
Abstract
BACKGROUND:
Timely development of early motor skills is essential for later skill development in multiple domains. Infants with severe bronchopulmonary dysplasia (BPD) have significant risk for developmental delays. Early motor skill development in this population has not been described. The aim of the present study was to characterize motor skill acquisition at 3 and 6 months corrected age (CA) and assess trajectories of skill development over this time period in infants with severe BPD.
METHODS:
We performed a single-center, retrospective descriptive study. Motor skills were categorized as present and normal, present but atypical, or absent at 3 and 6 months CA. Logistic regression was used to identify clinical characteristics associated with negative trajectories of skill acquisition.
RESULTS:
Data were available for 232 infants and 187 infants at 3 and 6 months CA, respectively. Ten motor skills were present and normal in 5–44%(range) of subjects at 3 months. Nineteen motor skills were present and normal in 1–63%(range) of subjects at 6 months. Significant postural asymmetry was noted throughout the study period. Loss of skills and worsening asymmetries over time were common. Exposure to sedating medications was significantly associated with poor development.
CONCLUSION:
We report delays in motor skill acquisition and postural asymmetries in infants with severe BPD at both 3 and 6 months CA. The association between sedating medications and poor development suggests that efforts to limit these exposures may lead to improved development. Targeted interventions to facilitate early motor development may improve outcomes of this high-risk population.
Keywords
Abbreviations
Bronchopulmonary dysplasia Corrected age
Introduction
Bronchopulmonary dysplasia (BPD) is associated with poor neurodevelopmental outcomes, including cognitive and motor deficits, throughout childhood [1]. In very preterm infants, BPD is an independent risk factor for adverse development that is similar in magnitude to severe brain injury and retinopathy of prematurity [2]. Yet, BPD is far more common than these other morbidities [3]. BPD is associated with more than two-fold increase in odds of death or neurodevelopmental impairment at 18 months corrected age [2]. The impact of BPD on neurodevelopment correlates with the degree of lung disease; children with the most severe forms of BPD are at the highest risk for poor outcomes [1, 4].
Timely development of early motor skills is essential because they are the foundation on which later motor, cognitive, and perceptual skills are built [5, 6]. Theoretical frameworks posit that early motor development depends on factors inherent to the child, such as state of health, and factors in the environment, such as the availability of toys [7]. Infants with severe BPD have limited opportunities to experience and respond to the normal stimuli in their environment. Sedating medications, lack of positive sensory stimuli, medically necessary restrictions to normal movements, and stress all interfere with normal sensorimotor experiences. Despite the recognized developmental risks posed by prolonged intensive care and chronic respiratory illness, early motor skill development in infants with severe BPD is not well characterized.
In the present study, we aimed to characterize motor skill acquisition at 3 and 6 months corrected age (CA) and assess trajectories of skill development over this time period in infants with severe BPD. An improved understanding of early motor patterns in infants with severe BPD may provide insight into opportunities for novel interventions to improve outcomes in this medically complex population.
Methods
We performed a retrospective descriptive study of early motor development in infants with severe BPD receiving intensive care between January 1, 2014 and June 1, 2019 and referred to our quaternary-level neonatal and infant intensive care unit for multidisciplinary BPD care. Infants who died before 3 months CA were excluded.
A physical therapist and occupational therapist on the study team (MB, AW) abstracted data from all therapy and physician notes during the one week periods after the infants reached 3 and 6 months CA (“3 and 6 month CA assessment timepoints”). If the infant had an acute illness or surgery during this time period, data collection was deferred until the infant returned to his or her baseline state of health. Outpatient therapy, child development, neurology, neonatal follow-up and other relevant medical encounters were reviewed to assess post-discharge development among the infants who were no longer hospitalized at study assessment timepoints. The date of the last note reviewed and inpatient or outpatient status were documented for each time period.
Assessment of motor development was performed with a standardized checklist and included documentation of skills and postural asymmetries. We collected data on 10 motor skills at 3 months CA and 19 motor skills at 6 months CA, using pre-specified definitions. Motor skills were categorized into one of four levels: (a) present and normal for CA, (b) present but atypical, (c) not present, or (d) not documented. For example, head in midline skills were defined as present and normal if the infant was “able to sustain head in midline at least 2 seconds in spine or upright sit,” whereas the skills were defined as present but atypical if the infant had “head preference to right or left, torticollis, or cervical extension preference.” Postural asymmetry is a deviation from neutral alignment of the body that may present at rest or when the infant is posturally challenged. Postural asymmetries can occur in the head, trunk, upper extremities, hips/pelvis, and lower extremities. For example, asymmetries of the upper extremity include scapular elevation, retraction, external rotation and forearm pronation. Postural asymmetries were categorized as present, absent, or not documented. Before the complete record review, 20 infants’ records were reviewed independently by two investigators to establish inter-rater agreement for categorization of motor skills and postural asymmetries.
Exposure to sedating medications and degree of respiratory support at the 3 and 6 month CA assessment timepoints were abstracted from the electronic medical record. Sedating medications were defined as any opioid, benzodiazepine, or other medication administered for the purpose of sedation, anxiolysis, or pain control. Infants prescribed continuous intravenous infusions, standing intermittent intravenous doses, or standing enteral medications were classified as exposed. Respiratory support was categorized as none, low noninvasive (≤2L nasal cannula), high noninvasive (> 2L nasal cannula or any noninvasive positive pressure), ventilation via endotracheal tube, or ventilation via tracheostomy.
Standard statistics were used to describe characteristics of the study cohort and motor skills and postural asymmetries at the 3 and 6 months CA assessment timepoints. Longitudinal trajectories were assessed among infants for whom data were available at both 3 and 6 months CA. Trajectories were categorized into three levels; (1) always normal; (2) improving, if the skill was absent or atypical at 3 months CA and normal at 6 months CA or if a skill was absent at 3 months CA and present but atypical at 6 months CA; and (3) abnormal/worsening, if the skill was absent or atypical at both time points, if a normal skill became atypical or was lost, or if an atypical skill was lost. Trajectories were further dichotomized as positive (always normal or improving) or negative (abnormal/worsening). Logistic regression was used to evaluate associations between clinical characteristics and negative trajectories, using positive trajectories (always normal or improving) as the reference. All analyses were performed with STATA/SE 16.1 (College Station, TX) and p < 0.05 was considered significant. This study was granted exemption status by our local Institutional Review Board and patient consent was not required.
Results
Between January 1, 2014 and June 1, 2019, 294 infants received care from our multidisciplinary BPD team. Fifteen were excluded from the current study because they died before 3 months CA. Characteristics of the 279 children included in the current study are provided in Table 1. Nearly half underwent tracheostomy and ten (3.6%) died between 3 months CA and discharge. Medical status at the 3 and 6 month CA assessment timepoints is provided in Supplemental Table 1.
Patient characteristics
Patient characteristics
Motor development data were available for 232 of 279 (83%) patients at the 3 month CA assessment timepoint. Of these, 202 (87%) were inpatients. Of the 47 infants for whom 3 month data were not available, 28 (60%) had been discharged or transferred to another institution and 10 (21%) had not yet been referred to our institution. Of the 273 who survived to 6 months CA, motor development data were available for 187 (69%). Of these, 103 (55%) were inpatients and 84 (45%) were outpatients. Data were available at both timepoints for 165 (59%), one timepoint for 89 (32%), and neither timepoint for 25 (9%) (Supplemental Figure 1).
The majority of infants had not acquired typical motor milestones at either timepoint (Supplemental Table 2). At the 3 month CA assessment timepoint, the 10 distinct skills were categorized as present and normal in between 5%and 44%of infants. At the 6 month CA assessment timepoint, 19 distinct skills were categorized as present and normal in between 1%and 63%of infants. For example, at 3 months, 16%of children could bring their hands together in the midline but only 5%of children could reach for an object or toy in the midline. By 6 months CA, 48%could bring their hands together and 26%could reach in the midline for a toy, but only 12%could reach to the side and only 6%could reach for their feet. Similarly, postural asymmetry was noted in most infants at both timepoints (Supplemental Table 3). For example, 90 and 87%of infants demonstrated postural asymmetries of the upper extremities at the two study timepoints, respectively.
Trajectories of motor skill development between 3 and 6 months CA
Trajectories of eight motor skills were assessed in the 165 infants for whom data were available at both timepoints (Fig. 1). A minority of infants had normal skills at both timepoints. Between 29%and 52%of infants had persistently absent or atypical skills or lost skills over time. Similarly, infants without evidence of postural asymmetries at 3 months CA often acquired asymmetries by 6 months CA (Fig. 2). For example, of the 18 for whom asymmetry of the trunk was not noted at 3 months CA, 11 developed truncal asymmetries by 6 months CA.

Early motor milestone trajectories. Percentage of infants who had persistently normal, improving, or persistently absent/persistently abnormal/worsening motor skills between 3 and 6 months corrected ages. Data are provided for 8 skills that were assessed at both points; n represents the number of infants with data at both timepoints for each milestone.
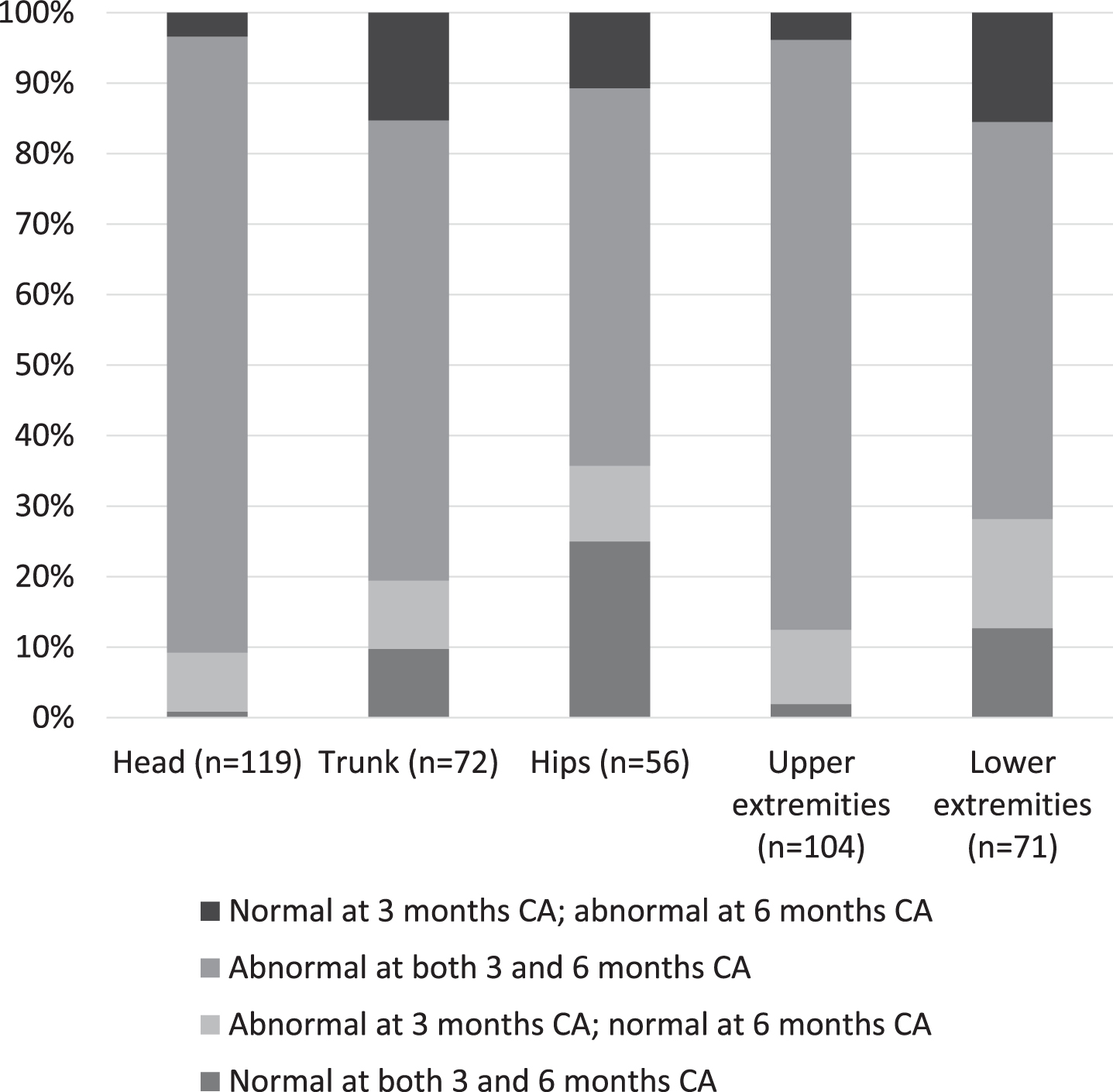
Postural asymmetries at 3 and 6 months corrected ages. Percentage of infants who had persistently normal, improving, persistently abnormal, or worsening postural asymmetries between 3 and 6 months corrected ages. Data are provided for postural tone in 5 areas: head, trunk, hips, upper extremities, and lower extremities; n represents the number of infants with data at both timepoints.
Exposure to sedating medications at either 3 or 6 months CA was significantly associated with negative trajectories of motor skill acquisition (Table 2). For example, infants who received sedating medications at both timepoints, compared to those who were free of treatment at either timepoint, had a 7.2 (2.7–19.2) times higher odds of a negative trajectory for midline hand skills. The level of respiratory support administered at 3 and 6 months was significantly associated with negative trajectories for visual fixation and tracking (Table 2). The level of respiratory support at 6 months was significantly associated with negative trajectories for midline head and hand skills. When both level of respiratory support and exposure to sedating medications were included in the same models, only medication exposure was associated with trajectories of acquisition of some motor skills (data not shown). Inclusion of gestational age in these models did not substantively alter the results.
Odds ratios for negative trajectories of motor skill acquisition, based on clinical characteristics at 3 and 6 month corrected age assessment timepoints
*Reference group is infants without medication exposure at either timepoint. #Reference group is infants on no support or on nasal cannula≤2LPM.
Severe BPD is a risk factor for poor neurodevelopmental outcomes in early childhood [1, 9]. Motor abnormalities in children with BPD persist at least until school age and are manifested as cerebral palsy as well as problems with both fine and gross motor coordination [10–12]. Motor skill acquisition is often delayed or atypical in children with BPD, as demonstrated in prior studies using the Bayley Scales of Infant Development at 12–36 months CA and the Hammersmith Infant Neurological Examination at 6 and 12 months [13–15]. However, the magnitude and severity of aberrations in early motor development in this population are not well described.
More than 90%of children included in the current study were intubated or on positive airway pressure at 39 weeks PMA, when they were transferred to our institution. Thus, the preponderance of this cohort would have met the Jensen criteria for grade 2 or grade 3 BPD, indicating high risk for respiratory and neurodevelopmental sequelae [4]. We provide novel, granular data about the timing and progression of early motor skill acquisition in this unique population. We observed that not only do infants with severe lung disease show delayed acquisition of many critical motor skills compared to age-specific norms, but these skills often develop atypically. The delay in motor skill acquisition is associated with frequent and often persistent postural asymmetries. Moreover, between 3 and 6 months CA, many infants lose skills, skills develop atypical features, and postural asymmetries emerge.
Infants depend on early motor skills to develop more advanced motor, cognitive, and perceptual abilities [5, 6]. For example, development of postural control is fundamental to later motor, cognitive and language skills [6, 7]. Adequate vestibular, haptic, auditory, and visual input through movement and interaction with the environment are essential for supporting development of more advanced motor skills. In animal models, deprivation from sensory or motor experiences leads to permanent loss of function [16]. In contrast, when animals are raised in complex housing with large social groups, they demonstrate increased brain development and increased motor, sensory, and cognitive functions [16]. In functional MRI studies of preterm human infants, early life experiences are associated with both maturation of sensory-motor function and brain structural development [17]. For example, when preterm infants between 31 and 34 6/7 weeks are imaged at the same post-menstrual age, increasing postnatal age is associated with increasingly bilateral patterns of functional response to passive motor tasks [17]. In a systematic review, environmental enrichment was associated with a small but significant improvement in the motor development of infants at high risk for developing cerebral palsy [18]. Along with appropriate stimulation and environmental factors, factors inherent to the child exert influence on early motor development [7]. Beginning at 3 to 4 months CA, infants use exploration and trial and error to learn how to stabilize and move their bodies to interact with their environments. In the current study of infants with severe BPD, significant abnormalities in postural control and poor acquisition of motor milestones were apparent by the 3 month CA assessment and often persisted or worsened by 6 months CA. Protracted medical illness, coupled with insufficient opportunities to experience and explore the environment, likely led to the identified deficits. These deficits in foundational skills likely have implications not only for more advanced motor development but also for development in multiple domains.
The severity of BPD correlates with the severity of neurodevelopmental impairment in early childhood [1, 15]. In addition, duration of exposure to both mechanical ventilation and noninvasive ventilation are independent predictors of neurodevelopmental outcomes [8, 9]. In our cohort of infants, the majority of whom had severe lung disease and chronic ventilator dependence, negative trajectories of motor skill acquisition were more strongly and consistently associated with routine exposure to sedating medications than with the level of respiratory support. One interpretation of this finding is that infants with severe BPD should be provided sufficient respiratory support to enable comfort and participation in developmentally appropriate activities with minimal sedation. This is consistent with prior research by our group demonstrating that infants receive less medication for sedation and are able to participate more fully in therapy focused on acquisition of motor milestones following tracheostomy [19].
Motor therapies, specifically occupational and physical therapy, are an essential component of multidisciplinary care for infants with BPD. Therapy should be implemented early during the neonatal hospitalization and continue throughout the entire hospital stay. Early implementation of interdisciplinary programs that integrate therapy services has been associated with improved performance on the Bayley Scales of Infant Development at 18–24 months [20]. Therapy services in the neonatal intensive care unit can be initiated even if the infant still requires high levels of respiratory support, including intubation. It is common for therapy in this group of infants to focus on supporting patient care tasks and state control [19]. As respiratory status improves, therapies transition from activities that promote physiologic stability to activities that promote skill acquisition. Doing so at the earliest safe timepoint may minimize the risk of skill loss observed in the current study.
While facilitating the development of early motor skills, therapists must also pay close attention to postural deformities that may impact skill acquisition. Atypical postures related to excessive activation of respiratory musculature include elevated and retracted scapulae, cervical hyper-extension, limited trunk mobility and a flatter chest [21]. Such asymmetries of the upper extremities and trunk were commonly noted in the current study. Additionally, we identified frequent head shape deformities, head preferences including torticollis, spinal curvature anomalies, and gravity dependent positioning of the upper and lower extremities. A strategy to address these evolving deformities is to implement early progressive mobility, while monitoring infant behavioral states to ensure that the infant is tolerating position changes [22, 23]. Early mobilization provides opportunities for increased participation in upright positioning and development of postural control [24]. Collaboration between the medical team and therapists is critical to ensure that the level of respiratory support administered is adequate to facilitate implementation of early progressive mobility.
Targeted developmental interventions post-discharge improve motor and other neurodevelopmental outcomes [25, 26]. Therefore, infants with severe lung disease require referrals to outpatient services including early intervention, outpatient physical and/or occupational therapies, and NICU follow-up clinics. Parent and caregiver education is essential to ensure carry-over of therapy plans including developmental positioning, age appropriate stimulation, stretching and ROM exercises, and increased participation in play and movement activities in the home environment. Importantly, parent provided interventions are effective for promoting developmental skill acquisition in premature and high-risk infants, with effects sustained through at least the first few years of life [25, 27–29]. Because early intervention is an effective, evidence-based tool for improving motor outcomes, it is essential to identify precursors to later motor delays and target therapies to high-risk infants [25, 30]. Infants with deficits such as those identified in the current study are likely to benefit from ongoing therapy post-discharge.
Our study is limited by its retrospective design. The presence or absence of all evaluated skills and postural asymmetries were not documented for every infant, and motor data were incomplete among the small number of infants who were admitted after 3 months CA or discharged before 6 months CA and not seen in follow-up. Because most infants are several months old by the time they are transferred to our institution, we do not have consistent data about perinatal factors such as intrauterine infection or early respiratory characteristics which may be related to the severity of lung disease. Due to lack of clear evidence in the literature to drive our practice, we do not have a standardized approach to use of sedating medications in our NICU. Finally, we did not quantify level of respiratory support and medication exposure throughout the study period; rather, we used data from the 3 and 6 month CA assessment timepoints to represent each infant’s clinical condition during that time period. At times, this may have not been fully representative of the degree of intensive care provided.
Despite a small amount of missing data, we employed robust data collection methods to ensure high-quality study data. The therapists who provide inpatient and outpatient care for patients with BPD in our institution did not use a standardized, validated motor assessment during this time period; however, they consistently utilized a standardized template for routine clinical documentation of infant motor skills. The same therapists reviewed the electronic medical record in order to ensure that data for as many skills as possible was collected. Rigorous assessment of clinical data such as in the current study is critical for driving evidence-based decisions about incorporation of validated motor assessments into clinical care. Reliability of the data abstraction process was established before all study data were collected.
In conclusion, infants with severe BPD at our institution have significant delays in motor skill acquisition and postural control that can be detected as early as 3 months CA and persist through at least 6 months CA. In future work we will assess relationships between these early skills and motor and cognitive development at 2 years CA. Ultimately, targeted interventions to facilitate development of specific early motor skills may improve outcomes of this high-risk population.
Sources of financial assistance
None
Conflicts of interest
Nothing to declare