
Abstract
BACKGROUND:
Aortic thrombosis in neonates is a rare phenomenon, and in most cases iatrogenic. An early recognition of the clinical features and an immediate intervention can offer a better prognosis, and thus preventing morbidity such as limb amputation, and even mortality.
METHODS:
We present two cases of full-term newborns with a thrombosis of the abdominal aorta hospitalized in the neonatal intensive care unit of Mohammed VI University Hospital in Marrakech in 2017 and 2019.
RESULTS:
The two patients presented swelling and cyanotic lower limbs. Doppler ultrasound revealed a pathological lower limb blood flow as a result of a thrombosis of the abdominal aorta. Both patients underwent an anticoagulant therapy, the first one benefited from a surgical thrombectomy, he developed a reperfusion syndrome with alveolar hemorrhage, and passed away as a result of a cardiorespiratory arrest. However the second patient got amputated of the right foot, his clinical evolution was favorable with a good healing of the surgical wound without recurrence of any thrombosis.
CONCLUSION:
Through those cases clinicians should be aware of the first clinical signs of this condition in order to offer a rapid and successful management.
Introduction
Neonatal thrombosis is uncommon and relatively rare. It is mostly related to iatrogenic events, spontaneous thrombosis is less frequent and can be related to aortic and renal vein thrombosis. This condition still present considerable challenges in diagnosis and management. A rapid and effective clinical assessment and an appropriate therapy are essential as the neonatal thrombosis varies from asymptomatic incidents to life or limb threatening events. Strategies for management are still evolving, and evidence based treatment algorithms are lacking [1–3].
CASE 1
We present a case of a 41 weeks no consanguineous baby boy, weighing at birth 3 kilograms, born to a 28 year old mother via vaginal delivery, with no particular medical history such as a miscarriage event or maternal diabetes.
The patient presented jaundice within 2 days of birth with a urinary infection, complicated with seizures. At day 3, the newborn had swelling and ecchymosis on lower limbs, which began in the feet and extended to the thighs over the next days. By the day 10, the patient was admitted to the hospital in the neonatal intensive care unit, presenting a cyanosis on the left lower limb and on the right foot (Figs. 1–3), with an onset of gangrene on two right toes (Fig. 2). The baby had a functional impairment and a lack of spontaneous movement, with no reactivity to pain. Right and left femoral pulse was diminished at first, becoming not palpable within the next hours, with a peripheral coldness and a prolonged capillary refill. Oxygen saturation was over 92 %in the four limbs, the systolic blood pressure of the upper limbs was around 80 mmHg, the diastolic one around 45 mmHg. The patient did not present any sign of dehydration; his admission’s weight was 3300 grams.

Pre-operative appearance of the two lower limbs.

Pre-operative appearance of the right foot.

Pre-operative appearance of the left lower limb.
Preoperative biological assessment found polycythemia with hemoglobin (Hb) at 21.2 g/dL, hema-tocrit (Hct) at 69.2%and a thrombopenia at 38000/mm3, the sedimentation velocity was 2 at the 1st hour and 5 at the 2nd hour, C-reactive protein (CRP) came at 10 mg/l, prothrombin time (PT) count 60.8%with an INR of 1.32, at last the fibrinogen came at 2.43 g/l. Initial lower limbs doppler ultrasound revealed a peripheral arterial disease with an absence of the right lower limb blood flow, with demodulated left proximal arterial blood flow.
Echocardiography did not reveal any cardiac abnormalities. Abdominal CT angiogram showed a thrombotic occlusion of the abdominal subrenal aorta (Fig. 4).
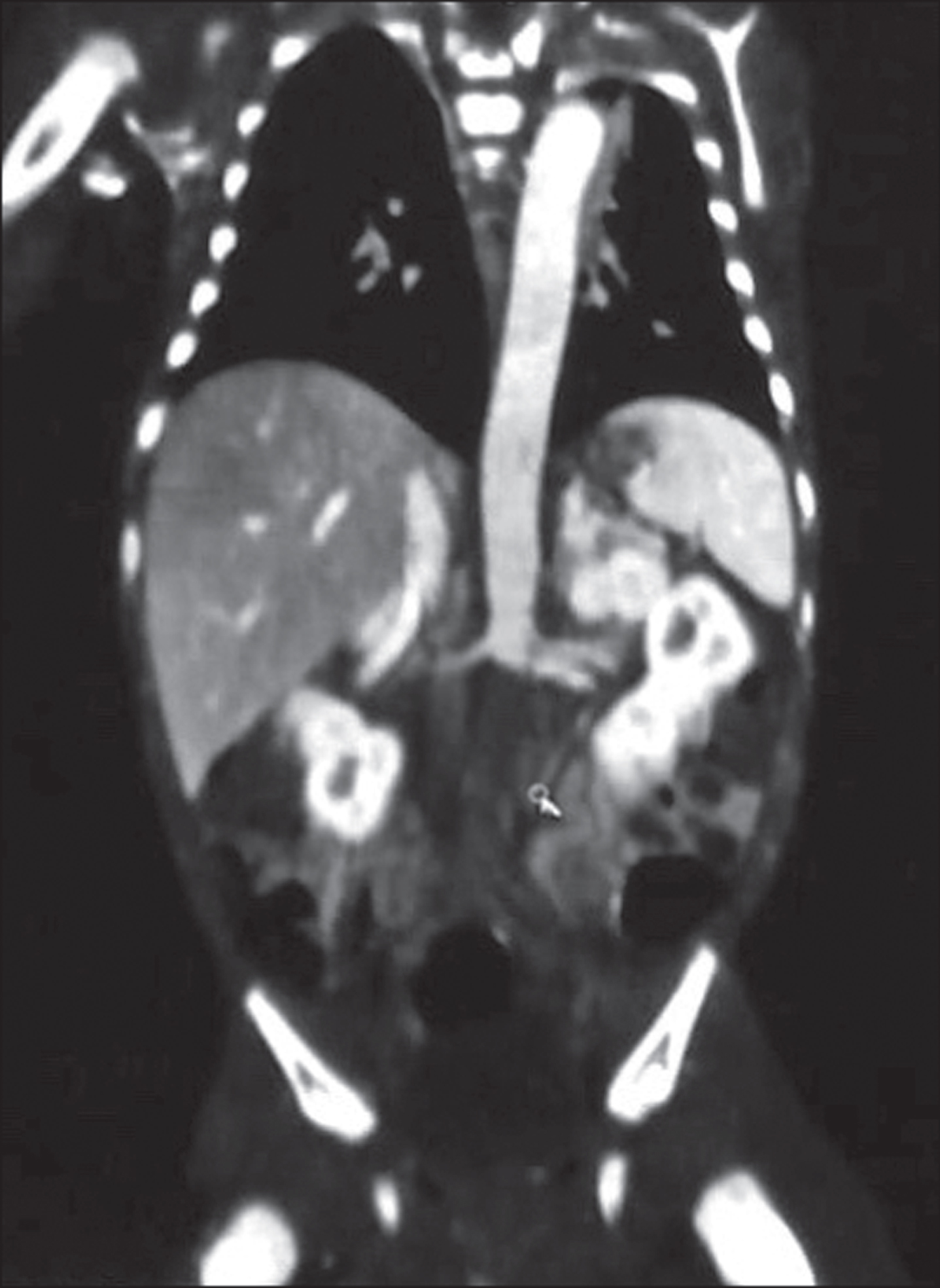
Thrombotic occlusion of the abdominal subrenal aorta.
The patient was put on unfractionated heparin (UFH) treatment starting at 100 U/kg, and because of thrombocytopenia one unit of platelets was transfused preoperatively. Bleeding of 40 ml was induced to minimize the risk of an additional thrombus because of the high hemoglobin level.
He urgently underwent a surgical thrombectomy, the abdominal aorta and both iliac arteries were explored (Fig. 5) and a thrombus was removed from those 3 axes with the use of a Fogarty catheter 3Fr. The patient benefited from a per operative administration of 300U of UFH. By the end of the surgical procedure the left femoral pulse was palpable, however the right femoral pulse wasn’t perceived.
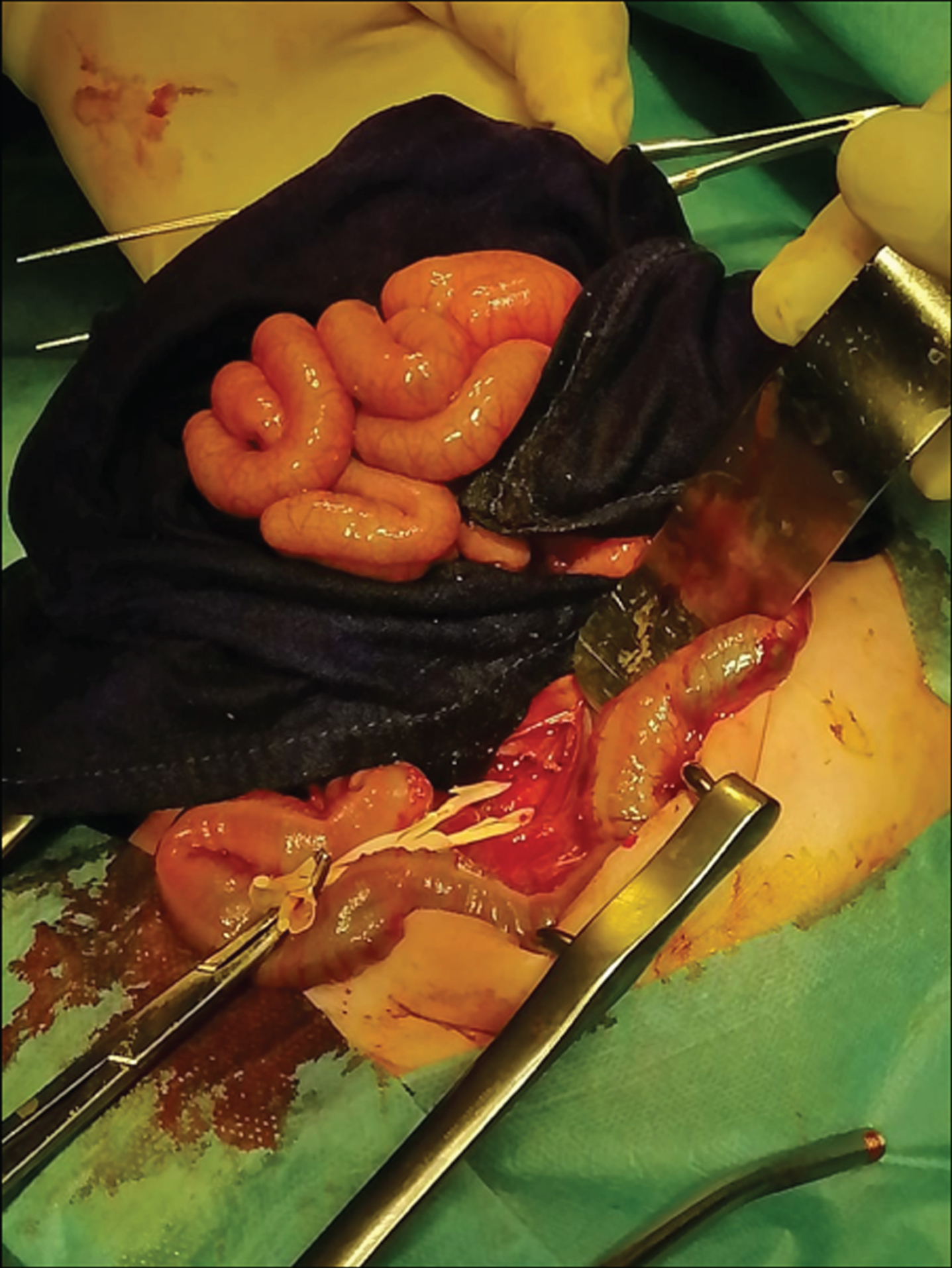
Perioperative individualization of the abdominal aorta.
Over the next hours, the patient developed edema of both limbs, with a reduction of the cyanotic appearance of the left lower limb (Figs. 6, 9), and a reperfusion of the right lower limb (Fig. 6), the two right toes remained dusky without progression to frank necrosis (Fig. 8).

Post-operative appearance of the two lower limbs.

Post-operative appearance of the left lower limb.

Post-operative appearance of the left foot.

Post-operative appearance of the right foot.
Post-operative investigations were as follows: Hb at 9.7 g/dL, Hct at 29.7%, platelet at 108000/mm3, the PT came at 12%, the activated partial thromboplastin time was prolonged to 100 seconds. The newborn presented hyperkalemia at 9.92 mEq/l, and acidosis with an alkaline reserve at 7 mEq/l. At the neonatal intensive unit care the patient developed a bradycardia with a heart rate of 70 beats/min, for which he was put on 5 ug/kg/min of dobutamine, and 175 UI/kg/day of heparin. The patient presented a reperfusion syndrome with alveolar hemorrhage, and later passed away as a result of a cardiorespiratory arrest.
In order to identify the etiology of this condition, we have measured the C and S protein level, and the antithrombin III, however we couldn’t benefit from the results because of the early use of heparin. Other investigations couldn’t be done because of the low economical level of the parents.
The second patient is a male no consanguineous newborn, weighing at birth 3000 grams, born to a mother aged 36 years without any particular medical history, admitted to the neonatal intensive care unit on his 13th day of life for acute lower limb ischemia. At birth, the newborn presented respiratory distress with generalized cyanosis which spontaneously decreased over the first 24 hours. On his admission, the patient had a weight of 3600 grams; he was hemodynamically and respiratory stable, with a normal value of the blood pressure and the oxygen saturation on the four limbs. Examination of the lower limbs had found coldness of the extremities with a purplish blue coloration of the feet (Fig. 10, 11), mainly on the right foot with necrosis of the right toes (Fig. 10). Examination of the peripheral pulses found an abolished right pedal pulse and a weak femoral pulse on both sides. Protein C, S and antithrombin III assays were normal. Maternal anti-nuclear and anti-cardiolipin antibodies were negative.

Appearance of the right foot.

Appearance of the left lower limb.
The biological assessment made on admission found: hemoglobin at 24 g/dL, white blood cells at 12290/mm3, thrombocytopenia at 31000/mm3, CRP at 14.8 mg/L, and PT at 64%.
An emergency doppler ultrasound of the lower limbs showed an absence of arterial flow in the fem-oral and iliac line of the two lower limbs, which is more pronounced on the right side, as a result of a thrombotic obstruction at the aortoiliac level. Ech-ocardiography found a hypertrophic cardiomyopathy localized in the interventricular septum without a subaortic obstruction, with a patent foramen oval.
The patient was placed on intravenous bi-antibiotic therapy with 3rd generation cephalosporin with 100 mg/kg/day and gentamycin with 3 mg/kg/day. Heparin therapy was initiated with LMWH at a dose of 1.5 mg/kg/12 h combined with corticosteroid therapy 5 mg/kg/6 h. The evolution was marked by a limitation of the necrosis of the right foot and by the suppression of the cyanosis of the left foot (Figs. 12, 13). The doppler ultrasound performed after 15 days of treatment with LMWH showed thrombosis of the abdominal subrenal aorta and proximal primary iliac arteries with an absence of flow in the external iliac arteries. The newborn had to be amputated of the right foot taking the lower third of the right leg. In early post-operative period, a combination of LMWH at a dose of 3 mg/kg/day and aspirin at a dose of 5 mg/kg/day was started. A doppler ultrasound done in 30 days of treatment with LMWH showed a weak flow in the arteries of the lower limbs with a slow and abnormal pulsed doppler trace.

Appearance of the right foot after 15 days of treatment.

Appearance of the left foot after 15 days of treatment.
After one month of hospitalization, the clinical ev-olution was favorable with a good healing of the surgical wound without recurrence of any thrombosis.
Neonatal thromboembolism (TE) is extremely variable and largely dependent on the location and the size of the thrombus. It is mostly iatrogenic related to vascular catheterization of central or peripheral arteries and umbilical lines, it has been rarely described at birth spontaneously, being either aortic as shown in our cases or renal vein thrombosis [2, 3]. Risk factors include maternal diabetes, maternal lupus, delayed rupture of membranes, polycythemia, dehydration, asphyxia, patent ductus arteriosus and coagulopathy [4–7]. Our patients presented polycythemia with no other evident etiology. TE has been categorized as arterial, venous, and central nervous system events. Its presentation may vary from asymptomatic or discrete symptoms to life threatening complications. Arterial vascular events, accounting for about half of all TE in the neonatal population [2], the clinical features of peripheral arterial occlusion are gathered as the 6P: pallor, pulselessness, paralysis, pain, paraesthesia, and perishing cold of involved extremity [2, 8]. At least four of the above were presented in our cases. The clinical presentation varies depending on the site and time of occlusion.
Doppler ultrasound is the most common imaging technique used in the diagnosis of neonatal arterial or venous thrombosis, it can demonstrate absence of flow in complete occlusion and diminished flow in partial one. Abnormal arterial waveforms are also dia-gnostic of partial or complete arterial occlusion even if the thrombus is not visualized [9, 10], using either echocardiography or abdominal ultrasound is also applied to confirm clinical suspicion of TE or to screen patients for clinically silent form [2]. Our pat-ients undergo a transthoracic and limb doopler ultrasound imaging, showing a thrombotic occlusion of the abdominal aorta resulting in a limited lower limb blood flow.
The lack of randomized clinical trials about the management of neonatal TE emergencies limited neonatologists’ medical decisions [11], treatment guidelines for pediatric patients with TE events most often are extrapolated from the literature regarding adults. The goal of treatment is to prevent life-threatening consequences, thrombus extension and recurrence, and long term complications, without significantly increasing the risk of bleeding [12], as seen on the presented cases, one of them got bleeding complication and passed away, while the second one had a limb loss with a long-term functional impairment.
The American College of Chest Physicians Evidence Based Clinical Practice Guidelines presented a guideline strategy for the management of thrombosis in neonates and children, for neonates with acute femoral artery thrombosis; the guideline recommend therapeutic doses of intravascular unfractionated heparin (UFH) as initial therapy. For neonates with a limb or organ threatening with no response to initial UFH therapy thrombolysis is recommended, and when initiating UFH therapy, UFH boluses should be no greater than 75 to 100 units/kg and that boluses be withheld or reduced if there are significant bleeding risks, in addition long-term use of therapeutic UFH in children should be avoided [13]. A review summarized the management of aortic thrombosis; therapeutic options include UFH or low molecular weight heparin (LMWH), thrombolytic therapy, and surgical thrombectomy, but there are insufficient data to recommend any one treatment over others, especially regarding spontaneous aortic thrombosis [14]. The first patient had been put on a dose of 100 U/kg of UFH, he also received a bolus of 300 U during the surgical procedure, as it is recommended in the previous review [14], and on the other hand, the second case had been put on LMWH at a dose of 3 mg/kg/day over a period of one month without any significant bleeding complications. Following these two cases, we have noticed that in this situation the use of LMWH is more beneficent for newborns in terms of preventing hemorrhage.
Conclusion
Spontaneous neonatal TE is a rare condition of uncertain cause that requires early diagnosis and management. Neonatologists and pediatricians should be aware of the first clinical signs in order to avoid limb and organ damage. Strategies for management are still evolving, we hope that more guidelines will be provided in order to improve the care given.
Footnotes
Aknowledgment
We would like to thank the patients’ family for their cooperation during the hospitalization period.
Disclosure statements
None.
Conflicts of interest
The authors declare no conflict of interest.