
Abstract
BACKGROUND:
Recently, the first report of lung ultrasound (LUS) guided recruitment during open lung ventilation in neonates has been published. LUS guided recruitment can change the approach to open lung ventilation, which is currently performed without any measure of lung function/lung expansion in the neonatal population.
METHODS:
We included all the newborn infants that underwent a LUS-guided recruitment maneuver during mechanical ventilation as a rescue attempt for an extremely severe respiratory condition with oxygen saturation/fraction of inspired oxygen (SpO2/FIO2) ratio below 130 or the inability to wean off mechanical ventilation.
RESULTS:
We report a case series describing 4 LUS guided recruitment maneuvers, underlying crucial aspects of this technique that can improve the effectiveness of the procedure. In particular, we describe a novel pattern (the S-pattern) that allows us to distinguish the recruitable from the unrecruitable lung and guide the pressure titration phase. Additionally, we describe the optimal LUS-guided patient positioning.
CONCLUSIONS:
We believe that the inclusion of specifications regarding patient positioning and the S-pattern in the LUS-guided protocol may be beneficial for the success of the procedure.
Keywords
Introduction
Lung ultrasound (LUS) is being increasingly used as diagnostic tool in the neonatal intensive care units (NICUs) [1]. However, the possibility to monitor and guide mechanical ventilation with LUS in neonates has not been fully explored yet. Recently, the first trial documenting the efficacy of LUS in guiding lung recruitment maneuvers during mechanical ventilation has been published [2]. This recent publication by Shady and colleagues is particularly relevant, as LUS guided recruitment may refine mechanical ventilation strategies in neonates. Currently, in the neonatal population, the lack of practical tools to monitor lung expansion/lung function, such as static volume curves or CT scan imaging [3], has led to recruitment maneuvers being based on oxygenation as a surrogate for lung volume changes [4, 5]. However, oxygenation does not always correlate with lung recruitment and oxygenation-based lung recruitment may be not only ineffective, but also harmful in some cases [6, 7].
We report a case series that utilizes some specific novel features of the LUS-guided lung recruitment, which could be used to improve the effectiveness of this innovative technique.
Methods
We included all the newborn infants that underwent a LUS-guided recruitment maneuver during mechanical ventilation as a rescue attempt for an extremely severe respiratory condition with oxygen saturation/fraction of inspired oxygen (SpO2/FIO2) ratio below 130 [8], or the inability to wean off mechanical ventilation. Infants were included regardless of their underlying condition, as long as they showed evidence of lung consolidation (C-pattern, Fig. 1) at LUS evaluation. The LUS guided recruitment procedures were performed between January 2020 and July 2020. Data was retrieved retrospectively.
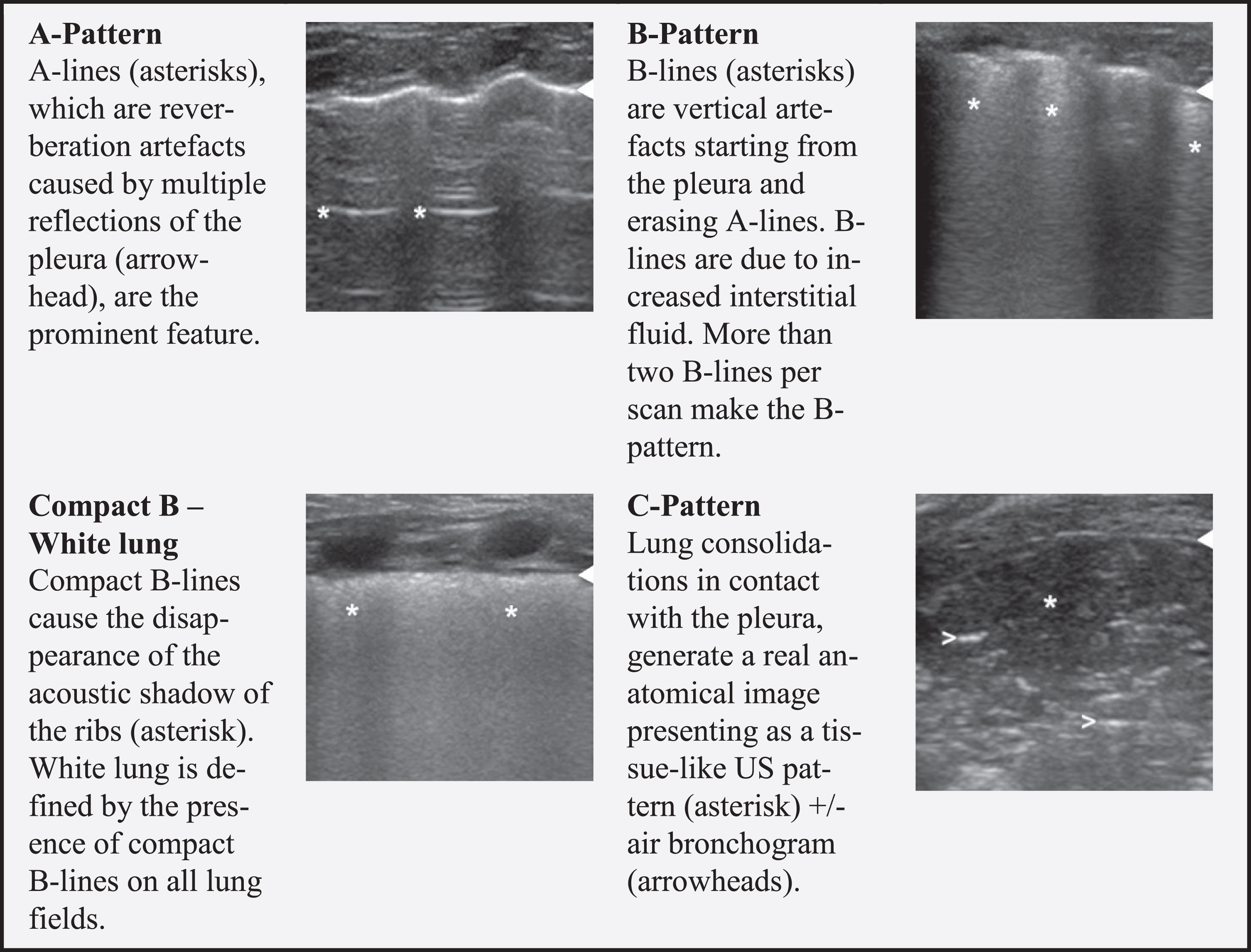
Lung ultrasound patterns.
LUS manoeuvre is described in Fig. 2. Briefly, LUS was systematically performed on all lung fields (anterior superior, lateral superior, posterior superior, anterior inferior, lateral inferior, and posterior inferior for the right and left sides) [1]. LUS examination, executed by an expert neonatologist, was performed by using a high-frequency linear probe (9–16 MHz [1]) with General Electric Medical System LOGIQ S8 or with Mindray DC8-EXP ultrasound machines. When lung consolidation was detected (C-pattern, Fig. 1), and after exclusion of the corrigible causes of lung collapse (e.g., endotracheal tube misplacement), the LUS guided recruitment was carried out. The selected probe was placed in the most dependent zone of the atelectatic lung and then a stepwise pressure increase began, either positive end expiratory pressure (PEEP) or continuous distending pressure (CDP). PEEP/CDP was increased by 1 cmH2O every two minutes. The aim of this was to visualize the progressive lung re-aeration. The pressure was increased until the opening PEEP/CDP was reached. As opposed to the oxygenation-based recruitment maneuver, where the opening PEEP/CDP is the pressure at which oxygenation no longer improves, we based the definition of opening PEEP/CDP on the sonographic evidence of atelectasis resolution. Sonographically, this was represented by the disappearance of the consolidation pattern (C-pattern, Fig. 1) and the appearance of a B-pattern or a white lung image (Fig. 1). Following this, LUS was systematically performed another time; and, if no consolidation was detected in any of the lung fields, this level of airway pressure was defined as opening PEEP/CDP. Once the opening PEEP/CDP was reached, LUS allowed us to find the closing PEEP/CDP as the pressure was decreased in a stepwise manner. PEEP/CDP was decreased by 1 cmH2O every two minutes. The closing PEEP/CDP was defined as the very moment where the LUS began to show the reappearance of lung consolidation. During this phase, the probe was kept in the same dependent lung region as before. Then, the optimal PEEP/CDP was set right above the closing pressure. A throughout LUS follow-up was performed 1 hour, 6 hours and 12 hours after the end of the maneuver.
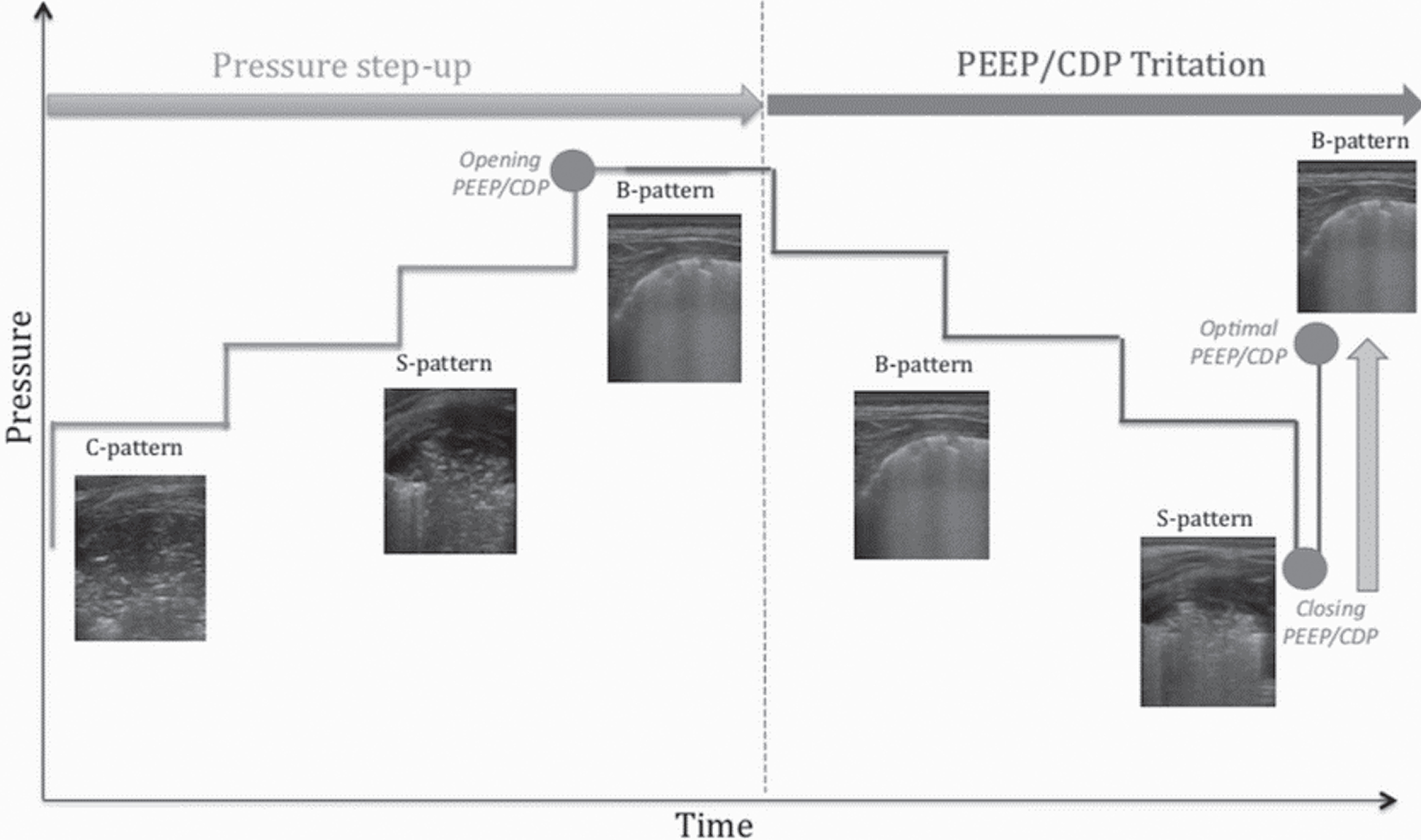
Lung ultrasound (LUS) guided recruitment procedure. The first phase of the LUS guided recruitment maneuver is the stepwise pressure increase, aiming to find the opening pressure, either positive end expiratory pressure (PEEP) on conventional ventilation or continuous distending pressure (CDP) on high frequency oscillatory ventilation (HFOV). During this process, the LUS C-pattern shifts towards the S-pattern and then into a B-pattern (opening PEEP/CDP). Then the PEEP/CDP titration phase begins. PEEP/CDP is decreased until a S-pattern reappears (closing PEEP/CDP), suggesting that the pressure is becoming too low to maintain the lung well-aerated. PEEP/CDP is then increased again until the S-pattern vanishes, and the B-pattern reappears (optimal PEEP/CDP).
Table 1 summarizes patient characteristics, presentation and modification related to the LUS guided recruitments. Case description and the specific features of each LUS guided recruitment are reported.
Characteristic of the study population and recruitment procedures
Characteristic of the study population and recruitment procedures
Gestational age (GA), Birth weight (BW), Meconium aspiration syndrome (MAS), Hypoxic ischemic encephalopathy (HIE), Late onset sepsis (LOS), Extremely low birth weight (ELBW), Late preterm (LP), Pulmonary thromboembolism (PTE), Adult respiratory distress syndrome (ARDS), Pulmonary interstitial emphysema (PIE), High frequency oscillatory ventilation (HFOV), Pressure control-assist control (PC-AC), Lung recruitment (LR), Fraction of inspired oxygen (FIO2), Peripheral capillary oxygen saturation (SpO2), Continuous distending pressure (CDP), Positive end expiratory pressure (PEEP), Ultrasound (US), Oxygenation saturation index (OSI), Heart rate (HR), Mean Arterial Pressure (MAP).
At the onset of the thrombotic event, the infant’s conditions suddenly deteriorated with suboptimal SpO2 (50%) on high frequency oxygen ventilation (HFOV) (Sensor medics 3100A, Carefusion), CDP 21 cmH2O, FiO2 1. LUS revealed a bilateral atelectasis involving the upper and lower lobes in the anterior and posterior lung regions. Therefore, a LUS-guided recruitment maneuver was attempted (Fig. 3). The SpO2/FiO2 ratio improved from 53 to 194. During the procedure, after increasing the pressure two intervals, the re-opened lung units created air artefacts, which started from the re-opened bronchi (Fig. 3b). We named these artefacts “sunray lines” (S-lines) as they resemble sunrays crossing the clouds. After increasing the pressure another two intervals, the S-lines increased and became the most prominent feature of the LUS image. We named this sonographic pattern, with more than two S-lines per field, an S-pattern.

Discrimination between recruitable and non-recruitable lung on lung ultrasound (LUS). a-b) LUS imagining obtained from patient 1 (recruitment 1) a) Transverse LUS section showing lung consolidation (C-pattern) with evident air bronchogram (arrowheads) before starting the lung recruitment maneuver on high frequency oscillatory ventilation (HFOV) at a continuous distending pressure (CDP) of 21 cmH2O. b) Sunray (S) lines (asterisks) develop during the recruitment maneuver at the increase of CDP, shifting from C-pattern to S-pattern (CDP 25 cm H2O). The S-lines represent air artefacts that start from the reopened bronchus (arrowhead), indicating alveolar recruitment. c-d) LUS i m agining obtained from patient 4 (recruitment 4) c). Longitudinal LUS section showing a C-pattern with air bronchogram (arrowheads) before starting the lung recruitment maneuver on high frequency oscillatory ventilation (HFOV) at a pressure of 13 cmH2O. d) In this patient the CDP increase only resulted in a further increase in air bronchogram (arrowheads), with no S-pattern developing (CDP 17 cmH2O). This implies that only the dead space (bronchi) is recruited without alveolar reopening, suggesting a non-recruitable lung.
The onset of septic shock led to a respiratory deterioration with a FiO2 increase from 0.47 to 1 to maintain suboptimal SpO2 (approximately 87–89%) on HFOV (VN500, Draeger) with CDP 13 cmH2O. A standard oxygenation-based lung recruitment maneuver was attempted in the supine position, increasing CDP from 16 cmH2O up to 25 cmH20, but with no clinical improvement. CDP was then decreased to pre-procedure settings by two-minute pressure intervals.
In the following hours, the respiratory conditions deteriorated further with the SaO2 decreasing to 80%. A LUS evaluation detected wide unventilated areas in the posterior lungs, with bilateral posterior C-pattern. The anterior fields showed a normal A-pattern with sparse B lines. Given the sonographic distribution of lung decruitment and the failure of the standard oxygenation-based lung recruitment when performed in the supine position, the infant was placed in the prone position. Following a lack of improvement after 30 minutes in the prone position with the same ventilator parameters, a LUS-guided recruitment was started. CDP was increased from 16 up to 28 cmH2O, while obtaining substantial improvement in the SpO2/FiO2 ratio from 80 to 219. Similar to the previously discussed case, S-lines appeared after one pressure interval increase, and the S-pattern developed after three further pressure interval increases. The S-pattern transformed into a white lung image at the end of the recruitment maneuver.
In this case, the standard lung recruitment in the supine position failed, as the pressure was directed towards the normally aerated ventral areas. Once the dorsal lung was examined, the significant posterior atelectasis could be detected. While not sufficient by itself, the subsequent prone positioning, prompted by the LUS visual aid, dramatically enhanced the effectiveness of the lung recruitment maneuver and the clinical conditions of the patient. This result was likely due to the pressure recruitment being targeted towards the most collapsed areas of the lung.
Lung recruitment procedure number three, performed on a preterm infant suffering from a life-threatening pulmonary interstitial emphysema: Guidance of the PEEP/CDP titration phase
At ten days of life, while on conventional ventilation (VN500, Draeger), and after repeated unsuccessful attempts to wean mechanical ventilation, a LUS showed a right upper lobar atelectasis. Thus, after positioning the infant on the left side, a LUS-guided recruitment was started. PEEP was increased from 5 to 8.5 cmH2O with sonographic and clinical improvement. During the stepwise pressure increases, sparse S-lines developed after two pressure intervals and the S pattern after three pressure intervals. S-pattern resolution developed into a B -pattern (video 1). During the stepwise PEEP reduction, LUS-monitoring identified a partial collapse of the reopened parenchyma (closing pressure) 1 cmH2O below the opening PEEP, despite a stable SpO2. In our experience, the closing pressure was documented as the conversion from B-pattern into the S-pattern (some open bronchi with partial collapsed parenchyma). Another lung recruitment was performed with slower pressure interval step-down (five minutes each), in an attempt to titrate PEEP to a lower level. After the prolonged LUS-guided pressure step-down, the closing PEEP was revealed to be substantially lower (going from 7 to 4.4 cmH2O) and the optimal PEEP was found at 5.5 cmH2O, improving the SpO2/FiO2 ratio from 216 to 282. The baby was extubated two days later.
The use of LUS as direct, real-time morphological monitoring permitted us to refine the procedure during the PEEP titration phase of lung recruitment and allowed us to find a more accurate optimal closing PEEP.
Lung recruitment procedure number four, performed on an infant suffering from a viral bronchiolitis, complicated by bacterial pneumonia: The evidence of unrecruitable lung
The day after admission, the infant required intubation and mechanical ventilation with an oxygen requirement of 70% on HFOV (VN500, Draeger). LUS showed a wide left lung consolidation (Fig. 3c). After repositioning the infant onto the right side, a LUS-guided recruitment was attempted. During the two stepwise pressure increases, a significant increase in air bronchogram was visualized. However, despite a modest improvement in the SpO2/FiO2 ratio, S-lines and S-pattern could not be visualized (Fig. 3d). The maneuver was stopped after four pressure intervals due to the absence of an S-pattern, which suggested that no distal lung recruitment was possible. Subsequently, the blood work and the clinical picture confirmed that bacterial pneumonia was the cause of the lung consolidation, which is not responsive to pressure recruitment. The pulmonary and clinical picture improved 24 hours after the start of the antibiotic treatment. In this case a LUS pattern allowed for the early termination of a potentially counterproductive lung recruitment therapy.
Discussion
We described four LUS-guided recruitment maneuvers that highlight some specific features of this technique, which can be used to improve the effectiveness of the procedure.
The S-pattern identifies the recruitable lung early, supports significant pressure step-up
LUS may represent a convenient and safe method to obtain lung expansion through a highly targeted PEEP/CDP. The visualization of lung re-aeration allows for the detection of the best pressure for each specific lung condition. Presently, the fear of causing a pneumothorax and volutrauma, due to the lack of lung function monitoring, often limits the use of lung recruitment pressure in neonates. Although higher opening CDP have been sporadically mentioned [4], most of the articles reported a maximum value of 20 cmH2O on HFOV for opening CDP during neonatal lung recruitment [9–11]. In most of our cases the minimal pressure to obtain LUS evidence of the de-recruitment resolution (disappearance of the C-pattern on LUS) was well beyond the described values. The stepwise increase of pressure was supported, in our experience, by the sonographic evidence of lung recruitability. We described the shift from C-pattern to S-pattern (Fig. 3a-b) as the sign of lung recruitability. The S-pattern can only be visualized in the presence of recruitable lung, as it represents the sonographic counterpart of the anatomical distal lung unit aeration. The pattern appears early in lung recruitment, after few intervals of pressure increase (2–4 cmH2O). Although the presence of ring down artefacts, has been previously mentioned [12], we believe that the definition of a specific pattern that allows for early identification of the recruitable lung is important in order to identify the patients that can benefit from the procedure. Additionally, including the presence of the S-pattern as a condition to continue the lung recruitment in the LUS-guided recruitment protocol may improve the success rate of the procedure.
The LUS guided patient positioning allows for the PEEP/CDP to be directed towards the most derecruited areas and avoid “healthy” lung over-distension
Another advantage of the LUS guided recruitment is the spatial detection of lung de-recruitment and consequential guidance of patient positioning in order to optimize pressure direction, according to the gravity-dependent lung physiology [13, 14].
We show that a comprehensive LUS examination can change the success of the ventilatory strategy, especially when an inhomogeneous lung is anticipated. Chest x-ray may be misleading in intubated patients [15], since it basically reflects the aeration of the ventral lobes. In adult patients, major lung volume loss can be identified on a CT scan, despite their roughly normal appearance on a chest x-ray [16]. However, in the NICU, where the CT scan is rarely performed, the precise location of the aeration loss identified on LUS may be crucial to improve the outcome of the ventilator strategy. Proper position, according to lung decruitment, allows the PEEP/CDP to be targeted towards the derecruited areas and lower the over-distention of the better aerated segments. This strategy reduces the possible hemodynamic compromise due to vascular return compression. In our patients, pulmonary blood flow was stable throughout the maneuver (data not shown). Initially, we allowed for some time in prone position before starting the lung recruitment, as it is described that positioning alone may be sufficient to re-aerate a collapsed lung [17]. However, in our case, patient positioning was not enough.
We believe that the definition of the best patient position, based on the LUS evidence of the most dependent region, should be part of the LUS-guided recruitment protocol. Patient positioning should be well defined and described, as it may change the progression of the procedure.
The early appearance of the S-pattern during the PEEP/CDP titration phase may suggest that longer pressure steps are required
The optimal PEEP/CDP titration time has not been determined yet. While lung recruitment allows for the reopening of collapsed alveoli, the redistribution of surfactant and stabilization of the airless lung units may take an unpredictable amount of time [18]. The dynamic changes in lung compliance differ depending on pulmonary characteristics, the type of lung disease and duration of the atelectasis. In our experience, opening and closing PEEP/CDP that are close in value may suggest that a prolonged PEEP/CDP titration is required in order to allow for surfactant redistribution and find the optimal lowest PEEP/CDP. During pressure step down, the conversion of the B pattern into the S pattern defines the closing PEEP/CDP, as the S-pattern represents the presence of some collapsed bronchi within an otherwise aerated lung. In particular, the appearance of an early S-pattern, during pressure interval step down (1-2 cmH2O from opening PEEP/CDP) suggests that a prolonged PEEP/CDP titration is needed in order to further reduce the transpulmonary pressure.
The absence of the S-pattern is an early marker to identify unrecruitable lung
Currently, given the lack of more sophisticated tools, lung recruitment in neonates is performed adjusting the opening and closing pressures based on relative changes in SpO2. However, recruitability and oxygenation, contrary to common belief, are usually weakly correlated [6]. For a fixed FiO2, oxygenation depends on both the components of the ventilation/perfusion ratio. It has been shown that the improvement in oxygenation, obtained with PEEP increases, in an unrecruitable lung may be a result of the decreased perfusion due to the compression of the vascular lung compartment by the over-distended and over-recruited dead space, rather than a result of the improved ventilation [16]. This ultimately leads to a transient improvement in oxygenation, at the expense of potential damage to the lung. With the aid of LUS, this risk is reduced, as LUS can distinguish recruitable from unrecruitable lung, avoiding potentially counterproductive recruitment maneuvers when not indicated. We observed that the increased presence of air bronchograms without the development of the S-pattern (Fig. 3c-d) indicates that the lung is not being recruited by the pressure interval increases, while the dead space is. We believe that the absence of the S-pattern could be included in the LUS-guided recruitment protocol as the sign to discontinue an ineffective maneuver early on.
Limitations
Our report has several limitations, including the retrospective nature of the series and the technical impossibility to compare the LUS results with gold standard pulmonary measurements or CT scan imaging. Given the lack of a gold standard for lung mechanic monitoring in the neonatal setting, in order to avoid volutrauma, we interrupted pressure step-up as soon as the LUS sign of lung consolidation disappeared, and the B-pattern was obtained. It is possible that higher pressure might have been necessary to obtain full recruitment of the most peripheral lung units. On the other hand, since LUS cannot detect over inflation, it cannot be excluded that regional over distention had occurred in our patients, although no hemodynamic changes were detected during the maneuver.
This is only a small case series, with a heterogeneous group of patients despite a similar US pattern, therefore no definitive conclusion can be drawn based on our report. Future studies are needed to assess if LUS guided PEEP/CDP titration timing based on the early appearance of the S-pattern can improve the outcome as well. Lastly, it must be mentioned that LUS is an operator-dependent technique [1].
Conclusions
We describe 4 lung recruitment maneuvers that each show a specific, novel feature of the LUS guided recruitment in neonates. Following validation, our findings could be taken into account to improve the LUS-guided recruitment protocol and ultimately the efficacy and safety of the procedure. Given the fact that this is a novel field in neonatal ventilation, this report on the importance of optimize patient positioning, PEEP/CDP titration, and distinguishing recruitable from non-recruitable lung may open the door for more innovative research and opportunities.
Footnotes
Acknowledgment
We thank Professor Bernard Thébaud for his insightful and bright manuscript revision that substantially improved our report. We thank Ida-Sofia Toivonen and Sabina Strashun for the careful English revision.
Disclosure
The authors have no funding to disclose. The authors declare that there is no conflict of interest.