, and of right ventricular systolic dysfunction, evident by the lower global longitudinal strain for this ventricle [19].
In our study the right-sided cardiac output was lower for DM with corresponding higher left ventricular cardiac output and thus lower RV/LV ratio (DM mean ratio was 1.3 vs 1.6 for NDM). Our observation of increased stroke volume ejected through greater aortic and pulmonary valve orifices, with similar VTI in fetuses of DM needs further evaluation. The greater combined cardiac output (adjusted for fetal weight) and left sided cardiac output in the fetuses of DM, compared to NDM, may represent differences in cardiac adaptation to the diabetic environment, possibly myocardial stiffness of the right ventricle or increased metabolic demand to the left sided cardiac structures, brain, and myocardium.
Conclusion
This large retrospective study demonstrates the greater CCO (adjusted for fetal weight), left sided cardiac output in the fetuses of DM, compared to NDM, represent differences in cardiac adaptation to the diabetic environment. In addition to diabetes maternal risk factors, such as obesity or overweight might have further modified fetal cardiac output. Further prenatal follow-up starting from the first trimester and continuing to monitor during the second and third trimester could provide insight in the mechanisms of these differences. Maternal blood glucose levels, weight gain during pregnancy, monitoring of BP may also provide additional value in understanding the changes and the mechanism of these differences.
Limitation
A limitation of this study includes the retrospective design, which does not allow exploring casualty. Blood pressure status of the mothers was not available at the time of data collection and absolute fetal weight estimation could be a limitation. We did not study the reproducibility of the ultrasound parameters regarding fetal weight estimation. However, McLaren et al found that the accuracy of predicting birth weight among diabetic women is similar to that among women without diabetes, regardless of the sonographic model used [20]. In addition valve flow velocity pattern and ventricular thickness, this may be affected by numerous variables, such as maternal BMI, ventricular compliance, loading conditions and myocardial contractility. Prospective studies should be conducted to monitor these parameters in the 3rd trimester.
Conflict of interest
The authors have no potential conflicts of interests, real or perceived, to report with regard to this work
Funding
No funding.