
Abstract
INTRODUCTION:
Few studies exist that research the association between umbilical cord characteristics with cardiac malformations. In this study, we describe a population of newborns with congenital heart defects (CHD) and the frequency of presentation of umbilical cord (UC) alterations, based upon the hypothesis that the continuity of the cardio-placental circuit can be affected by similar noxas during early development.
METHODS:
We carried out a descriptive study at a hospital in Bogota based on clinical records from newborns with congenital heart disease with placental and UC pathology results. Group analyses were done according to the major categories of the ICD-10.
RESULTS:
We analyzed 122 cases and found that the most frequent alterations where hypercoiling (27.9%) and abnormal UC insertion (16.4%). Additionally, in almost every group of CHD, more than 65%of patients had some type of cord alteration.
CONCLUSION:
We discovered a high frequency of UC alterations in patients with CHD. This outcome suggests that a possible association exists between the two phenomena, further research is needed.
Introduction
In the fetus-placenta-mother relation with the fetal heart, the umbilical cord (UC) functions as an extracorporeal extension of the fetal vascular system. Abnormal UC diameter, length, blood pressure or blood viscosity, may lead to insufficient fetal cardiac output, blood stasis or thrombosis, and, ultimately, to fetal death due to heart damage [1]. Furthermore, a number of other specific UC and related functional abnormalities can lead to morphological deformities, neurological anomalies and obstetric and neonatal complications that may adversely affect the development of both the fetus and the newborn, oftentimes resulting in perinatal mortality [1–5]. One such case occurs when long umbilical cords compound heightened perfusion pressure and greater flow resistance that together aggravate fetal vascular perfusion, thus triggering myocardial hypertrophy and fetal cardiomegaly [6–8]. Additionally, in many autopsies performed on newborns with acute complications, the apparent cause of death can often only be attributed to an excessively long UC [5]. It is reasonable to surmise that these abnormalities stem from organogenesis, since genetic patterns determine the formation and development of living beings. However, physical factors in the growth environment may also play a part in organ abnormalities [9]. The results of experiments in animals demonstrate that hemodynamic changes in the extra-embryonic circulatory systems, in vitelline membranes and in placentas can disrupt normal cardiac development [9–12]. At the molecular level, regulatory signaling pathways, such as those mediated by Nkx2.5, ASXL1 y 2, GATA4, Hand1, Hand2, T-box y MEF2, determine normal cardiac embryology. For example, Nkx2.5 triggers cardiogenesis after prompting from the proteins Wnt, BMP and FGF [13], which in turn function under the guidance of proteins FGFH and FGF2. Any alteration that takes place along these signaling pathways will ultimately be a major factor in the manifestation of CHD [14–16]. In addition, VEGF-R1 plays an important role in both UC and fetal circulatory system angiogenesis, and any malfunction in this protein will contribute to fetal and newborn abnormalities [17].
Some evidence relates mechanical factors and fetal cardiovascular development. One study in animals that focused on the irregular laminar flow between heart chambers revealed that biventricular disorders stemmed from abnormal heart and coronary artery morphology and deformities. Studies on the relation between the fetal circulatory system and congenital heart disease link irregular shearing stress to disruptions in genetic expressions KLF-2, ET-1 and NOS-3 [9]. Moreover, as the fetus grows, abnormal UC width, length and coiling may affect vascular development, thereby causing CHD [1, 18]. Ultimately, the cause of some congenital heart disorders has been associated with abnormal umbilical venous circulation; especially, fetal vascular malperfusion, which can increase risk of heart malformation by up to six times over the normal rate. However, research has yet to determine the causal chain for these events [19].
The present study set out to describe UC characteristics in patients with congenital heart disease, as well as to identify UC abnormalities present at birth, and their connections to congenital heart defects. In order to understand how these phenomena, along with the signaling pathways involved, influence the development of the fetal heart and circulatory system, we focused on the importance of the biological relations described above, as well as on UC embryonic genesis.
Methods
We carried out an observational descriptive study on cases of newborns with CHD diagnosed at the Hospital Universitario San Ignacio (HUSI) in Bogota, Colombia. Our study combined a mixed timeframe that shared a retrospective component (2008–2018) with a prospective component (2019). The project was approved by the Institutions Ethics Research Committee approval number 2019/052. Due to the study being observational and since no patients were contacted the IRB waved the need for a consent form. At study outset, we searched for cases-of-interest among diagnosed neonatal patients classified under ICD10 criteria, in categories ranging from Q20 to Q28. Definitive study inclusion required postnatal diagnosis confirmed by echocardiogram as the gold standard. We then uploaded collected data to a REDCap database.
We should point out that we did not specifically perform the placental pathology analysis just for this study: They existed before our study began, and had been ordered in accordance with international diagnostic guidelines for cases of infant heart disorders.
We grouped UC alterations (Fig. 1) according to classification guidelines found in the literature [2, 21]. We also collected information regarding Apgar scores, childbirth risks [22–24], intrauterine growth restriction [25] and parental age [26, 27]. In collecting data on UC measurements, we employed the method developed at HUSI [1].
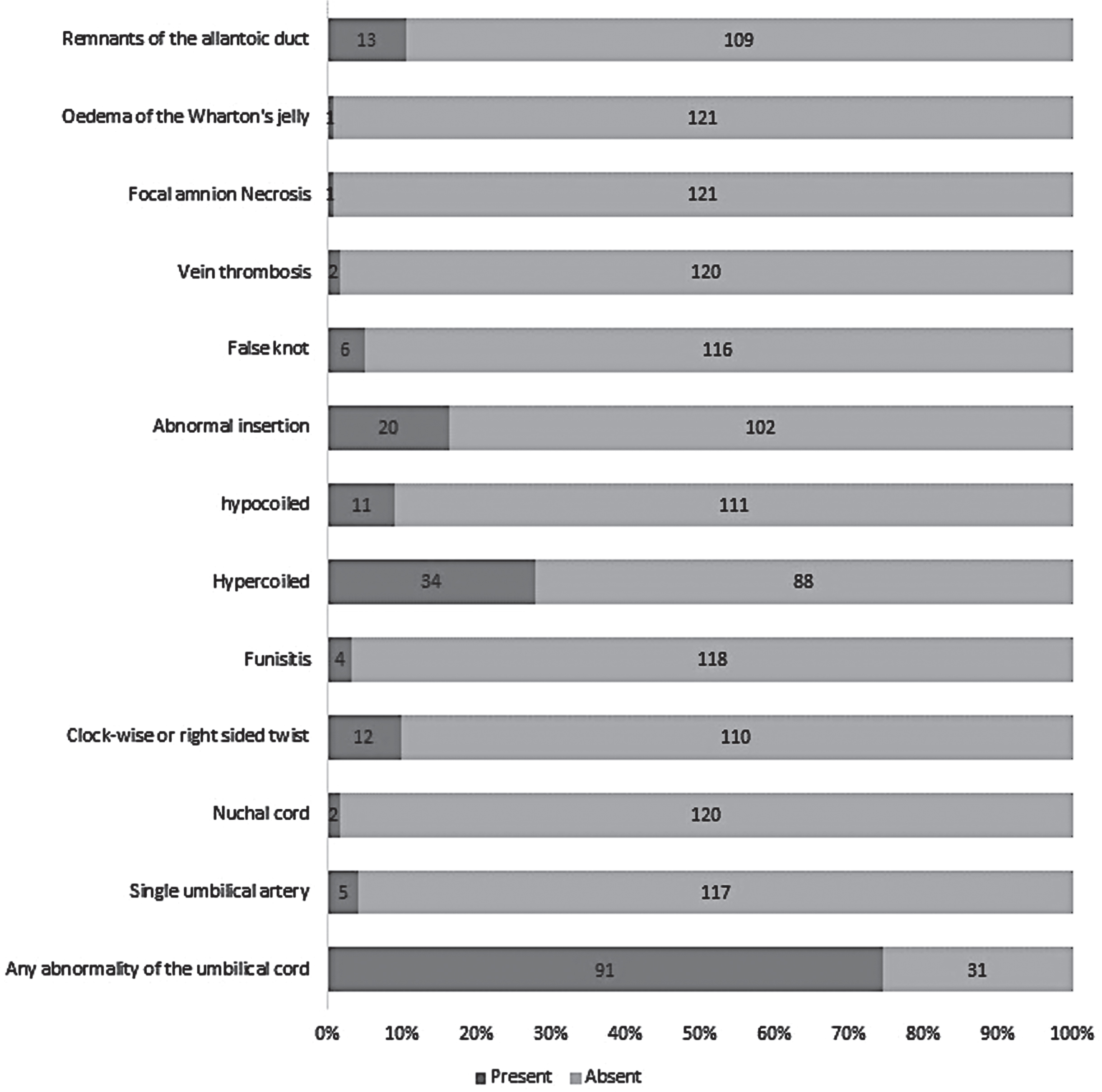
Umbilical cord findings.
We utilized absolute and relative frequencies to summarize analyses of qualitative variables; we identified distribution of quantitative variables (maternal, paternal and fetal ages) with frequency graphs. We described numerical variables in medians, accompanied by percentiles 25 and 75 to capture dispersion. Afterwards, we laid out numerous associations that might link congenital heart diseases to UC alterations. We used R 3.5.0 software to carry out statistical analysis.
We proceeded to identify 459 potential cases, out of which we eliminated duplicates, and selected only cases whose diagnoses had been confirmed by both postnatal echocardiogram and complete placental and UC histopathology reports. A total of 122 cases qualified for study inclusion. Table 1 describes the parental demographics of newborns with congenital heart disease. The most commonly pre-existing maternal conditions were overweight and obesity (n = 15), followed by glycemic alterations and hypothyroidism, (n = 10), with acquired heart disease (n = 8) in third place. One mother suffered from Tetralogy of Fallot.
Clinical characteristics and demographic data of included newborns and parents
Clinical characteristics and demographic data of included newborns and parents
STORCH† disease group comprising syphilis, toxoplasmosis, other infections, rubella, cytomegalovirus infection, and herpes simplex, IUGR‡ Intrauterine growth restriction, ICD§ International Classification of Disease.
The most common complications during pregnancy included hypertensive disorders of pregnancy (n = 28), risk of abortion or of pre-term delivery (n = 21), premature rupture of membranes and infections (n = 12), most frequently S. agalactiae, which affected 4 expectant mothers.
During hospital stay, 36%of newborns suffered from hyperbilirubinemia, and 33%from pulmonary hypertension. Among patients diagnosed with CHD, 11 had chromosomal abnormalities: Down syndrome (n = 6), Trisomy 13 (n = 2), Turner syndrome (n = 2), Trisomy 18 (n = 1); in this same group of infants, 55%of mothers were over 35, and 17%were affected by an additional severe deformity.
Upon grouping CHD under ICD-10 guidelines, we observed that fifty-percent of congenital malformations corresponded to malformations of the large arteries and malformations of the interventricular septa. In the latter cases, 18%of patients exhibited diagnosis of isolated patent ductus arteriosus. At the end of the hospital stay, 32.5%of patients had died, due to baseline pathology complications; after receiving signed parental informed consent, 10 deceased infants underwent autopsy.
Figure 1 contains the findings on UCs collected from placental pathology reports. It is worth noting that among the eight abnormal-in-length UCs examined (either short or long), range varied from 33.3 cm to 104 cm. UC features were categorized according to what is described in the literature: Abnormal insertions: Marginal, velamentous, furcate (vessels lacking Wharton’s jelly before reaching the placenta), and paramarginal (1 cm or less from placental margin); Abnormal coiling: Normal coiling index: Number of coils divided by the length of cord of between 0.07 and 0.3 turns per cm. We considered hypocoiled cords (coiling index value < 0.07 coils/cm [10th percentile]) and hypercoiled cords (coiling index value > 0.3 coils/cm [90th percentile]). A twist was defined as a full turn (360 degrees) of the vein. These were classified according to the direction of coiling as either counterclockwise (also called left twist), dextrorotatory (clockwise), and bidirectional coiling; the number of cord vessels was counted to find SUA cases; true UC knots and entanglements (cord tangles in fetal body parts) [30].
In a final step, we carried out a bivariate analysis to ascertain how CHD might be related to UC malformations (Fig. 2). In scrutinizing every classified group (with the exception of Q28, which contained only one case), we found that some type of UC deformity was present in more than 65%of patients. See supplemental Table 1 and supplemental Table 2, detail the UC deformities present in each CHD group.
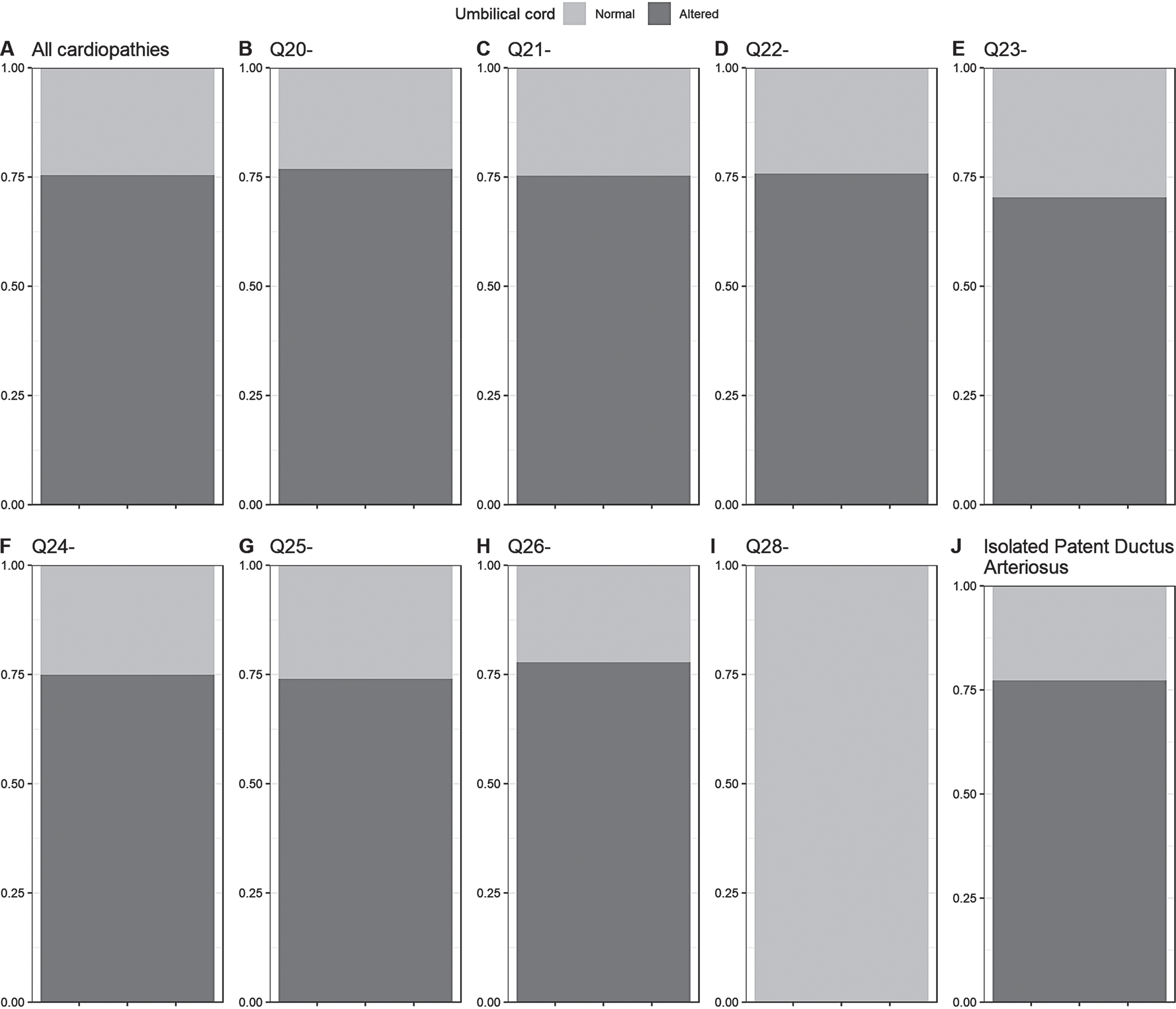
Distribution of umbilical cord alterations by CIE-10 diagnosis. Q20 Congenital malformations of cardiac chambers and connections. Q21 Congenital malformations of cardiac septa. Q22 Congenital malformations of pulmonary and tricuspid valves. Q23 Congenital malformations of aortic and mitral valves. Q24 Other congenital malformations of heart. Q25 Congenital malformations of great arteries. Q26 Congenital malformations of great veins. Q28 Other congenital malformations of circulatory system.
The rate of CHD continues to rise in Bogota, Colombia; currently, it is at 15.1 per 10,000 newborns [28]. In spite of the oftentimes lethal outcomes produced by heart defects (they are one of the major causes of infant mortality), their etiology remains uncertain.
The descriptive study at hand purports to show how UC deformities could be linked to CHD. To that end, we showed that 75%of the newborns with heart defects in our study also displayed some type of UC malformation; especially, those malformations we had described in the initial study protocol. However, in other studies, the average reported rate of UC deformities in infant patients with heart defects does not surpass 61%[29].
Our UC study revealed hypercoiling to be the most frequently occurring abnormality; indeed, 28%of all UC abnormalities fell into this category (n = 34/87). Multiple studies have associated UC hypercoiling with a variety of negative outcomes (fetal death, fetal defects, abnormal insertion). Therefore, many experts believe that this abnormality may serve as a marker of abnormalities that occur during fetal development; particularly, since it increases turbulent blood flow that, in turn, leads to greater peripheral vascular resistance and, ultimately, to asphyxia and stunted intrauterine growth; a fact that further reinforces the suspicion that these conditions are intricately related to one another [30].
However, researchers have been unable to identify the underlying hemodynamic mechanisms that link the above-described pathological relations to one another; nor have they been able to establish the order in which they occur [30]; or whether or not genetic coding determines their appearance [31]. In contrast, studies do exist that demonstrate that even in cases where the placenta is normal, hypercoiling and stunted intrauterine growth occurred; meaning, consequently, that the altered fetal-placental hemodynamic profile must be the only possible explanation for the UC defect [32].
As is well known, mother’s age during pregnancy, especially in women over 35, is an important risk factor that contributes to low fetal or newborn weight, perinatal death, as well as to a greater need for emergency cesarean section [33]. In some Colombian studies on fetal and newborn abnormalities, 13.2%of patient cases occurred among mothers over 35 years of age [29]. In our study, this rate reached 21%, an outcome we had anticipated, considering the notable presence of chromosomal pathologies, and the severity of the defects we encountered. Our registry of maternal endocrinological, vascular and infectious disorders closely resembled that found in other, previously described series [29].
When considering Apgar score among patients born with CHD, other studies showed median score with heart defects of 8 at one minute and 9 at five minutes in 131 newborns [34, 35]. In contrast, in our study, 80%of patients had an Apgar score greater than 7 at one minute, and 97%at 5 minutes.
Limitations and possible biases
Because the study took place at a highly complex medical center, and although the study population included only liveborn infants, many of the patients, both mothers and children, suffered from baseline pathologies and complications that similar patients, in a less complex setting, may not have.
Conclusion
Our study describes the findings on umbilical cords in 122 patients with congenital heart defects. We observed anatomical UC defects in 74.6%of patients with congenital heart defects; hypercoiling ranked as the most common UC deformity. The frequency of UC anatomical alterations found in our study surpassed that found in other studies on UC deformities in consecutive newborns.
The foregoing information may serve to reinforce the thesis that a link exists between anatomical UC deformities and congenital heart defects. A body of the literature connects hemodynamic alterations, such as those caused by UC abnormalities, with heart defects. However, given the nature of our study, we are unable to subject this hypothesis to analytical testing. Nonetheless, we offer data that should be useful in designing studies with said objective.
To sum up, our study poses the following research questions:
Are hemodynamics and heart development affected by hypercoiling or other physical and structural changes in the UC?
How are UC deformities related to one another, and what repercussions do they have on cardiac morphology and physiology?
Can UC deformities, and not just overall birth defects, be linked specifically to mother’s age?
Which signaling pathway could explain the possible association between UC and congenital heart disease?
Summary points list
Umbilical cords alterations seem most frequent in newborns with congenital heart defects. Hypercoiled umbilical cords ranked as the most common alteration seen in congenital heart defects. This study reinforces the thesis that a link may exist between anatomical umbilical deformities and congenital heart defects.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Footnotes
Acknowledgments
The authors thank the Pontificia Universidad Javeriana—Hospital Universitario San Ignacio in Bogota, Colombia for its indispensable support and participation in this study. The authors also thank the Staffs of the Departments of Pathology and Obstetrics and Gynecology. The authors also extend their thanks to the parents who participated in UC studies and to Steven W Bayless for the English translation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding statement
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study makes up part of the research project entitled, “Congenital heart diseases and umbilical cord abnormalities, an unknown association?” (ID PPTA 00008766) financed by the Pontificia Universidad Javeriana and its Hospital Universitario San Ignacio, Bogota, Colombia.