
Abstract
BACKGROUND:
To determine the clinical implications and gestation age-specific diagnostic predictability of pneumatosis in preterm infants with necrotizing enterocolitis (NEC).
METHODS:
A retrospective study on abdominal radiographs comparing clinical and radiological information in infants with and without pneumatosis.
RESULT:
Our findings disproved our hypothesis. Pneumatosis was seen more frequently in infants with higher gestational age [28.4 (26.1–32.4) vs. 26.4 (24.3–29) weeks; p < 0.001] and birth weight [1110 (762–1768) vs. 770 (645–1022) grams; p < 0.001] and were more likely delivered vaginally (39.1% vs. 21.7%, p = 0.01). Portal venous gas was seen frequently on radiographs (10.3% vs. 0%, p < 0.001), but not pneumoperitoneum (20.7% vs. 36.7%, p = 0.02). Infants with pneumatosis frequently developed acute kidney injury, with higher serum creatinine (16.5% vs. 4.5%, p = 0.02) and frequent oliguria (12.9% vs. 2.7 %; p = 0.043) and had higher C-reactive protein levels at 24 and 96 hours (p < 0.002). Receiver operating curves for pneumatosis showed GA >28 weeks and birth weight > 1000 gm to have a sensitivity of 58.6% and specificity of 72.5%.
CONCLUSION:
Contrary to our hypothesis, infants who developed pneumatosis during NEC were more mature with a higher gestational age and birth weight than those who did not.
Introduction
Necrotizing enterocolitis (N.E.C.) is an idiopathic, acute inflammatory bowel necrosis [1–5] affecting about 3–10% of preterm very-low-birth-weight (VLBW) and some critically-ill term infants with multi-system organ failure [6, 7]. Despite all advances in neonatal care, confirmed N.E.C. remains a leading cause of death in these neonates [5, 8–11].
Abdominal radiography is currently the mainstay of the diagnosis of NEC [12]. The early disease usually shows ileus and bowel loop dilatation, but 50–60% of infants with established N.E.C. develop pneumatosis intestinalis, a pathognomonic finding with intramural radiolucent lesions containing air or bacteria-derived gases [13–15]. Circumscribed lesions in the mucosa/submucosa usually look ‘bubbly,’ whereas the deeper sub-serosal lesions extend between intestinal layers and start looking more linear. Although the pathogenesis of pneumatosis is still not well-elucidated, the best-accepted view of these lesions is as a mark of gas-producing bacteria having invaded the mucosa and in situ carbohydrate fermentation. In early NEC., some of these radiolucent lesions might be dilated intestinal lymphatics. In advanced disease, high intestinal pressures in some areas may cause the luminal gases to tear into the necrotic bowel wall. Pneumatosis intestinalis lesions have been described by other monikers such as pneumatosis cystoides intestinalis, intramural gas, pneumatosis coli, pseudolipomatosis, intestinal emphysema, bullous emphysema of the intestine, and lymphopneumatosis. In infants, > 85% of lesions occur due to NEC, although it could also be an incidental finding in some asymptomatic post-term infants.
This study sought to investigate the clinical impli-cations of radiographically-evident pneumatosis intestinalis in infants with NEC. We reviewed the medical records at the University of Mississippi and identified 207 infants with medical and surgical NEC Similar to earlier studies [15–21], we have not found pneumatosis in all our NEC patients [15, 21]. Postulating that pneumatosis lesions reflect large luminal loads of gas-producing bacteria invading the damaged intestinal mucosa, we hypothesized that the likelihood of detecting these radiological lesions was inversely proportional to gestational age because immaturity of the gut mucosal barrier, tissue perfusion, and mucosal immunity could be visualized as consistent with the current view of its pathogenesis; and so were larger, dysbiotic gut bacterial loads acquired prior to the typically later onset of NEC in the most premature of infants [13, 22–24]. We compared infants with clinically-evident NEC who showed pneumatosis vs. those who did not, for demographics, age of onset of NEC, clinical and radiological signs, postoperative course, and outcomes in terms of the length of hospital stay and mortality.
Methods
This retrospective cohort study was conducted at the level four neonatal intensive care unit (NICU) at the University of Mississippi Medical Center (UMMC.) at Jackson, Mississippi, after approval by the local Institutional Review Board. We identified all infants diagnosed to have NEC from January 2000 to December 2018. Patients identified by the radiologist to have pneumatosis on abdominal radiographs were included in one group. If a radiology report expressed uncertainty with descriptions such as “pneumatosis vs. stool,” we followed subsequent imaging and had cases in the pneumatosis group (a) if the infants were symptomatic and two consecutive abdominal radiographs taken at different times received similar reports; (b) if there were consistent findings such as portal venous gas and/or pneumoperitoneum; and/or (c) if pneumatosis was identified during surgery. If pneumatosis had been identified in earlier radiological reports but not intra-operatively or in histopathology, the infants were still included in the first group because pneumatosis is known to resolve over time [15, 21]. The second group was comprised of patients who did not show pneumatosis but had been classified to have NEC≥stage two because of suggestive clinical signs with loss of bowel sounds, tenderness, and abdominal distension; systemic instability with increased needs for ventilatory and hemodynamic support; radiological signs such as intestinal dilatation, bowel wall edema, and ascites; and histopathological evidence of N.E.C. in surgically-resected bowel. Infants with congenital intestinal anomalies, congenital heart disease, gastroschisis, spontaneous intestinal perforation, and those with suspected NEC with uncertain clinical signs (Bell stage I) were excluded.
Clinical information
We recorded demographic characteristics including gestational age, birth weight, gender, ethnicity (African-American, Caucasian, or Latina/Latinos), mode of delivery, 5-minute Apgar scores, delivery site, and small-for-gestational-age status. Maternal factors were recorded, including pregnancy-induced hypertension, chorioamnionitis, and antenatal steroids. We also collected clinical data such as the administration of surfactant, respiratory distress syndrome, and patent ductus arteriosus (PDA) that was treated medically or surgically.
The features of NEC such as the age of onset, pneumatosis, and clinical presentation (abdominal distension, feeding intolerance, and bloody stools) were noted. Results of blood cultures drawn at the time of NEC onset, use of inotropes at 24 hours, assisted ventilation, and the duration of antibiotic therapy after the onset of NEC was also recorded. In addition, surgical data, such as the affected region(s), length of bowel resected, and the need/site(s) of stomata (indirect markers of severity, need for decompression), were noted.
During the postoperative phase, the duration of ileus (nil per os, NPO), parenteral nutrition (PN; from postoperative day 0 until full enteral feedings defined as 120 mL/kg/day; and time to achieve clinical goals of full enteral feeds were recorded. Persistent cholestasis was defined as direct bilirubin levels ≥2 mg/dL for ≥2 weeks. Short bowel syndrome (SBS) was defined as the administration of parenteral nutrition (PN) for ≥90 days after the onset of NEC or at the time of discharge. The total length of stay (LOS) and mortality were recorded in the hospital. LOS included the number of days of hospitalization both at the referring hospital and at UMMC. Mortality was defined as any-cause death prior to hospital discharge.
Histopathological examination
Hematoxylin & eosin-stained surgically resected intestinal tissues were evaluated for pneumatosis by a blinded pathologist.
Hematological information
We noted complete blood counts (CBCs) and white blood cell (WBC) counts recorded prior to the onset, the day of onset, and at 24–48 hours after onset. We recorded the most abnormal results if multiple CBCs were available from a particular day.
Renal function data
We captured serum creatinine (SCr) measurements and daily urine output (UOP) prior to and for five days after the onset of NEC AKI was defined using the modified neonatal staging criteria described in the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines (25–29): stage 1: increased SCr by 1.5–1.9× baseline or by ≥0.3 mg/dL, or UOP < 0.5 mL/kg/hour for 6–12 hours; stage 2: increased SCr by 2–2.9× of baseline or UOP < 0.5 mL/kg/hour for ≥12 hours; stage 3: increased SCr by 3× baseline or to 4 mg/dL, need for renal replacement therapy, or UOP < 0.3 mL/kg/hour for ≥24 hours.
Statistical methods
Patient demographics and clinical information were compared between infants with and without pneumatosis. Continuous data were summarized with medians and interquartile ranges and compared using the Mann-Whitney U or the Kruskal-Wallis H tests. Categorical variables were reported with frequencies and percentages and compared using the chi-squared tests. We also computed pneumatosis’s receiver-operating characteristics (ROC) by plotting sensitivity vs. 1-specificity. ROC models based on gestational age/birth weight were used to calculate/predict sensitivity, specificity, and positive and negative predictive values. A p-value < 0.05 was considered significant. All statistical analyses were performed in SAS software.
Results
We identified 207 infants with N.E.C., including 96 with confirmed medical (Bell stage ≥2) and 111 with surgical disease. The median gestational age was 27 (IQR 25–30.4) weeks, and the birth weight was 900 (675–1375) grams. There were 126 (60.9%) males, 153 (74.3%) were African-American, and 147 (71%) were delivered by cesarean section. The median age of N.E.C. onset was 15 (8–29.5) days. This cohort had 104/207 (50.2%) infants with P.D.A.; 26 (12.9%) were treated with cyclooxygenase inhibitors (indomethacin/ibuprofen) before the onset of N.E.C.
Abdominal radiographs showed pneumatosis in 87/207 (42%). Pneumoperitoneum was seen in 62/207 (30%) and portal venous gas in 9/207 (4.3%). In surgical sub cohort, infants with pneumatosis received less Penrose drain (10/47, 21% vs 30/64, 47%) and underwent laparotomy more frequently (37/47, 79% vs 34/64, 53%) as the initial surgical intervention compared to infants without pneumatosis. Blood cultures were positive in 57 (27.5%) at the time of NEC onset and were treated with antibiotics for a median of 7 (5–10) days following the diagnosis. Forty-seven (22.7%) infants died. The median length of hospital stay was 95 (46.5–151) days. The other demographic and clinical findings are summarized in Table 1a and 1b.
Clinical, NEC features and demographic information in neonates with pneumatosis and no pneumatosis in combined Cohort
Clinical, NEC features and demographic information in neonates with pneumatosis and no pneumatosis in combined Cohort
Abbreviations: NEC = necrotizing enterocolitis Continuous variables are as median with interquartile range (IQR). When the normality assumption was not satisfied, continuous measures’ statistical associations were tested with the Mann-Whitney U test. Categorical variables are presented as count (column percentage). Differences in categorical measures’ associations were tested using the Chi- square test. The presence of bold values signifies p < 0.05.
Clinical and laboratory information in neonates with pneumatosis and no pneumatosis in combined Cohort
Abbreviations: NEC = necrotizing enterocolitis; CRP = c-reactive protein; WBC = white blood cell; ANC = absolute neutrophil count. Continuous variables are as median with interquartile range (IQR). When the normality assumption was not satisfied, continuous measures’ statistical associations were tested with the Mann-Whitney U test. Categorical variables are presented as count (column percentage). Differences in categorical measures’ associations were tested using the Chi- square test. The presence of bold values signifies p < 0.05.
Table 1a and 1b show demographic characteristics and clinical factors of infants who developed pneumatosis and those who did not. Neonates with pneumatosis were born at higher gestational ages [28.4 (26.1–32.4) vs. 26.4 (24.3–29) weeks, p < 0.001]; and higher birth weights [1110 (762–1768) vs. 770 (645–1022) grams, p < 0.001]. They were vaginal births more frequently (39.1% vs. 21.7%, p = 0.01). More infants with pneumatosis showed portal venous gas (10.3% vs. 0%, p < 0.001) and but fewer showed pneumoperitoneum (20.7% vs. 36.7%, p = 0.02). Infants with pneumatosis developed AKI≥stage 3 by serum creatinine (16.5% vs. 4.5%, p = 0.02) and urine output (12.9% vs. 2.7 %; p = 0.043) more frequently compared to those without these lesions. These infants had higher CRP levels at 24 and 96 hours (p < 0.01) and frequently showed abnormal CBCs (p < 0.005).
Pneumatosis on histopathology in surgical sub cohort
In our 111 patients with surgical N.E.C., 47 (42.3%) showed pneumatosis on abdominal radiography. Twenty-nine (29/47, 61.7%) showed confirmed pneumatosis lesions on histopathology. In 64 infants who did not show pneumatosis on radiology, 15/64 (23.4%) showed lesions in histopathology.
In neonates with surgical NEC, blood culture was positive for one type of organism in 19% (9/47) of patients with pneumatosis and 18.8% of cases in the non-pneumatosis group. In pneumatosis, blood culture was positive for the gram-negative organism in 12.8% (6/47) and gram-positive in 10.6% (5/47) infants. Klebsiella and E.coli were the most common gram-negative organisms, while Staphylococcus epidermidis was the most common gram-positive bacteria in neonates with pneumatosis. The data has been summarized in Table 2.
Microbiology data in neonates with surgical necrotizing enterocolitis
Microbiology data in neonates with surgical necrotizing enterocolitis
Abbreviations: NEC = necrotizing enterocolitis.
*In the neonates with pneumatosis, one infant with a positive blood culture had a polymicrobial infection that involved Staphylococcus warneri + Candida albicans.
*In the neonates with pneumatosis, one infant with a positive blood culture had a polymicrobial infection that involved Staphyloccus epidermidis + Serratia marcesens.
Data is presented as count and percentage. Polymicrobial is defined as a blood culture with more than one organism.
*In the neonates without pneumatosis, one infant with a positive blood culture had a polymicrobial infection that involved Staphylococcus warneri + Staphyloccus epidermidis + Enterococcus faecalis.
*In the neonates without pneumatosis, three infants with positive blood cultures had polymicrobial infections. Organisms involved in the polymicrobial cultures were as follows:
ROC models based on a gestational age cutoff < 28 weeks and birth weight < 1000 grams showed pneumatosis on abdominal radiographs to have a sensitivity of 58.6% and specificity of 72.5% to detect NEC. For infants with surgical and medical NEC, the positive and negative predictive value has been summarized in Table 3 and Fig. 1. The predictive probabilities of the pneumatosis by gestational age in preterm infants with medical and surgical NEC has been shown in Fig. 2.
Model Values By Gestational age < 28 weeks and birth weight > 1000 gms in preterm infants with NEC
Model Values By Gestational age < 28 weeks and birth weight > 1000 gms in preterm infants with NEC
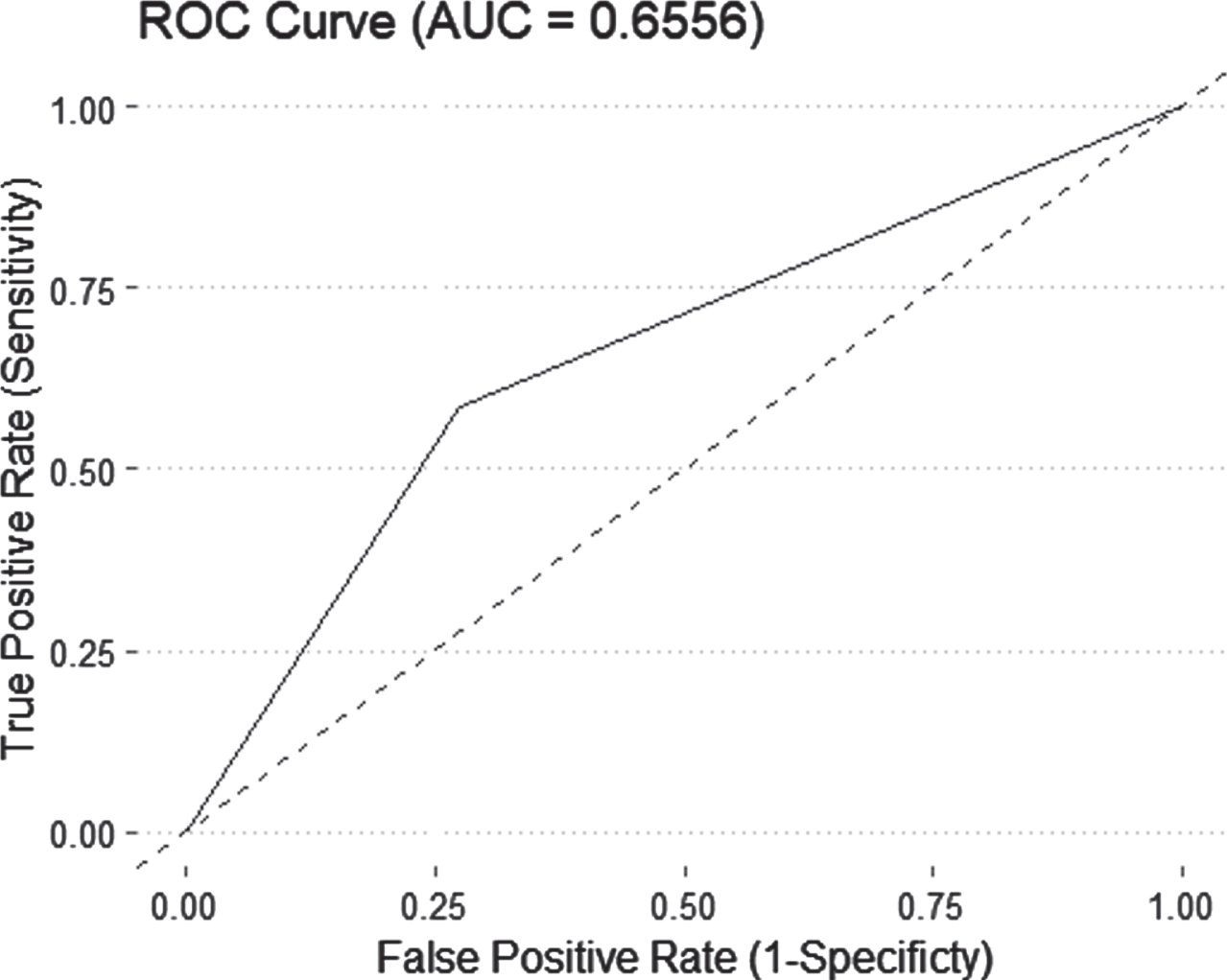
The Receiver Operative Curve for preterm infants with medical and surgical necrotizing enterocolitis. Receiver operating curve (R.O.C.) and area under the curve (A.U.C.) of pneumatosis in neonates with necrotizing enterocolitis. Parameters include pneumatosis in neonates with gestational age < 28 weeks and birth weight < 1000 grams.
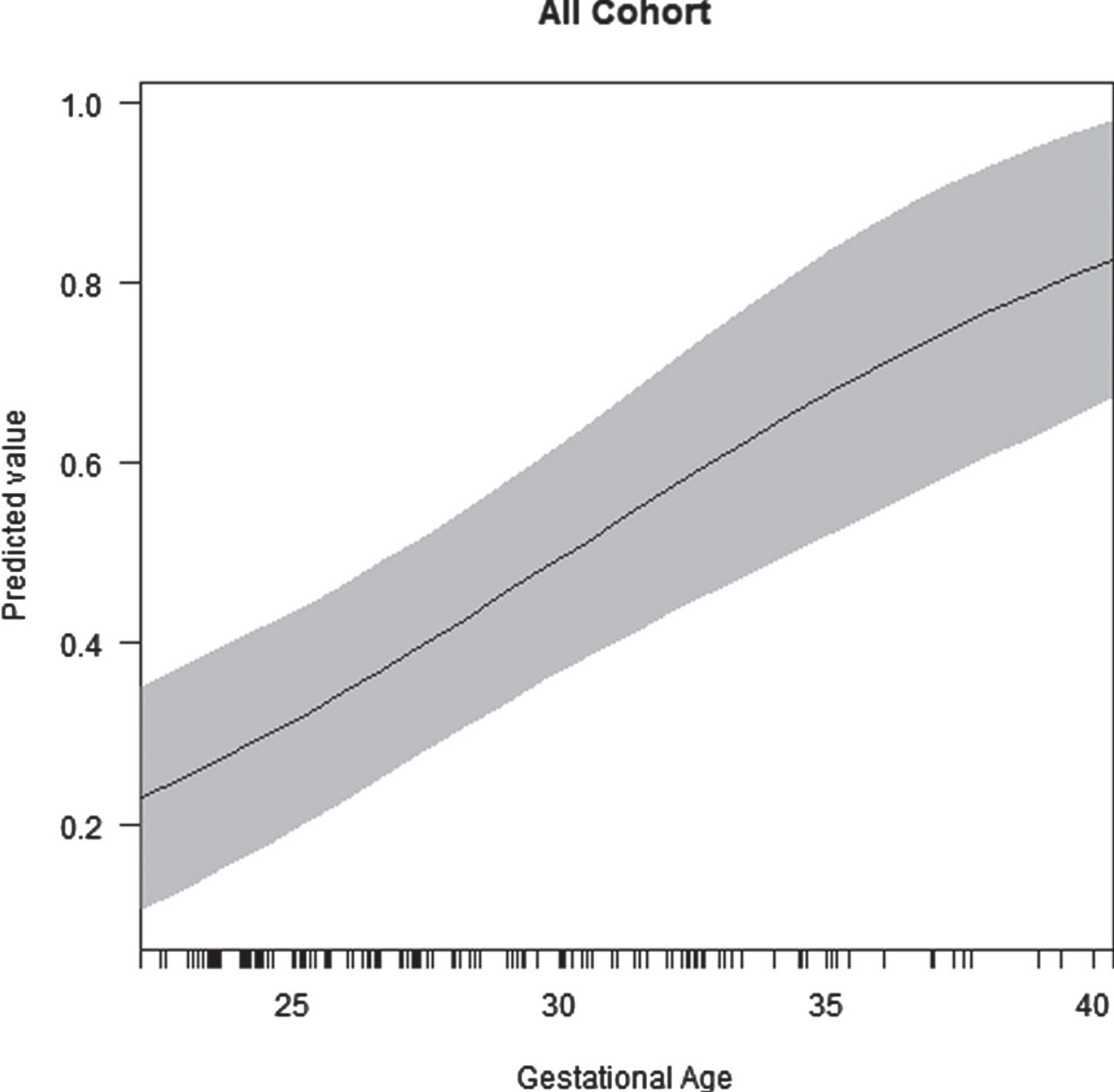
Predictive probabilities of pneumatosis to detect N.E.C. by gestational age in preterm infants with N.E.C.
In our study, infants with pneumatosis had a median gestational age of 28.4 weeks and a birth weight of 1.1 kg, higher than those without pneumatosis. These findings are most likely due to a thin intestinal wall and rapid progression of the disease process resulting in pneumoperitoneum (20.7% vs. 36.7 %) in neonates without pneumatosis. In addition, pneumatosis was seen more frequently in infants with a median gestational age of 28.4 weeks than 26.4 weeks in the group that did not show pneumatosis. In comparison, our study yielded a sensitivity of 53.2% and specificity of 82.8%, PPV of 68.4%, and A.U.C. of 68% for infants with surgical N.E.C. In another report, Sharma et al. also reported pneumatosis only in 29% of infants with gestational age between 23 to 26 weeks compared to infants with higher gestational age [13].
In the literature, very few studies have discussed the correlation between gestational age and radiological findings such as pneumatosis in NEC [13, 14]. Battersby et al. [14] performed a prospective study of 3866 infants, where 888 developed NEC, and 2978 did not. They reported that infants who developed NEC and had a gestational age < 26 weeks were less likely to present with pneumatosis (31.1% vs. 47.2%; p = 0.01) than patients born with a gestational age > 30 weeks. In their study, sub-analysis of 431 infants who underwent a laparotomy yielded a sensitivity of 76.5% (95% CI, 70.0–82.1), a specificity of 74.4 % (95% CI, 68.3–80.0), an AUC of 75.0% (95% CI, 71.0–80.0), and a PPV of 72.9% (95% CI 66.4–78.7). In comparison, we found a cutoff of 28.4 weeks in preterm infants who were most likely to have pneumatosis on abdominal X-rays. Another study of 89 infants (from the Swedish national quality register) with medical (32/89) and surgical N.E.C. (n = 57/89) by Palleri et al. [30] had also reported a greater incidence of pneumatosis (86.2% vs. 60%) in infants with gestational age more than 28 weeks which is similar to our study findings. However, they did not report birthweight cutoff, clinical implications, and histological correlation of pneumatosis in preterm infants with N.E.C. Our findings validate the published data and the need for gestational age and birth weight-based case definition to help us accurately diagnose necrotizing enterocolitis. Our study also demonstrated the discrepancy between pneumatosis’s radiological and histopathological presence.
The pneumatosis at a later age of NEC onset could be explained due to establishment of the gut microbiome by gas-producing bacteria by 3-4 weeks of life and translocation of gas-producing bacteria to the subserosa layer. La Rosa et al. [31] have shown that gut microbiota of premature infants residing in a tightly-controlled microbial environment progresses through a choreographed succession of bacterial classes from Bacilli to Gammaproteobacteria to Clostridia, interrupted by abrupt population changes. They have also demonstrated as infants approach a postconceptional age of 33–36 weeks (corresponding to 3–12 weeks of life depending on gestational age at birth), anaerobes well colonize the gut. The progression of microbiota was slowest in infants with lower gestational age, which can explain the lower frequency of pneumatosis in infants with gestational age < 27 weeks. In another report by Wang et al. [32], the intestinal microbiota of preterm infants with N.E.C. has fewer bacterial species, less diversity, and increased proportions of the potential pathogen with a predominance of Proteobacteria. In our study, blood cultures at the time of NEC onset also predominantly grew E. coli and Klebsiella spp. in neonates with pneumatosis. Our study lacks microbiome data in infants with and without pneumatosis.
Another possible explanation of pneumatosis in preterm infants is the immaturity of the gut barrier [33, 34]. A recent study by Henderickx et al. [33] showed that the fecal proteome of preterm infants was deprived of gastrointestinal barrier-related proteins during the first six postnatal weeks compared to term infants. Another study of resected human small intestine tissue has shown that the increased gut permeability in NEC might be related to decreased occludin with an increase in myosin light chain kinase (MLCK), an important regulator of tight junction permeability [35]. In this cohort, neonates with pneumatosis had consistently higher C-reactive protein levels following the onset of NEC, suggesting a sustained inflammatory response. These infants also developed AKI more frequently, evident as increased serum creatinine levels and lower urine output. In a recently published report, we have shown sepsis to be an independent predictor (aOR = 3.5; 95% CI = 1.3, 10.0) of severe AKI stages 2-3 on the K.D.I.G.O. classification) in infants with NEC [36]. These findings are similar to those reported by Coggins et al. [37]; they showed that infants (n = 203) with late-onset sepsis had increased odds (aOR, 3.0; 95% CI 1.5–6.2; p = 0.002) and severity AKI within seven days of onset of sepsis compared with age-matched infants without sepsis. The published reports have suggested that the most likely explanation of sepsis-associated neonatal AKI may be related to hypovolemia, altered hemodynamics, inflammation, and nephrotoxic medications [38, 39].
More recently, Rehan et al. [40] showed considerable observer variability in individual radiological signs. In this study, trained observers performed better than in training, but the radiological signs in isolation were unreliable. Another study used the Duke Abdominal Assessment Scale (DAAS), a 10-point numeric scale of radiological signs with intra-observer and interobserver agreement by weighted κ values. The agreement was at levels of 0.635–0.946 for the intra-observer agreement and 0.574–0.898 for the inter-observer agreement [22]. In our cohort, we did not use any numeric scale of radiological signs mainly due to reported high inter-observer variability in the interpretation of radiological signs.
This study’s strengths include a comprehensive description of the pneumatosis in a consecutive cohort of neonates with surgical NEC predominantly in African American population. This description had a demographic, clinical, laboratory and postoperative outcomes. We also correlated and confirmed radiological findings with resected intestinal histopathology. Our study also validates the reported data on a gestational age-based case definition for NEC. However, our study is limited by its single-center cohort, retrospective design, and relatively small sample size. There may have inadvertent inclusion of some cases with diagnosis of spontaneous intestinal perforation. These difficulties reduce the generalizability of the results and the statistical power to detect other important associations between pneumatosis and clinical outcomes in neonates with NEC.
In conclusion, our study demonstrates that pneumatosis might be a more sensitive and specific sign of N.E.C. in neonates with gestational age > 28 weeks and birth weight > 1000 gm. Our data add to the guidance available to bedside care providers in referring hospitals for timely referral of infants with NEC Our data gives guidance to look for other radiological findings besides pneumatosis in neonates with suspected NEC. However, there is a need for prospective studies to include non-invasive markers [40] of NEC. such as urinary fatty acid-binding protein or claudin 3 with radiological signs, including sonography findings in suspect cases of NEC. In addition, there is a need to have standardized criteria to define N.E.C. in infants with clinical and radiographic features of NEC [24] to reduce observer variability and decrease false-negative and false-positive reporting. Finally, there is an urgent need to revise the Bell classification for N.E.C. to improve our definition, timely diagnosis, treatment, and possibly, enrollment in collaborative national and international efforts.
Footnotes
Author contribution
P.M. Garg designed, collected, analyzed, and wrote the manuscript. J. Paschal: collected/analyzed the data and wrote the manuscript. M.A.Y Ansari: Analyzed the data and wrote the manuscript. S.Chen and C Grey analyzed the data and wrote the manuscript.
H Sonani, Neha Varshney and W. Hillegass collected and analyzed the data and wrote the manu-script. All authors approved the manuscript.
Conflicts of interest
The authors disclose no conflicts.
Acknowledgments
We would like to thank Dr. Akhil Maheshwari from Global Newborn Society for all the guidance for the project. We would like to thank Dr. Redline from Case Western University and Dr. Suhas G. Kallapur from UCLA Mattel Children’s Hospital for all the guidance for the project.
Funding
Dr. Parvesh Garg is partially supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 5U54GM115428. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Consent
Patient consent was not required for de-identified retrospective data.