
Abstract
BACKGROUND:
Thrombocytopenia absent radius (TAR) syndrome is a rare disease with an estimated prevalence of one in 200,000 live births. TAR is associated with cardiac and renal anomalies as well as gastrointestinal problems such as cow’s milk protein allergy (CMPA). Typically neonates with CMPA present with mild intolerance, with few reports in the literature of more severe intolerance resulting in pneumatosis. We present a case of a male infant with TAR syndrome who developed gastric and colonic pneumatosis intestinalis.
CASE DESCRIPTION:
An eight-day-old male infant born at 36 weeks gestation with a diagnosis of TAR, presented with bright red blood in his stool. At this time he was on full formula feeds. Given continued bright red blood within his stool, an abdominal radiograph was obtained which was consistent with colonic and gastric pneumatosis. A complete blood count (CBC) was notable for worsening thrombocytopenia, anemia and eosinophilia. Once enteral feeds were held there was rapid resolution of the radiographic findings and resolution of his bloody stool. He was ultimately diagnosed with a CMPA.
CONCLUSION:
Though there are reports of CMPA in patients with TAR, the severity of this patient’s presentation with both colonic and gastric pneumatosis is unique. Without the knowledge of the association of CMPA with TAR, this case could have been misdiagnosed and led to reintroduction of cow’s milk containing formula, resulting in further complications. This case highlights the importance of a timely diagnosis and severity of CMPA in this population.
List of abbreviations
Thrombocytopenia absent radius
Cow’s milk protein aller
Neonatal intensive care unit
Complete blood count
Glucose infusion rate
Expressed breast milk
Total parenteral nutrition
nutrition NEC
Introduction
TAR syndrome is a rare disease with an estimated prevalence of one in 200,000 live births [1]. TAR is associated with cardiac and renal anomalies as well as gastrointestinal problems such as CMPA. In the majority of patients with TAR, CMPA presents with mild intolerance with either vomiting or poor weight gain. However, there are some reports in the literature that detail more severe intolerance including pneumatosis. To our knowledge this is the first case report to detail both colonic and gastric pneumatosis as a complication of CMPA in a neonate [1–3].
Case description
A male infant born at 36 weeks’ gestation was admitted to the neonatal intensive care unit (NICU) for management of TAR syndrome. He was born to a 36-year-old gravida 1 para 0 woman with a history of chronic hypertension and diet-controlled diabetes. She had an anatomy scan suggestive of fetal arthrogryposis so underwent an MRI that demonstrated bilateral absent radii. Fetal echocardiogram was normal. Genetic testing during pregnancy was declined. He was born via cesarean section in the setting of severe maternal preeclampsia. At birth, the infant was vigorous with a birth weight of 2.4 kilograms (24%) but was noted to have multiple limb anomalies including limited elbow extension with flexed wrists and clenched hands and a left knee dislocation. Radiographs of the upper extremities confirmed absence of the radii bilaterally, thus a CBC was drawn to measure baseline platelets given concern for TAR syndrome. The initial platelet level on DOL 0 was 69,000/μL without an appropriately elevated immature platelet fraction, making TAR the most likely diagnosis; thus, confirmatory genetic studies were sent and hematology was consulted.
The infant’s initial hospital course was further complicated by hypoglycemia at birth that required a maximum glucose infusion rate (GIR) of 11 mg/kg/min in the form of IV dextrose in addition to small volume enteral feeds with either expressed breast milk (EBM) or cow’s milk-based formula. Given persistent hypoglycemia beyond three days requiring IV dextrose, he underwent an endocrinology evaluation and ultimately had a glucagon stimulation test with a positive response, thus suggestive of transient hyperinsulinism, likely secondary to maternal gestational diabetes. He was continued on enteral feeds that were then fortified to 24 calories per ounce in an attempt to improve glucose control. Given recurrent episodes of hypoglycemia despite fortification, his gavage feeds were run over two hours, which allowed him to successfully wean off of total parental nutrition (TPN) with stable blood glucoses. In addition, he was allowed to take a limited amount of feeds by mouth for oral stimulation. He had normal stooling patterns and did not have emesis associated with feeds or other evidence of feeding intolerance.
On the morning of day of life eight, he was noted to have a small amount of bright red blood in his diaper. Upon further examination he was noted to have an anal fissure, and given a reassuring abdominal exam without distension or pain on palpation, enteral feeds were continued. However, that same afternoon he had a large frank bloody bowel movement. His physical exam at this time was notable for slight abdominal distension, however, he remained active without evidence of pain on palpation of the abdomen. Enteral feeds were held and an abdominal radiograph and CBC were obtained. His CBC was notable for a normal white blood cell count, worsening thrombocytopenia of 45,000/μL down from 56,000/μL, and a hematocrit of 29% down from 35%. Up until this time his platelets, which were trended on a daily basis, were typically greater than 60,000/μL. The CBC was also notable for eosinophilia, with 12% eosinophils, which peaked the following day at 17%. The abdominal radiograph (Fig. 1) demonstrated both colonic and gastric pneumatosis, without evidence of free intraperitoneal air. Given these findings in the setting of frank bloody stools and thrombocytopenia, he was transfused with platelets and packed red blood cells. He was started on vancomycin and piperacillin-tazobactam for presumed necrotizing enterocolitis (NEC). Later that night, while receiving the blood transfusion, he had a fever, which peaked at 38.5 degrees Celsius. While febrile, he was tachycardic with stable blood pressures. His exam was notable for increasing abdominal distension and lethargy. However, once he defervesced, his activity level returned to baseline and was no longer febrile for the remainder of his hospital stay.
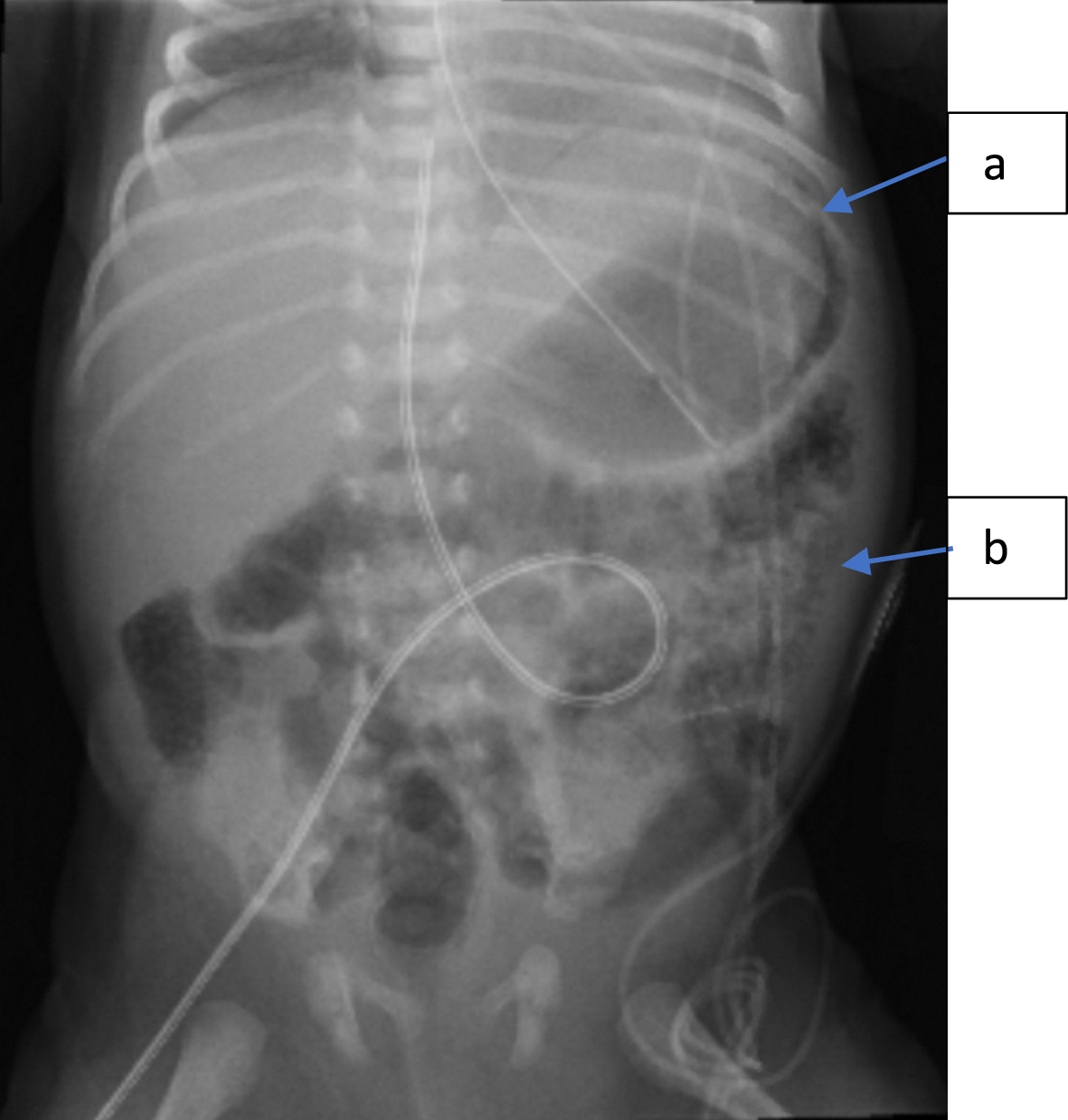
Abdominal radiograph demonstrating (a) gastric pneumatosis and (b) colonic pneumatosis as depicted by the blue arrows.
Abdominal radiographs improved, with no gastric pneumatosis and limited colonic pneumatosis seen on a serial radiograph obtained twelve hours later with complete resolution of findings after 48 hours of bowel rest (Fig. 2). He no longer had bloody stools and his antibiotic therapy was narrowed to monotherapy with piperacillin-tazobactam to complete a one-week course for possible NEC.
After completion of the antibiotic course, the infant was restarted on feeds with Alimentum, a hydrolyzed formula. His mother underwent a dairy exclusion diet with plans to reinitiate EBM feeds after a two-week period of dairy exclusion. He was discharged home on Alimentum feeds, tolerating all feeds by mouth without any further episodes of bloody stools. One month after discharge from the NICU, he continues to tolerate his Alimentum feeds supplemented up to two feeds daily of EBM, while the mother continues a dairy exclusion diet. He has not required any further platelet transfusions, with platelets stable at 110,000/μL at his most recent check at two months old and he has not had any further bloody stools.
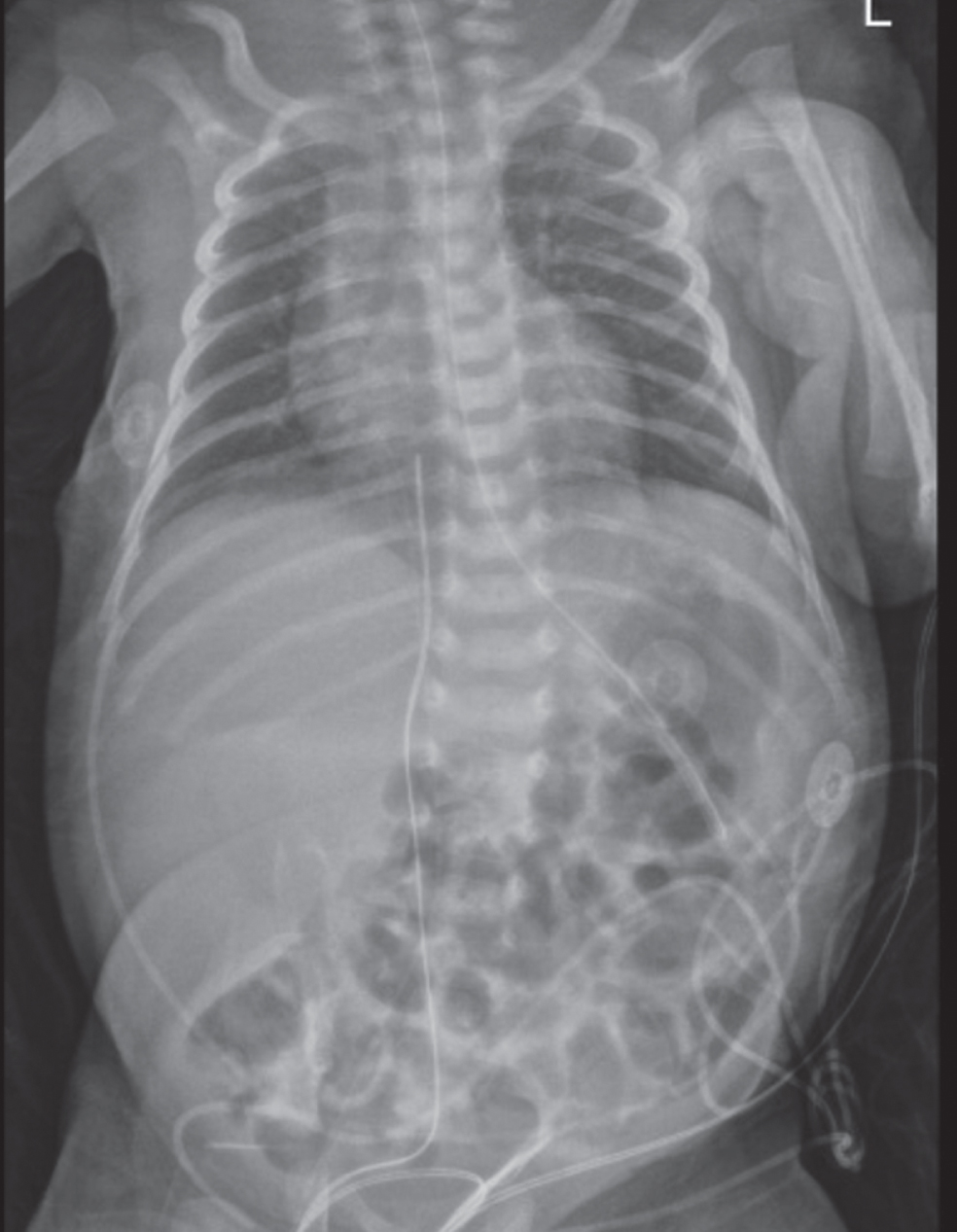
Abdominal radiograph 48 hours after initial abdominal radiograph with complete resolution of pneumatosis.
TAR syndrome is a rare disease with an estimated prevalence of one in 200,000 live births [1]. It represents a congenital malformation syndrome that is characterized by the combination of bilateral absence of the radii with presence of both thumbs and thrombocytopenia. It is a result of a deletion on chromosome 1q21 [1]. Besides the hallmark features of TAR, 16–22% will have cardiac anomalies most commonly being septal defects rather than complex cardiac lesions and 25% will have renal anomalies with duplicated ureter, horseshoe kidney and dilated renal pelvis being the most common [1, 2].
Gastrointestinal problems are common in this population with one case series of 34 patients reporting an incidence of CMPA of 61% [3]. Within this cohort, 67% of infants with CMPA, presented with mild intolerance, detailed as poor weight gain and vomiting, 23% had moderate intolerance presenting with failure to thrive and diarrhea, and 10% had severe intolerance requiring TPN therapy [3]. Episodes of more significant thrombocytopenia can occur in those individuals with CMPA, who are fed with cow’s milk containing formula [3–5]. In individuals with CMPA, gastroenteritis and thrombocytopenia tend to improve with age and are less likely to be triggered by cow’s milk protein exposure [3].
To our knowledge this is the first report of gastric and colonic pneumatosis in an infant less than 2 weeks of age with TAR. There is only one other case report in the literature detailing severe complications of an infant with TAR and CMPA. In this case, a full-term infant’s course was complicated by recurrent periods of severe diarrhea, bloody stools, dehydration, failure to gain weight, eosinophilia and worsening thrombocytopenia each time enteral feeds with cow’s milk formula were introduced. Although abdominal radiographs never revealed pneumatosis, she ultimately was found to have an intestinal obstruction requiring a colostomy. Her symptoms finally improved with a soy-based formula, with adequate weight gain, and resolution of her eosinophilia and feeding intolerance [4]. The other reports within the literature are mainly case series, that detail moderate CPMA, with infants developing bloody stool and worsening thrombocytopenia [3, 5].
The differential diagnosis for this case was pneumatosis intestinalis due to severe CPMA and NEC. Several factors led the team to believe that this patient’s presentation was secondary to severe CMPA and not NEC; most notably the infant’s rapid clinical improvement once feeds were held, rapid improvement in abdominal radiographs (Fig. 2), eosinophilia noted on the CBC, and his older gestational age. Although this is the first report of gastric and colonic pneumatosis in an infant with TAR, there are a few case reports in the literature of pneumatosis in children who had CMPA [6–8]. In one case, an infant born at 26 weeks gestation had recurrent allergic enterocolitis mimicking NEC, when fortified EBM was introduced, and once an amino acid formula (e.g. Neocate), was introduced there was resolution of symptoms with improvement in radiographic findings [7]. In another case, a full term infant developed intestinal perforation at one month of age, after repeated exposure to cows’ milk formula despite multiple admissions for diarrhea, abdominal distention and vomiting [8]. In our patient, when feeds were reintroduced, he tolerated feeds with an extensively hydrolyzed formula, as evidenced by weight gain, and a normal stooling pattern, without bloody or loose stools. Extensively hydrolyzed formula differs from Amino Acid based formula, in that the nitrogen source in extensively hydrolyzed formula is from whey or casein, whereas the nitrogen source in Amino Acid based formula is from amino acids. Ten percent of cases of CMPA will not tolerate feeds even with an extensively hydrolyzed formula; therefore, in these cases an Amino Acid based formula will be required [9].
This is an important case that shows how severe the presentation of CMPA can be in a patient with TAR. Though it is reasonable to attempt feeds containing cow’s milk protein, especially in infants who are breastfed, it is vital to provide appropriate anticipatory guidance and close follow up, to ensure that feeds are being tolerated.
Disclosure statement
The authors declare no conflicts of interest.