
Abstract
There are multiple manifestations in the neonatal period for infants born to mothers with systematic lupus erythematosus (SLE), ranging from cardiac, hematologic and dermatologic abnormalities. Cardiac complications may arise in utero in the form of heart block with a resulting increase in fetal mortality. The fetal conduction system is suspected to be affected by transplacental maternal antibodies, however additional environmental and fetal factors appear to play a role. We describe a rare case of a dichorionic-diamniotic twin pregnancy in which only one twin developed a complete heart block progressing to hydrops fetalis and fetal demise.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a multi-organ autoimmune inflammatory disease which follows a relapsing and remitting course [1]. With an inactive disease and lack of end-organ involvement, the risk of miscarriages, stillbirths or fetal growth restriction are not significantly increased as compared to the general population [2]. However, the presence of anti-Ro/La and antiphospholipid antibodies are associated with multiple fetal anomalies such as congenital heart block and neonatal cutaneous lupus syndrome [3].
The incidence of neonatal lupus erythematosus approximates to 2% in offspring of mothers with autoantibodies of Sjogren syndrome autoantigen type A (Ro/SSA) or B (La/SSB), with an 18% to 20% recurrence rate. Conversely, approximately 25% of the mothers of neonates with neonatal lupus are asymptomatic at the time of delivery, of which 50% will become symptomatic within three years [4].
Neonatal lupus erythematosus commonly presents with reversible manifestations including cutaneous lesions (40%) hepatic dysfunction (35%), and hematological abnormalities (35%) [4]. Approximately 25% of neonates present with irreversible cardiac arrhythmias; the most distinctive and dangerous feature. Neonatal heart block occurs in 1–5% of fetuses of women with the anti-Ro/La antibody and has a recurrence rate of 16% in subsequent pregnancies. The transplacental transfer of maternal autoantibodies is believed to destroy the fetal Purkinje system, thereby causing fixed fetal ventricular bradycardia that may result in hydrops fetalis due to heart failure [4].
We describe a rare case of a dichorionic-diamniotic pregnancy with twin males in which only one twin developed complete heart block progressing to hydrops leading to intrauterine fetal demise.
Case presentation
A 27-year-old G2, P1, A2, L1 female with known SLE for the last 12 years was referred to our fetal cardiology clinic for evaluation at 25 weeks of gestation. She had a dichorionic, diamniotic twin pregnancy with concerns for fetal bradycardia in twin A. She was positive for SSA (Ro) and SSB (La) autoantibodies and her symptoms (joint pains and skin rash) were well controlled with dexamethasone, chloroquine, aspirin, and enoxaparin.
Initial fetal echocardiogram for twin A showed a normal cardiac anatomy with a mildly hypertrophied and dilated ventricles. M-mode echocardiogram showed a complete AV block with an atrial rate of 150 bpm and a ventricular rate of 43 bpm. Interestingly, Twin B had a normal fetal cardiac anatomy and function and a heart rate of 147 bpm with a complete AV synchrony.
A follow up fetal echocardiogram at 28 week-gestation confirmed the presence of a complete AV dissociation with an atrial rate of 155 bpm and ventricular rate of 40 bpm in twin A (Fig. 1). There was also biventricular hypertrophy and dilation (Fig. 2), with an increased cardiothoracic ratio of 0.71, and a decreased ventricular function. A small pericardial effusion was also noted at that visit (Fig. 1).
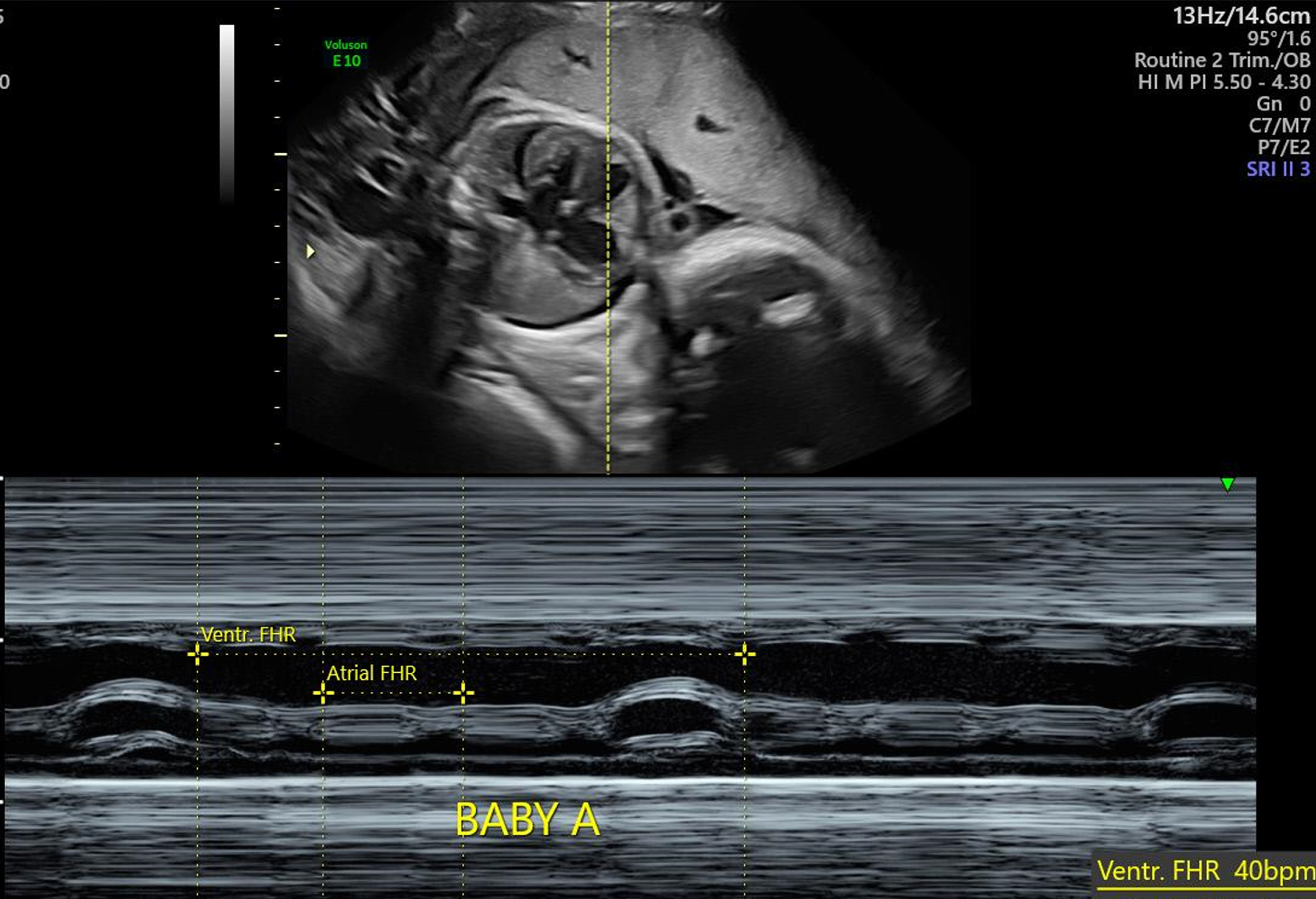
A fetal 2-D echo and M-mode in twin A at 28 week-gestation showing an atrial rate of 155 and a ventricular rate 40 beat/min with a complete AV dissociation. A small pericardial effusion is also noted.
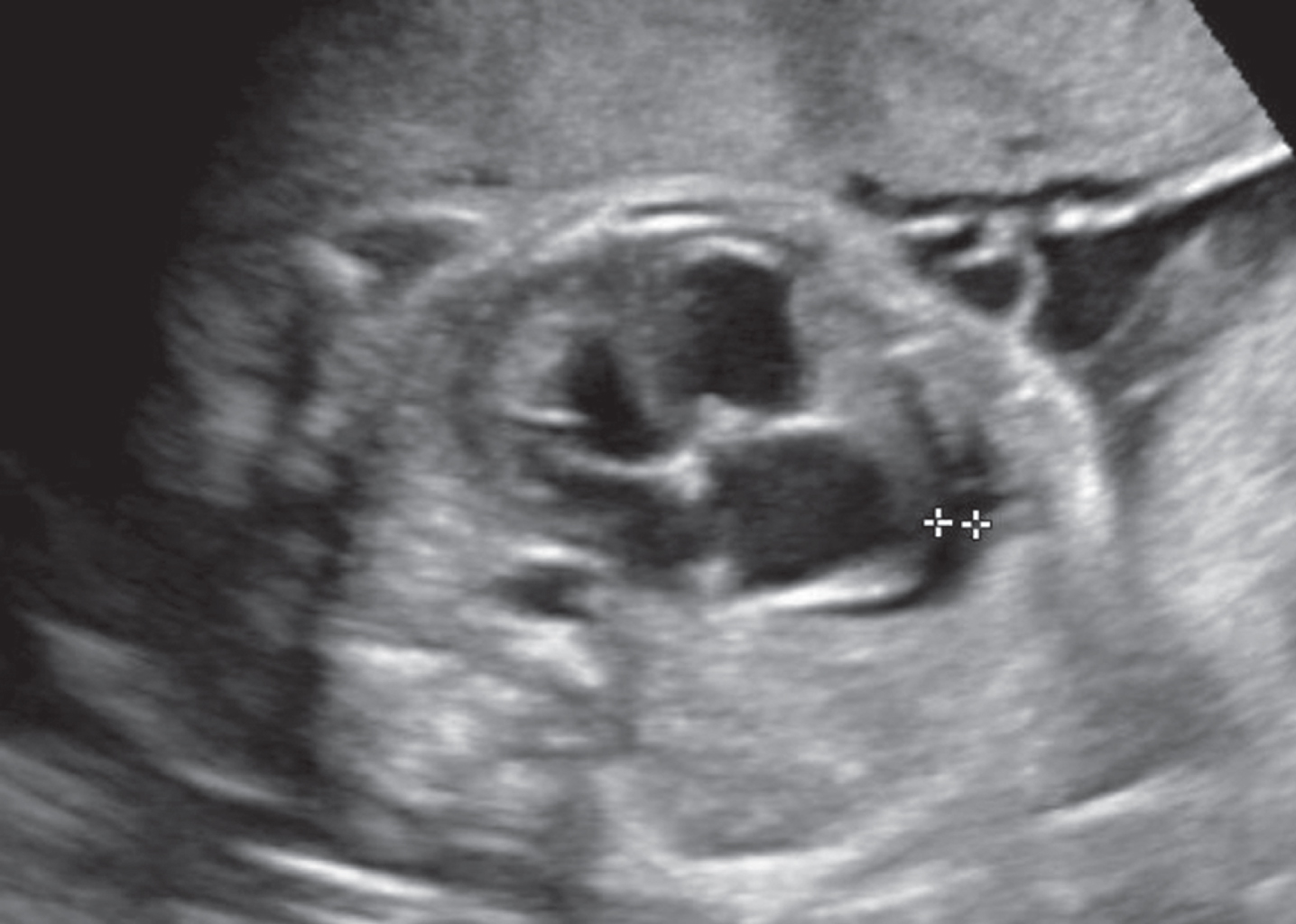
A fetal 2-D echo done at 28 week-gestation in twin A showing a 5 mm pericardial effusion, a biventricular hypertrophy and dilation.
At 30 week-gestation, progression to hydrops fetalis was demonstrated with the development of an increased nuchal skin thickness (10 mm), significant scalp edema (Fig. 3), ascites and peri-hepatic fluid collection (Fig. 4). The ventricular function continued to deteriorate.
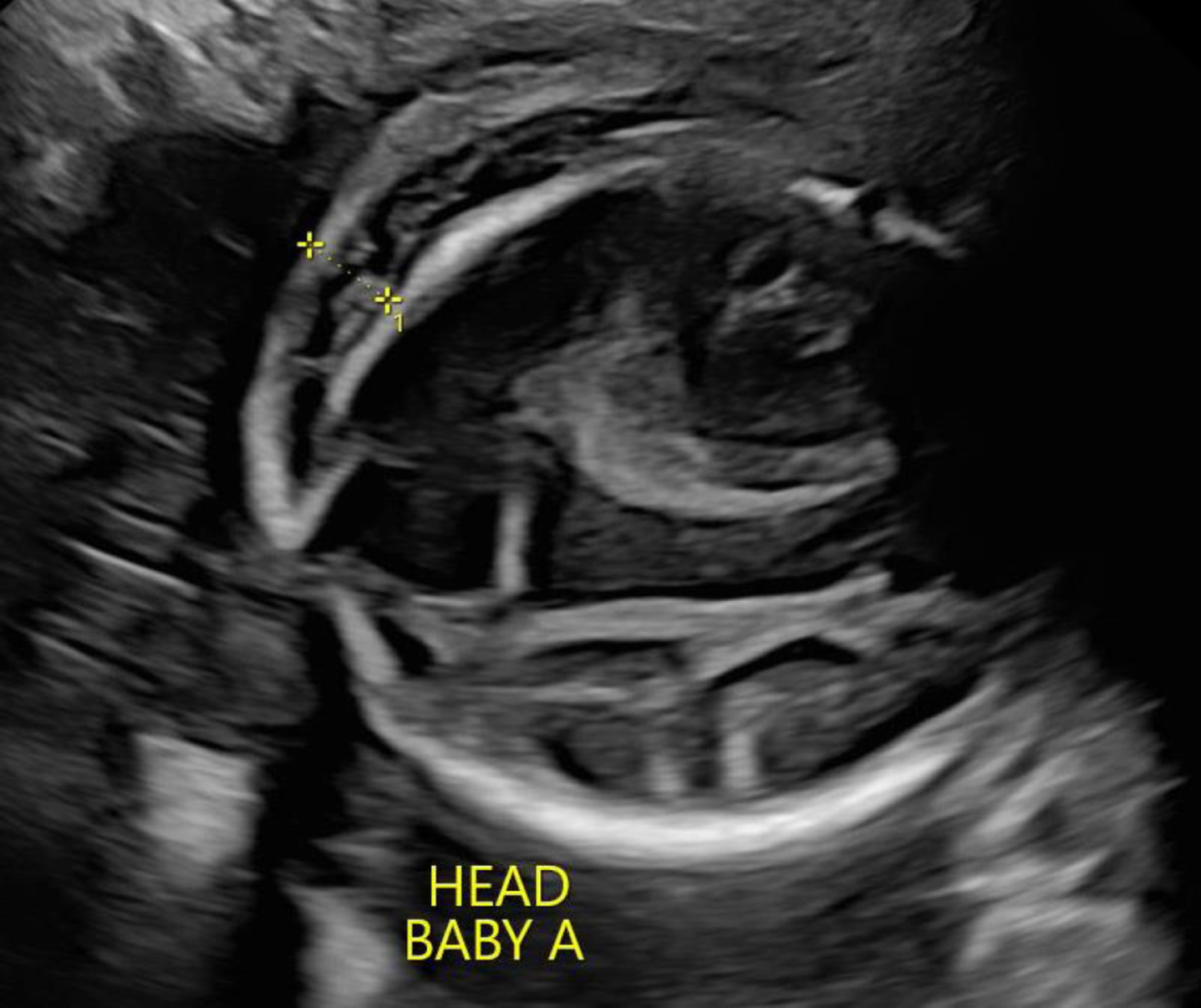
A fetal ultrasound scan of twin A head at 30 week-gestation showing a significant scalp edema.

An abdominal fetal ultrasound scan of twin A showing a peri-hepatic fluid collection.
The mother went into preterm labor at 31-weeks of gestation, triggered by intrauterine fetal demise in twin A and fetal decelerations in Twin B. Initial venous cord gas was 7.23/48/29/20/-7.6. Twin B had significant hypotension and respiratory depression at birth requiring intubation and mechanical ventilation. He received surfactant due to respiratory distress syndrome and was successfully extubated on day 2 of life. Interestingly, twin B had a normal echocardiogram and EKG with no evidence of heart block. He was later discharged at 35 week-gestation on no medications and is being followed in our premie clinic. An autopsy for twin A was declined by the family.
Serial fetal echocardiography screening is advised in women who test positive for autoantibodies to Sjogren syndrome auto-antigens types A or B or with a previous history of an infant with neonatal lupus erythematosus [4]. Most cases are detected early in the second trimester and only two percent of cases are detected postnatally [5]. The cardiac rhythm abnormalities of infants born to mothers with SLE has been thought to arise from the transplacental transfer of maternal autoantibodies SSA/Ro and SSB/La which causes destruction of the fetal cardiac conduction system. Both AV node fibrosis and calcium imbalances due to cross reaction between the antibodies and calcium channels have been suggested as potential causes for this destruction [5]. Risk factors for fetal mortality include the presence of major structural cardiac defects, hydrops, an atrial rate < 120 bpm, and ventricular rate < 55 bpm [6, 7].
There are limited treatment options for AV block in utero and early delivery is indicated with evidence of fetal distress. There are reports of steroids and intravenous immunoglobulin being beneficial in these cases, however data remains mixed. Studies that involved the use of hydroxychloroquine 400 mg daily starting between the 6 and 10 weeks of gestation have shown a decreased risk of developing neonatal cardiac lupus, especially in women with a previous history of an affected infant. Postnatal management involves the use of cardiac pacing; however, the insertion of a pacemaker is limited by the infant weight and gestational age. The concurrent development of hydrops significantly raises the mortality.
Fetal AV heart block is often seen if the mother has higher auto-antibodies titers, however enough overlap exists between affected and unaffected cases that a high titer alone is not indicative of heart involvement. There are some reports of discordant expression of cardiac SLE in neonates in dizygotic twin pregnancies suggesting the possibility of different interaction between fetal and in utero environmental factors [7–11].
Our case is unique since Twin A’s demise along with the resultant heart rate decelerations in Twin B caused the mother to go into preterm labor which ultimately resulted in delivery. Moreover, there was discordant expression as only one twin was affected by heart block. This in turn raises the possibility of specific fetal factors potentially modulating the effect of maternal antibodies on the fetal conduction system. Additional research is needed to further elucidate the nature of the complex interaction between the fetus and maternal autoimmune diseases.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflict of interest.
Consent
Consent was obtained from parents prior to submission of this manuscript.