
Abstract
BACKGROUND:
Preterm infant experiences neuromotor disturbances and neonatal pain during NICU stay. Optimal brain development and pain tolerance require both sensory and motor experiences. We aimed to explore the effect of multimodal stimulation (MMS) including multi-sensory and movement therapy on neuromotor behaviour and neonatal pain among hospitalized preterm infants.
METHODS:
32 recruited preterm infants [gestational age (GA): 28 to 36 weeks] by convenience sampling technique for pre-test-post-test control group, single-center randomized controlled study were randomly allocated into two groups, MMS group, and control group. MMS group received the interventions for 5 days period, totalling five sessions with 30 minutes/session. Infant Neurological International Battery (INFANIB), Neonatal Infant Pain Scale (NIPS), weight, length, and Occipitofrontal circumference (OFC) were recorded at baseline and 6th day to analyze the changes observed neuromotor behaviour, neonatal pain, and changes in the anthropometric parameters respectively.
RESULTS:
GA, weight, length and OFC of preterm infants recruited were, 34.4±2 weeks, 2.11±0.48 kg, 45±3.8 cm and 32.3±1.7 cm respectively. INFANIB and NIPS change scores in MMS group were [4 (2, 6); p = 0.001] and NIPS scores [2 (2,3); p < 0.001] respectively when compared to INFANIB [– 4 (– 6, – 2); p = 0.001] and NIPS scores [1 (– 1,1); p = 0.778] in control group. Significant difference p < 0.001 in INFANIB and NIPS scores while non-significant difference in weight (p = 0.166), length (p = 0.443) and OFC (p = 0.413) were observed between the groups.
CONCLUSION:
Administration of MMS has a positive clinically significant impact on neuromotor behaviour and neonatal pain on preterm infants.
Abbreviations
Birth Weight
Corrected Gestational Age
Council For International Organizations Of Medical Sciences
Infant Neurological International Battery
Indian Council for Medical Research
Multimodal Stimulation
Neonatal Infant Pain Scale
Occipitofrontal Circumference
World Health Organization
Introduction
Approximately 10%of all births were classified as preterm birth [1]. About 50%of them are at a higher risk for the development of behavioural, motor, and cognitive problems due to unavoidable neonatal intensive care unit (NICU) stay [2]. These preterm infants have higher chances of developing, limited social or emotional development, autism spectrum disorders, cerebral palsy, attention-deficit/hyperactive disorder, developmental coordination disorder, language impairments, hampered executive functions, decreased attention span, blindness, deafness, etc. [3]. They affect more than one domain of infant development and affects the overall quality of life of infant during their later childhood days by restricting their participation in home, school, and community activities [3]. In addition to NICU stay, preterm infants are exposed to 7 to 17 painful stimulation per day for their immunization, metabolic screening, and blood sampling [4]. Exposure to the painful stimulus by preterm infants during their NICU stay has a detrimental impact on cortical development [5], behaviour [6], and abnormal cortisol response at later stages [7].
In NICU, preterm infants are deprived of necessary sensory stimulation for optimal growth and neuromotor behaviour against the uterine environment in which the foetus receives those necessary intrauterine sensations through their maternal environment [8, 9]. A handful of researches are executed to simulate the intrauterine maternal sensation of amniotic fluid and uterine wall provided through multisensory stimulation which includes, auditory, tactile, visual, and vestibular (ATVV) stimulations to improve neuromotor behaviour [10], weight gain [11], heart rate variability [12], neonatal pain [13], and oxygen saturation [14]. But to the best of our knowledge, none of the studies have used combined multi-sensory stimulation and kinesthesia (kinesthetic sense/sense of movement provided through therapy) as a part of early interventions. As recommended both sensory and motor experiences are necessary for normal brain development [10, 15].
However, the effects of early multimodal stimulation (MMS) with multi-sensory and movement therapy on neuromotor behaviour and neonatal pain among hospitalized preterm infants have not yet been explored. Hence, the research question for the priority of investigation is whether MMS would produce significant changes in neuromotor and pain among hospitalized preterm infants. We hypothesize that there would be no significant changes in neuromotor and pain outcomes between the groups following MMS intervention as the null hypothesis. While significant changes in neuromotor and pain outcomes between the groups following MMS intervention as an alternate hypothesis. Thus, the study aimed to determine the effect of MMS on hospitalized preterm infants on neuromotor behaviour and neonatal pain perception levels.
Materials and methods
Ethical statement and protocol registration
The study protocol for the single-center, pre-test post-test control group, randomized controlled study was approved by the institutional ethics committee (MMDU/IEC/1566) on 10th December 2019 and the same was registered in the Clinicaltrials.gov, with unique registration no. NCT04247308 on 30th January 2020 (last updated on 21st July 2021). https://clinicaltrials.gov/ct2/show/NCT04247308 before the first sample recruitment. Before their reg-istration, a unique Universal Trial Number (UTN), U1111-1236-9478 was obtained from WHO’s ICTRP and followed with the registration. The feasibility randomized controlled trial followed the ethical guidelines recommended by, Helsinki Declaration (Revised 2013), Council For International Organizations Of Medical Sciences (CIOMS) guideline’s International ethical guidelines for health-related research involving humans (2016), and National Ethical Guidelines for Biomedical Research Involving Children (2017) prescribed by the Indian Council for Medical Research (ICMR). Before recruiting the preterm infants in this trial, a signed informed consent form (ICF) prepared from the templates for ICF by WHO was obtained from the parents of the recruited preterm infants. Data collection for the study was conducted between October 2020 and August 2021.
Sample size estimation
The sample size for the study was calculated using the formula for comparing means with the level of significance as 0.05 (Zα= 1.96), with 80 %power (Zβ= 0.84) and 3.5 units change (d = 3.5) in the primary outcome measure, Infant Neurological International Battery (INFANIB), score as a clinically meaningful difference (CMD) with pooled standard deviations of, S = 3.2, from previous research [10]. In the study by, Kanagasabai et al. [10], the CMD of INFANIB was found to be, 3.08 against the proposed CMD of 2 by them. Hence, we have fixed the target to achieve a CMD of 3.5 between the groups. Thus, making the required sample of 13.11 in each group. Considering a 20%drop-out rate (n = 2.62), a final minimal required sample size of n = 16 (by the calculation, obtained minimal required sample size was, n = 15.73. As the sample size cannot be considered in decimals, the value was rounded off to the next whole number) was estimated for each group of the study. So, the total sample size for the study considering two groups was estimated to be, n = 32.
Recruitment
All the required preterm infants (n = 32) for the study were recruited from neonatal intensive care units of recognized tertiary care teaching hospital attached to the medical college through the conve-nience sampling technique to participate in this pre-test-post-test control group, single-center randomized controlled study. The selection criteria adopted for the inclusion of preterm infants were as follows, preterm infants born between 28 and 36 weeks of gestation, birth weight ranging from 1000–3500 g, and medically stable preterm infants. Preterm infants on assisted ventilation as they hinder the administration of neuromotor outcome measure, INFANIB, with congenital anomalies, congenital infections, and central nervous system injury, undergoing corrective surgeries, with severe cardio-respiratory anomaly, with other congenital anomalies (such as microcephaly) were excluded from their participation in the study.
Randomization
Recruited preterm infants were randomly allotted into two groups, MMS group and control group using block randomization with the matrix design of 4×8; which means 8 rows and 4 blocks containing 4 chits (2 chits for each group), totalling 32 chits. By the block randomization method, preterm infants was randomly allocated into one of the above two groups using Sequentially Numbered, Opaque Sealed, Envelopes (SNOSE) picked by the parents of eligible preterm infants. The physiotherapist who was not involved in this research performed the randomization. Once the first row of all the blocks was allotted, the next row blocks were opened for recruitment. Thus, approximately an equal number of preterm infants were assigned to each group over time.
MMS group
MMS group received multi-sensory stimulation and movement therapy for five days period, totalling five sessions. Each session will last for 30 minutes duration and received regular lifesaving NICU care. While the control group received regular lifesaving NICU care only. The study flow chart describing the details of the study is displayed in Fig. 1.
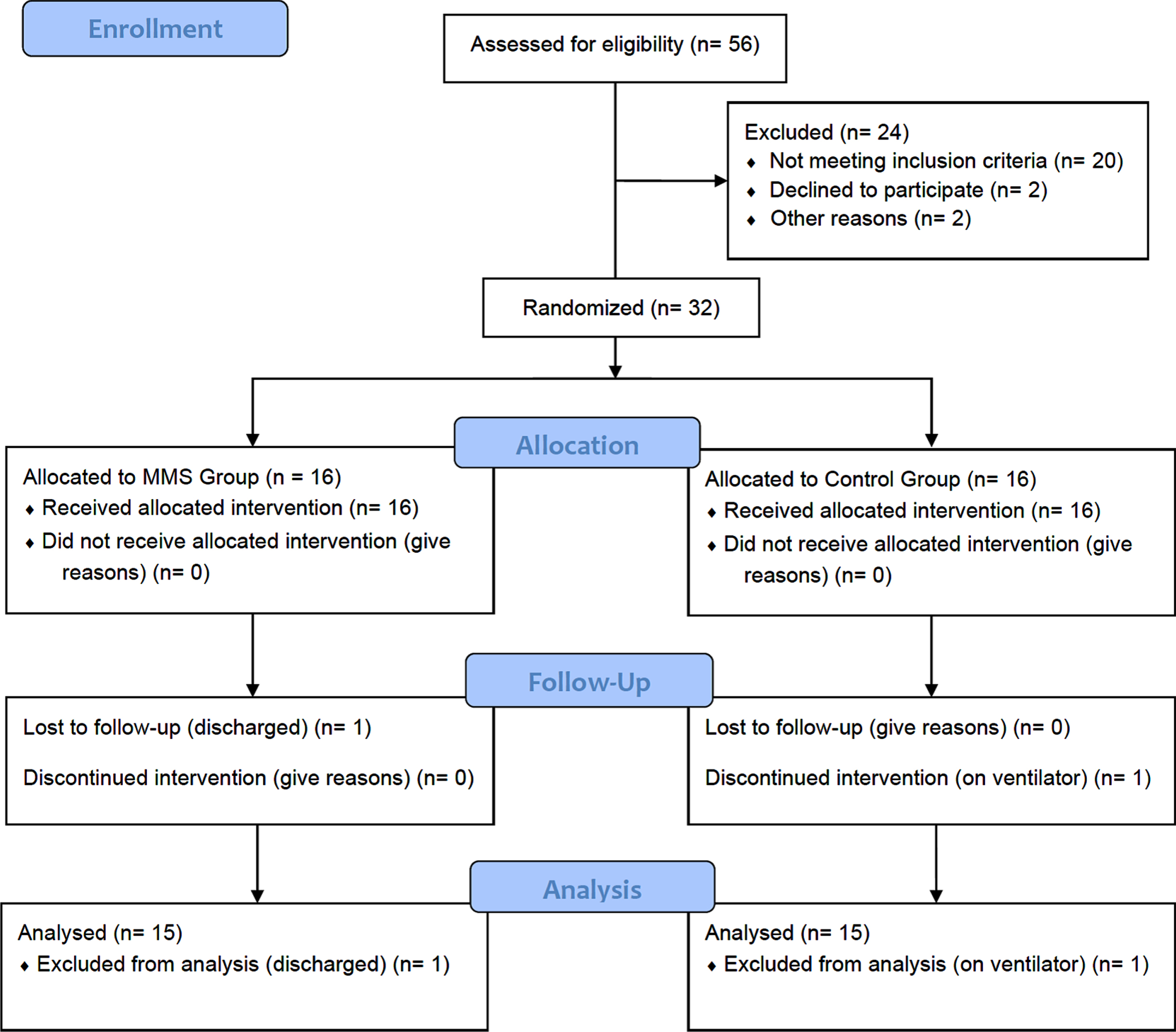
CONSORT (Consolidated Standards of Reporting Trials) flowchart of the study.
Multi-sensory stimulations consisted of auditory stimulation with voice provided by the mother (not provided with a soft lullaby using the miniature speaker as planned in the protocol but provided direct auditory stimulation in form of unstructured voice provided by the mother of preterm infants during every 2-hour regular feeding), gentle stroking massage (tactile), visual stimulations with black and white card gentle rocking, and oral stimulation including stocking cheeks, lips, jaw, and tongue, rubbing gum [16]. Each stimulation was administered for 3 minutes [10].
Movement therapy
Guided range of motion (upper and lower limb), antigravity movements in prone (neck and spinal extension), antigravity movements in sitting (supported), and upright positioning for 3 min each. The physiological stress (PS) during the intervention will be observed on a multi-parameter monitor. PS characterized such as heart rate (HR) > 200 or < 100 bpm, respiratory rate (RR) > 20 over baseline, and oxygen saturation (SpO2) below 86 %for more than 15 s [17]. The behavioral stress sign includes startle, tremors, yawning, finger splay, tone changes, state changes, gaze aversion, cry, hiccups and tongue protrusion will be observed throughout the treatment session. The intervention was modified (particular stimulation paused for 15 s and resumed if parameters recovered) based on the infant’s physiological and behavioral stress responses to prevent overloading of the inputs. MMS for the recruited neonates is named as Preemies’ Neuro-motor facilitation (PNMF) Protocol, tabulated in Table 1. The Preemies’ Neuro-motor facilitation (PNMF) Protocol by the first author was copyrighted under the copyright office of the Government of India with unique registration no. L-89359/2020 dated 11th February 2020 (copyright filed with diary no., 19789/2019-CO/L dated 10th December 2019).
Preemies’ Neuro-motor facilitation (PNMF) Protocol
Preemies’ Neuro-motor facilitation (PNMF) Protocol
PNMF Protocol should be administered for 30 min, 5 times per week.

Administration of auditory stimulation by the preterm neonate’s mother.

Administration of tactile stimulation by the neonatal physiotherapist.

Administration of visual stimulation by the neonatal physiotherapist.

Administration of vestibular stimulation by the neonatal physiotherapist.

Administration of oromotor stimulation by the neonatal physiotherapist.

Administration of passive range of motion by the neonatal physiotherapist.

Administration of antigravity movements in prone position by the neonatal physiotherapist.

Maintaining upright position of preterm infant by the neonatal physiotherapist.
Preterm infants allocated to the control group received life-saving care from the medical team and daily maternal care, such as being held in the mother’s arms.
Though both the groups may not be comparable, the groups differ only on basis of what changes would have occurred between measurements. Hence, this design could be considered as the accepted scientific standard for establishing a cause-and-effect relationship in clinical research.
Study measures
Demographic and clinical information
The anthropometric parameters such as gestational age (GA), corrected gestational age (CGA), birth weight (kg), length (cm), and occipitofrontal circumference (OFC) (cm), APGAR score at 1st minute and 5th minute were recorded for each preterm infants included in the study.
Outcomes
Infant Neurological International Battery (INFANIB): INANIB which is easier to administer and saves time as it took around 8–10 minutes to administer [18, 19], was used as the primary outcome measure to assess the neuromotor development of the pre-term neonate using corrected gestational age [10]. INFANIB has excellent reliability of, ICC = 0.9 with 90%sensitivity and 83%specificity and acceptable predictive validity, in detecting developmental delay [20]. It could be successfully used among preterm infants to detect the short-term effect of multisensory interventions on the neuromotor development of preterm neonates [10]. INFANIB consists of a total of 20 items to be evaluated in five positions, supine, prone, sitting, standing, and suspended [18]. Among them, only 14 items were administered at birth. The fourteen items which were considered at birth were, in the supine position (10 items) - hands closed/open, scarf sign, heel to ear, popliteal angle, leg abduction, dorsiflexion of the foot, foot grasp, tonic labyrinthine, asymmetric tonic neck reflex and pull to sitting; in the prone position (2 items) –all fours and tonic labyrinthine; in sitting position (1 item) –sitting and standing position (1 item) –weight-bearing will be observed and scored. Thus, the only total score of 70 was considered instead of 100 [21]. The neurological cut-off score proposed by the developer, Patricia H. Ellison (1986) were as follows, abnormal: ≤48, transient: 49–65, and normal: ≥66 [19]. Following the interpretation of scores were used to describe the characteristic of preterm infants recruited. INFANIB scores were recorded for both the groups to consider for the data analysis.
Neonatal Infant Pain Scale (NIPS): The Neonatal Infant Pain Scale (NIPS) was developed by Lawrence and colleagues and published in 1993 to assess the neonatal (both preterm and term neonates) and infant pain from birth to seven years of age [22]. NIPS assess the pain perceived by the neonates based on the six behaviours, facial expression, cry, breathing patterns, arm movement, leg movement, and state of arousal. The total score of NIPS ranges from 0 to 7, with scores > 3 indicates pain and scores approaching 7 indicating higher pain. Cry behaviour has three response categories (0, 1, 2) while all other behaviours have only two responses (0, 1). Thus, summing up the total scores of 7 for the six behaviours. The vocabulary used in NIPS to describe the pain is simple which could be understood without any difficulty by the health care professionals working in NICU with the neonates. NIPS was recorded within 2-minute after any painful stimulations in both groups.
Other outcomes: Weight (kg), length (cm), and OFC (cm) of the recruited preterm infants were recorded for both groups.
The above outcome measures were recorded at baseline and the end of the 5th day of interventions and used in further analysis.
Data analysis
The collected demographic dimensions, such as gestational age (weeks), birth weight (kg), birth length (cm), OFC and APGAR score at 1-minute and 5-minute and the outcome measures, which includes INFANIB and NIPS, to what extent the data match the normal distribution was confirmed by, “goodness of fit” test, Shapiro-Wilk (SW) test as the sample size of the recruited neonate is less than 50 (n < 50). The descriptive statistics of the normally distributed data (gestational age, birth weight, birth length, OFC) were expressed in mean±standard deviation and paired t-test was adopted to find out the differences within the MMS group and control group for pre-post intervention changes. While independent t-test was used to compare the changes in mean values of the outcome measures between the MMS group and control group at baseline and the end of the 5th day intervention of neonate from the NICU. For the data which deviate from a normal distribution (APGAR, INFANIB, and NIPS), the descriptive statistics were reported in the median with interquartile range (IQR) and range. Wilcoxon Signed-Ranks test will be adopted to find out the differences between the MMS group and control group for pre-post intervention changes. While Mann-Whitney U test was used to compare the changes in mean values of the outcome measures between the MMS group and control group at baseline and at 6th day after the baseline readings have been documented. All the data were analyzed using statistical software, statistical package for the social sciences (SPSS), IBM SPSS version 20.0 (Armonk, NY: IBM Corp.). For all the analyses, p < 0.05 was considered statistically significant. To determine the extent of occurrence of meaningful change, effect sizes for the outcome measures, INFANIB and NIPS were reported in terms of standardized response mean (SRM) using the formulae [23], ES (SRM) = Mean change score / SD change score. Cohen’s criteria for reporting ES (d) [24], ≤0.2 - small change, 0.5 - moderate change, and ≥0.8 –large change were used to report ES obtained. From ES, the power of the study in reporting the neuromotor development and pain outcomes following MMS were estimated by post hoc power analysis using G*Power ver. 3.1.9.4 software (Heinrich- Heine-Universität Düsseldorf, Düsseldorf, Germany; http://www.gpower.hhu.de/). Within the group effect size was estimated using the effect size for Wilcoxon Signed-Ranks test formula, r = z/√N, where N was the total number of observation in the final data analysis. Between the groups effect size was estimated using the effect size for Mann-Whitney U test formulae, r = z/√N, where N was the total sample analyzed in the final data analysis. ES (r) criteria for the use among the non-parametric tests, Wilcoxon Signed-Ranks test and Mann-Whitney U test recommended by Cohen’s (r) were 0.1 - small, 0.3 - moderate, and 0.5 –large [24]. They were used to report the effect sizes for the outcomes among the groups.
Results
Among 32 preterm infants recruited, after one drop-out in each group, 30 preterm infants completed the trial. The demographic dimensions collected, such as gestational age (weeks), birth weight (kg), birth length (cm), occipitofrontal circumference (OFC), and APGAR score at 1-minute and 5-minute were, 34.4±2 weeks, 2.11±0.48 kg, 45±3.8 cm, 32.3±1.7 cm, 7 (4 to 9) and 9 (8 to 10) respectively. Between the groups, demographics were tabulated in Table 2. There exists no significant difference (p > 0.05) bet-ween the groups in their demographic dimensions of preterm infants recruited. Table 3 tabulates the outcome variables of the Preterm infant undergoing MMS recruited in the MMS group (n = 16) and control group (n = 16) with one drop-out from each group. There exist no significant changes (p > 0.05) in weight, length, and OFC of preterm infants between the groups. But significant changes (p < 0.001) were reported for INFANIB and NIPS. ES estimated by SRM for INFANIB and NIPS were found to be, 1.1 and 2.6 respectively in the MMS group, and in the control group, ES were –1.36 and 0.1 respectively. Thus, confirming the study to be sufficiently powered with 97.1%for INFANIB and 100%for NIPS using post hoc power analysis reducing Type-II error < 3%. ES among the groups using the non-parametric tests were displayed in Table 4.
Demographic dimensions of the preterm infant undergoing Multi-Modal Stimulations (MMS) recruited in experimental group (n = 15) and control group (n = 15)
Demographic dimensions of the preterm infant undergoing Multi-Modal Stimulations (MMS) recruited in experimental group (n = 15) and control group (n = 15)
Note: Demographic dimensions does not follow normal distribution. Hence, expressed in median with interquartile range and range. * - Mann-Whitney U test.
Outcome variables of the Preterm infant undergoing Multi-Modal Stimulations (MMS) recruited in experimental group (n = 15) and control group (n = 15)
Effect sizes for the outcome variables of the Preterm infant undergoing Multi-Modal Stimulations (MMS) recruited in experimental group (n = 15) and control group (n = 15)
The study primarily focused on the short-term effects of MMS on neuromotor behaviour and neonatal pain tolerance in stable hospitalized preterm infants. The findings of our study demonstrate that MMS which is comprised of multisensory stimulations and movement therapy is a safe and effective method in improving neuromotor behaviour and dec-reasing pain among the preterm infants when compared to the control group of usual NICU care. MMS administration was observed to have both clinical and statistically significant reduction in INFANIB [4 (2, 6); p = 0.001] and NIPS scores [2 (2,3); p < 0.001] in MMS group when compared to non-significant clinical and statistical reduction in INFANIB [–4 (–6, –2); p = 0.001] and NIPS scores [1 (–1,1); p = 0.778] in control group. The significant difference of 8 (–4, 4); p < 0.001 and 1 (1, 2); p < 0.001 in INFANIB and NIPS scores respectively were observed between the groups. Thus, the null hypothesis was rejected and confirmed the effectiveness of MMS including multi-sensory stimulation and movement therapy on neuromotor behavior and neonatal pain among hospitalized preterm infants. These observations were consistent with the findings of previous research on a similar area of exploring neuromotor development [10] and neonatal pain [12–14].
In addition to the above main findings, significant weight gain of, 62±102 g; p = 0.036 was observed in the MMS group but a weight loss of, 33±235 g was observed in the control group. This was supported by the previous research on multisensory/multimodal stimulation [25]. Significant gain in length and OFC were observed in both groups.
MMS was administered in terms of ATVV along with movement therapy. This addition of movement therapy distinguishes and makes this study unique when compared with previous research [25, 26]. For practical convenience and with consideration of the real-world application, auditory stimuli were not provided with pre-recorded lullabies [25] or any sound produced by the mother as used earlier [25]. Instead, the mother was instructed to produce voice or continuous talk with their preterm infant while feeding. But, the sound level during auditory stimulation was not recorded. As recommended, the permissible sound levels were to be between 45–55 dB [27]. Visual stimulation was provided with a clean and sanitized chessboard. As neonates were attentive to black and white colors only, a chess board (black and white color pattern card) was used at a distance of approximately 20 to 25 cm as recommended earlier. Gentle stroking was used to provide tactile stimulation. As tactile stimulation could produce an arousal effect [28], it was followed by vestibular stimulation [10, 26]. Normal tone development could be attributed to the movement therapy by improving the proprioception and muscle preparedness. However, the mechanism by which actual improvement in neuromotor behaviour and neonatal pain tolerance that is associated with the administration of MMS is still unclear.
All the preterm infants underwent MMS without causing alteration in the physiological states implies the MMS is a safe intervention for preterm infants. These observations were very similar to the previous studies by, White-Traut RC et al. [25, 29] and Kanagasabai P S et al. [10] while performing the multisensory stimulation on preterm infants in the NICU.
There was a non-significant increase in weight gain when compared to the other researches administered by ATVV and H-HOPE intervention [11, 29]. The reason might be the short-term duration (5 days) of MMS intervention when compared to the intervention (approximately 21 days) [29] provided till the discharge of neonates from the hospital.
The study had a few limitations. They are, non-blinding of the therapist who provides intervention and assesses the outcomes as it was a part of doctoral research, recorded NIPS in real-time as against to recommended standard method of documenting pain through video recordings [30], and thereby documented pain outcomes by a single assessor with no inter-rater reliability checks, intervention duration of shorter period and, use of INFANIB among the preterm infants to document the neuromotor behaviour. However, we have used INFANIB only after correcting their gestational age [19] instead of from birth. Overall, cautious interpretation of study results is needed owing to a certain degree of selection bias due to the convenience sampling technique used in the neonate recruitment. This might affect the representativeness of the population.
The strengths of the study are, randomized controlled trial design, a gold standard of experimental design to verify cause-and-effect relationship, the first study that reported the combined effect of MMS and kinaesthetic stimulation on neuromotor behaviour and neonatal pain, all the interventions were provided by the trained neonatal physiotherapist with five years of clinical experience in providing neonatal physiotherapy care and of non-invasive type, attained sufficient sample size with adequate power (97.1%for INFANIB and 100%for NIPS) and thereby minimizing the type-II error < 3%. As we have included the preterm infants born between 28 weeks of gestation to 36 weeks 6 days of gestation, the generalizability of study results could be made to the preterm infants of these gestation weeks. Thus, overall the extrapolation of the clinical trial could be extended to two among the three classifications of preterm by WHO, that is, very preterm (28 to 32 weeks) and moderate to late preterm (32 to 37 weeks). As we have used appropriate study design to verify cause-and-effect relationship, careful data collection to limit information bias, and appropriate statistical analysis to derive the significant difference in the neuromotor behaviour and neonatal pain between the groups, the study findings have sufficient internal validity. Moreover, the study achieved sufficient statistical power to have high generalizability and replication. Thus, the study also has high external validity.
Further, the study could be extended to ascertain the benefits with long-term follow-ups at, 3-month, 6-month, 9-month, and 1-year. A multi-centre trial with double-blinding could be added to this.
Conclusion
The effectiveness of MMS including multi-sensory stimulation and movement therapy on neuromotor behaviour and neonatal pain among hospitalized preterm infants have been verified by the feasibility trial. However, high quality randomized controlled trial with a larger sample size is required to substantiate these effects.
Footnotes
Acknowledgments
The authors express their sincere thanks to Dr. Asir John Samuel, PhD (Physiotherapy), Associate Professor, Department of Pediatric and Neonatal Physiotherapy, Maharishi Markandeshwar Institute of Physiotherapy and Rehabilitation, Maharishi Markandeshwar (Deemed to be University), Mullana, Haryana, India, for providing technical support in editing Figs. 1 ![]() . This feasibility trial form the partial fulfillment for the completion of structured Doctorate of Philosophy / Philosophiae Doctor (PhD) programme by the first author, Mrs. Vencita Priyanka Aranha (Roll No. 2019001 / Regn No. 14-PCM-076).
. This feasibility trial form the partial fulfillment for the completion of structured Doctorate of Philosophy / Philosophiae Doctor (PhD) programme by the first author, Mrs. Vencita Priyanka Aranha (Roll No. 2019001 / Regn No. 14-PCM-076).
Financial Support/ Funding
Mrs.Vencita Priyanka Aranha, first author is being supported by three years PhD Research Fellowship ((MMDU/Ph.D/19/2108 dated 5th Febrauary 2019) from Maharishi Markandeshwar (Deemed to be University), Mullana, Ambala District, Haryana, India during the study period.
Conflict of interest
There is no conflict of interests among the authors.