
Abstract
BACKGROUND:
Late-onset sepsis is common in extremely low birth weight (ELBW) infants, and it leads to the use of antibiotics to cover resistant organisms, which can be nephrotoxic. Here we have investigated the role of vancomycin plus piperacillin-tazobactam on the rate of acute kidney injury (AKI).
METHODS:
In a retrospective case-control study, medical records of all ELBW infants who were admitted to our Neonatal Intensive Care Unit (NICU) with late onset sepsis who were prescribed vancomycin plus piperacillin-tazobactam were reviewed for demographics, clinical characteristics, use of potential nephrotoxic medications and outcomes.
RESULTS:
During the study period, 264 patients were admitted, of whom 28.4%(75/264) received vancomycin plus piperacillin-tazobactam and were matched with 64 controls. There were no differences in gestational age or birth weight between cases and controls [688±160 vs. 689±162 grams (p = 0.99), and 24.7±1.8 vs. 24.7±1.6 weeks (p = 0.99) respectively]. There was no difference in the rate of sepsis between cases and controls [76%(55/72) vs. 64%(41/64) respectively, p = 0.11]. Infants exposed to vancomycin plus piperacillin-tazobactam had a higher percentage of concomitant use of vasopressors and amphotericin. To adjust for confounders, a logistic regression analysis was conducted with AKI as the dependent variable. Use of vasopressors and vancomycin plus piperacillin-tazobactam were the only risk factors associated with AKI with an adjusted OR (95%CI) of 4.08 (1.90–8.74), p < 0.001; and 2.87 (1.26–6.53), p = 0.01 respectively.
CONCLUSION:
The use of vancomycin plus piperacillin-tazobactam in ELBW infants is associated with an increased risk for AKI.
Introduction
The recent improvement in survival among extr-emely preterm infants has been associated with increased short and long-term morbidities [1, 2]. It is common for sick infants to receive multiple broad-spectrum antimicrobials while their sepsis workup is pending. Some of these antimicrobials are known to be nephrotoxic, but others have an unclear renal side effects profile.
Acute kidney injury (AKI) is a common compli-cation in infants in neonatal intensive care units (NICUs), accounting for up to 30%of neonates in tertiary NICUs. The rate may be even higher ∼47%among extremely low birth weight infants (ELBW) [3, 4]. The incidence of AKI is probably underestimated due to the lack of standard definition and screening guidelines in high-risk infants. AKI is associated with higher morbidity, mortality, and longer NICU stay [4–7]. The high rates of AKI in ELBW infants can be partially attributed to incomplete nephrogenesis, low glomerular filtration rate (GFR), and increased renal vascular resistance. These risk factors put ELBW infants at risk for hypoperfusion injury and tubular ischemia. About 50%of AKI episodes in preterm infants are secondary to drug exposure [8]. Many commonly used medications in the NICU are not well studied in terms of their nephrotoxicity, especially in ELBW infants. The lack of knowledge about the side effects of these medications may increase morbidity and mortality in these infants. Vancomycin is a known nephrotoxic medication, but there is growing evidence of a further increase in nephrotoxicity in children or adults who received the combination regimen of vancomycin and piperacillin-tazobactam compared to vancomycin alone or vancomycin with any other beta-lactam [9, 10].
This antibiotic regimen is commonly used to treat intra-abdominal infections such as NEC or intraperitoneal abscesses or in patients with an indwelling central venous catheter. Vancomycin has a great gram-positive coverage against resistant organisms such as methicillin-resistant staphylococcus aureus (MRSA). Piperacillin/tazobactam provides broad coverage for gram-negative bacteria including pseudomonas, and anaerobic bacteria. In this study, we sought to determine if this antibiotic combination causes AKI in ELBW infants.
Methods
In a retrospective case-control study, medical records of all infants who were admitted to our NICU were reviewed. Our inclusion criteria consisted of all infants who were extremely low birth weight (< 1000 grams) and who were admitted to the neonatal intensive care unit (NICU) between March 2010 and August 2017. Our exclusion criteria consisted of all infants who had lethal congenital anomalies, renal anomalies and who died within the first week of life. Cases were defined as infants who were treated with vancomycin plus piperacillin-tazobactam for presumed late-onset sepsis for at least 48 hours. For each AKI episode, every case subject was matched to a control subject who was born before or after the case subject and who was not exposed to vancomycin plus piperacillin-tazobactam. Also, control patients were matched to cases for birth weight (within 10%difference) and gestational age (within one-week difference). Episodes of AKI were matched. Each episode of exposure to vancomycin plus piperacillin-tazobactam was matched to a control. Of note, the same patients could have received multiple courses of the antibiotics and the same control patients could have served multiple times as a control (separated by time). A patient who served as a case remained a case during the study, and a patient who served as a control remained a control throughout the study. None of the patients who were cases served as controls for another course of antibiotics, and none of the controls served as cases in subsequent courses of antibiotics exposures.
For patients with multiple AKI episodes, baseline creatinine was defined based on the latest serum Cr and up to one week before the initiation of antibiotics. Post-treatment creatinine was the first creatinine level obtained and within one week after the discontinuation of antibiotics.
Medical records were reviewed for patients’ demographics, including birth weight (BW), gestational age (GA), gender, ethnicity, mode of delivery, and Apgar scores at 1 and 5 minutes of life.
Medical records were also reviewed for infants’ clinical characteristics and outcome, including small for gestational age (SGA), patent ductus arteriosus (PDA), chorioamnionitis, sepsis, mechanical ventilation, postnatal steroids, necrotizing enterocolitis (NEC), severity of bronchopulmonary dysplasia (BPD) according to the NICHD network definition, grades of intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), length of stay, and death.
Medical records were reviewed for concomitant use of other medications during the course of vancomycin plus piperacillin-tazobactam use like gentamicin, furosemide, vasopressors (dopamine, epinephrine), amphotericin, acyclovir, and indomethacin. At the time of treatment with van-comycin plus piperacillin-tazobactam, medical rec-ords were reviewed for daily serum creatinine for a week before and a week after the antibiotics. Also, the medical records of infants who served as controls were reviewed for serum creatinine values during the period that corresponded to the period when the matched cases were treated with vancomycin plus piperacillin-tazobactam. For example, if a case subject was treated on day of life 20, the serum creatinine values of the matched control were reviewed for a week before and a week after day of life 20.
Acute kidney injury (AKI) was documented based on the changes in serum creatinine only, according to the KDIGO definition since urine output data was not available on chart review [11]. The study was approved by the Institutional Review Board (IRB) at MetroHealth Medical Center, Cleveland, OH.
Statistical analysis
Data were expressed as mean±standard deviation and as percentages. Parametric and non-parametric data were analyzed by T-test and Mann Whitney U test, respectively. Categorical data were analyzed by Chi-square test and Fisher exact test appropriately. A correlation between days of antibiotics use and percent rise in serum creatinine was calculated (Pearson R coefficient). To adjust for potential confounders, a backward logistic regression analysis was conducted with AKI as the dependent variable and concomitant medications used during vancomycin plus piperacillin-tazobactam course (that showed a statistically significant difference in a binary analysis) as the independent variables. A p-value < 0.05 was considered statistically significant.
Results
During the study period, 264 ELBW infants were admitted to the NICU. Among all patients, 28.4%(75/264) received vancomycin and piperacillin-taz-obactam, thus served as cases. Another matched 64 patients who had serum creatinine available for review served as controls. The demographics of inf-ants who received vancomycin and piperacillin-tazo-bactam and their controls are summarized (Table 1). There were no significant differences between the two groups.
Patients’ demographics
Patients’ demographics
The clinical characteristics and the outcome of infants exposed to vancomycin and piperacillin-tazo-bactam and their controls are summarized (Table 2). There was a higher rate of NEC and BPD in the group of infants who received the combined antibiotics therapy. During the study period, 75 infants received vancomycin with piperacillin-tazobactam. However, only 69 cases had serum creatinine levels available for review after the first course of antibiotics, 29 infants received 2 courses, 15 infants received 3 courses, and 8 infants received 4 courses of vancomycin and piperacillin-tazobactam. Overall, among the 139 studied patients, 120 courses of vancomycin and piperacillin-tazobactam were available for review, and they were matched to 64 controls (74 matched antibiotic courses).
Clinical characteristics and patients’ outcome
Among all patients who received vancomycin and piperacillin-tazobactam 27%(19/69), 38%(11/29), 40%(6/15), and 14%(1/7) developed AKI after the first, second, third, and fourth course of antibiotics, respectively. The average course of vancomycin plus piperacillin-tazobactam therapy was 5.2±3.5 days. There was no correlation between the duration of an antibiotics course and the percent increase in serum creatinine (Pearson R = –0.042; p = 0.655). Medications used during the times when infants were exposed to vancomycin plus piperacillin-tazobactam and their controls are summarized (Table 3). There were significant differences between the two groups. Infants exposed to the combination of antibiotics had a simultaneous higher rate of exposure to vasopressors and amphotericin.
Concomitant drug exposure
Infants treated with vancomycin plus piperacillin-tazobactam had a higher rate of AKI episodes than their controls [31%(37/120) vs. 12%(9/74); p = 0.003). Figure 1]. The percent increase in serum creatinine and AKI stages in infants exposed to dif-ferent courses of vancomycin and piperacillin-tazo-bactam and their controls are summarized (Table 4). There was a significant increase in the percentage of serum creatinine in infants exposed to vancomycin plus piperacillin and tazobactam and an increase in the rate of AKI at all three different stages.
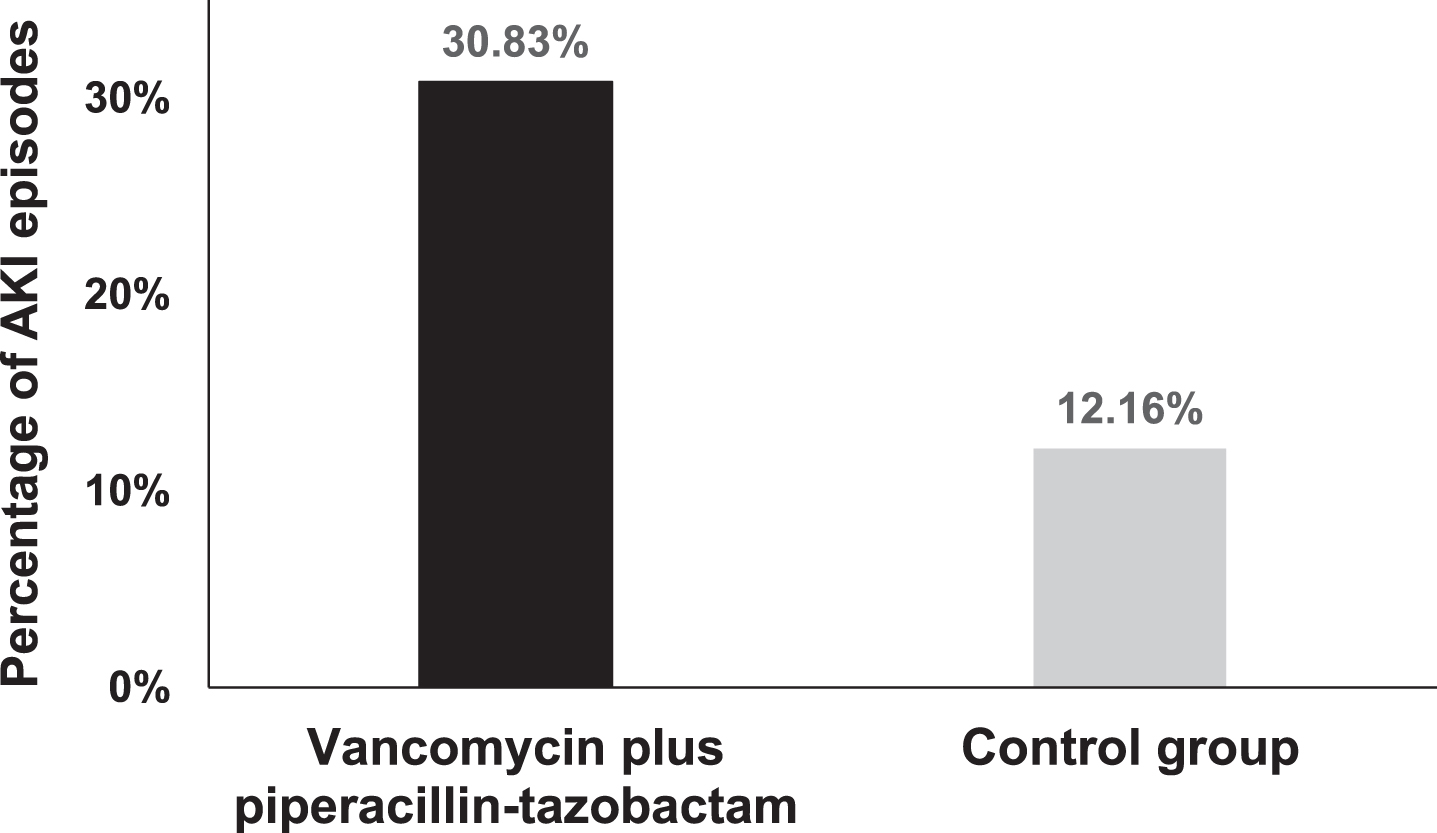
Percentage of AKI episodes among ELBW infants who received Vancomycin plus piperacillin-tazobactam and their controls.
Percent increase in serum creatinine and AKI stages
To adjust for potential confounders, since infants with AKI had a higher rate of exposure to vasopres-sors and amphotericin, a backward linear regression analysis was conducted with AKI as the dependent variable, and vancomycin plus piperacillin-tazo-bactam, vasopressors and amphotericin as independent variables. Vasopressors and vancomycin plus piperacillin-tazobactam remained the only risk factors associated with AKI (Table 5).
Adjusted odd’s ratio of risk factors associated with AKI
To the best of our knowledge, this study is the first to evaluate the renal side effect of the vancom-ycin plus piperacillin-tazobactam regimen in ELBW infants. The results reveal vancomycin plus pipe-racillin-tazobactam use in ELBW infants is associated with higher rates of AKI. This result is in line with other studies in adults and pediatric populations [12–14]. In a retrospective study that included 228 patients matched cohort reported 2.5 folds greater AKI incidence in children who received vancomycin and piperacillin-tazobactam compared to vancomycin and cefepime [9]. In a cohort study that included 167 children, the authors identified some risk factors of AKI related to vancomycin toxicity. These risk factors were prolonged vancomycin use > 15 days, age < 1 year, sepsis, and concomitant administration of piperacillin-tazobactam [15]. In a large (1,915 patients) multicenter retrospective study in children between 6 months and 18 years of age: IV vancomycin plus piperacillin-tazobactam recipients had a higher odds of AKI on each hospital day compared to vancomycin plus another beta-lactam OR 3.4 (CI 2.26–5.14) [13]. Hammond et al. reviewed 14 studies in a meta-analysis evaluating AKI risk in adults with concomitant vancomycin and piperacillin-tazobactam. They reported a higher risk of AKI in those who received this combination compared to vancomycin and any other β lactam (OR: 3.15, CI: 1.72–5.76) [16]. Another meta-analysis that included 3,258 adults also reported an increased risk of AKI in patients who received vancomycin plus piperacillin-tazobactam vs. those who received vancomycin +/- β lactam [17]. A large trial of adult ICU patients investigated the recovery time after AKI. The subjects who received piperacillin-tazobactam had a longer renal recovery time compared to those who received meropenem. Furthermore, the discontinuation of piperacillin-tazobactam led to a shorter recovery time [18]. W. Rutter et al. reported in a retrospective study that included more than 10,000 patients a two-fold increase in the odds of nephrotoxicity in patients who received vancomycin plus piperacillin-tazobactam compared to either agent as a monotherapy [19]. A similar finding was reported in a prospective multicenter observational study in adults 18 years and older (n = 242 patients). Patients who received this antibiotic combination were 6.7 times more likely to develop AKI compared to others in the cohort [20]. The use of vancomycin plus piperacillin-tazobactam is associated with a higher risk of nephrotoxicity compared to vancomycin/cefepime [21]. Similar findings have been found in comparing vancomycin plus piperacillin-tazobactam to vancomycin alone or vancomycin/imipenem-cilastatin in pediatric and adult burn patients [22]. The difference in AKI rate between the group who received vancomycin and piperacillin-tazobactam compared to the group who received vancomycin and another antibiotic maybe is secondary to additive renal toxicity from the sec-ond antibiotic or by enhancing vancomycin renal toxicity. Also, the increase in nephrotoxicity is pro-bably not related to piperacillin-tazobactam alone since its nephrotoxicity is not greater than other beta-lactam inhibitors such as ampicillin-sulbactam [23]. The mechanism of increased toxicity is un-known. Vancomycin causes oxidative injury that may exacerbate interstitial nephritis caused by pipera-cillin-tazobactam [14]. Another possible mechanism is piperacillin-tazobactam interferes with vancomycin excretion from the nephrons, which may lead to direct injury within the nephrons caused by vancomycin accumulation [24, 25].
The present study showed infants who received vancomycin plus piperacillin-tazobactam were more likely to be exposed to gentamycin, vasopressors, and amphotericin. The effect of vasopressors on the kidneys varies based on the type and dose of infusion. Gentamycin may cause proximal tubular cell necrosis. The degree of tubular injury correlates well with the decline in renal function [26]. The effect of vancomycin plus piperacillin-tazobactam on the rate of AKI in the study was adjusted for significant confounders.
There are several studies aimed to investigate the causes of AKI in preterm infants. Cataldi et al. identified some risk factors associated with AKI in premature infants such as low Apgar scores and exposure to certain antibiotics such as ampicillin and ceftazidime [27]. In a retrospective case-control study of 472 ELBW infants, the use of cephalosporins is associated with higher rates of AKI [28]. Other potential risk factors for AKI besides prematurity and low birth weight are perinatal asphyxia, intubation at birth, patent ductus arteriosus (PDA), preterm premature rupture of membranes (PPROM), sepsis, disseminated intravascular coagulation (DIC), and bronchopulmonary dysplasia (BPD) [29]. More than 50%of preterm infants with gestational age 22 to 25 weeks presented with transient alteration in renal function [29]. Koralkar et al. also reported an increased risk of AKI in very low birth weight (VLBW) infants who needed inotrope support [30]. Our study showed similar findings in ELBW infants who received inotropes with an OR 4.08 (p < 0.001).
Antibiotic stewardship could reduce AKI rates if this broad-spectrum combination is modified or discontinued at 48 to 72 hours after initiation [10]. The weaknesses of our study are its retrospective design and the inability to include patients with AKI based on urine output definition due to the unavailability of urine output data. Another weakness is that we did not have a case - control group of patients with culture proven sepsis treated with vancomycin / piperacillin-tazobactam versus other antimicrobial agents to avoid sepsis as a confounding factor.
Our results also showed that case subjects had a higher rate of severe bronchopulmonary dysplasia (BPD) than control subjects. That probably is attributed to altered renal function resulted in fluid retention and pulmonary edema early in life. In contrast, caffeine citrate reduces the frequency of AKI and the rate of BPD at 36 weeks corrected gestational age [31, 32]. The mechanism is unknown, but it can be related to the diuretic effect of caffeine in promoting negative fluid balance. Early induced diuresis lowers peak fluid balance and improves pulmonary edema. A higher degree of BPD was reported in infants with a history of early high fluid intake or positive fluid balance [33]. Selewski et al. reported that children with early AKI were on longer days of mechanical ventilation [34]. However, positive fluid balance or peak fluid balance at one-week chronological age is also a predictor of the need for mechanical ventilation at that age [35].
Conclusion
The use of vancomycin and piperacillin-tazo-bactam in ELBW infants increases the rate of AKI. The results of our study are in line with similar studies in older children and adult patients. This antibiotic combination should be used with extreme caution in ELBW infants and side effects of this therapy should be discussed with parents before initiation of therapy with the potential for long-term effects on outcomes. Further knowledge in neonatal pharmacology of such antibiotic combination is crucial to better identify nephrotoxic medications; thus, larger prospective studies are warranted.
Funding and conflict of interests
None.