
Abstract
INTRODUCTION:
The coronavirus disease (COVID-19) has created a serious health problem in pregnant people. We aimed to address whether vaccination can prevent development of placental disease in SARS-CoV-2 infected mothers.
METHODS:
We reported the pathology findings obtained from routine histopathological examination of placentas of overall 38 cases.
RESULTS:
We found low prevalence of placental pathology in vaccinated pregnant people with active SARS-CoV-2 infection in comparison to those unvaccinated cases.
CONCLUSION:
Based on our findings, SARS-CoV-2 vaccination can prevent development of placental pathological lesions and may lower the risk of serious illness in pregnant people.
Introduction
The emergence of the pandemic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and the coronavirus disease (COVID-19) has created a serious public health problem in every population class such as pregnant patients. Several reports suggest an increased risk of placental lesions due to malperfusion and inflammation in patients with SARS-CoV-2 infection [1–3].
Vaccines against SARS-CoV-2 have been approved for emergency use and recommended for all people including patients who are pregnant. The vaccine is shown to be safe and effective at any stage of pregnancy and provides better outcome against infection [4]. The aim of our study is to address whether vaccination can prevent the development of placental disease in pregnant patients with active COVID-19. The study was approved by the Institutional Ethical Committee.
Methods
In this retrospective cohort study, the data were anonymous and the requirement for informed consent was therefore waived. The study was approved by the Institutional Ethical Committee. We reported the findings obtained from routine histopathological examination of placentas of patients with COVID-19 to address the preventive effect of vaccination. The patients who were tested simultaneously and found positive for SARS-CoV-2 variant infection on polymerase chain reaction at delivery between September and November 2021 were enrolled. Of overall 38 participants, 20 were unvaccinated and 18 received two doses of Pfizer-BioNTech vaccine prior to delivery. The vaccinated group was given first dose of vaccine in June when vaccination was currently open in the country to all people at the age of 15 and above. Because with the most common variant of the virus (Delta variant) at that period, two doses were needed to give a good level of immunity, and second dose of the Pfizer-BioNTech vaccine was given 8 weeks after the first dose exclusively before the third trimester.
The placentas were sampled on routine examination as described previously and histopathological examination was done on Hematoxylin-Eosin (H&E) stained sections [5]. According to the Amsterdam criteria, the histopathologic lesions found in the placental examination were defined into the following subcategories: no placental pathology, maternal vascular malperfusion (MVP), fetal vascular malperfusion (FVM), acute inflammatory pathology (AIP) such as chorioamnionitis, chronic inflammatory pathology (CIP) such as villitis of unknown etiology, increased perivillous fibrin (IPF), intervillous thrombosis and others [5].
Results
The mean ages of the unvaccinated and vaccinated patients were 29.5 + 5.0 and 29.7 + 3.7 years, respectively. There was no statistically significant difference like the mean gestational ages which were 37.7 + 4.1 and 36.5 + 4.5 weeks, respectively.
Table 1 demonstrates the placental lesions found in the histopathological examination. Non-vaccination was associated with the development of placental disease in pregnant patients with active COVID-19 revealing that vaccination appears to have a preventive effect. No placental pathology was shown in 10 of 18 vaccinated cases (55.6%). In contrast, only 3 placentas of 20 (15%) unvaccinated cases were normal with statistically significant difference (chi-square test, p = 0.005). The MVM was the most common placental pathological lesion in 14 (70%) of unvaccinated cases and 16 (44.4%) of overall patients. The specific findings in this group were accelerated villous maturation and villous infarction (Figs. 1, 2). The second common pathological lesion following MVM was IPF found in four (11.1%) of overall 36 cases.
Placental histopathological lesions in comparison with vaccination status in pregnant patients with SARS-CoV-2
Placental histopathological lesions in comparison with vaccination status in pregnant patients with SARS-CoV-2
Abbreviations: MVM: maternal vascular malperfusion, FVM: vascular malperfusion, AIP: acute inflammatory pathology, CIP: chronic inflammatory pathology, IPF: increased perivillous fibrin.
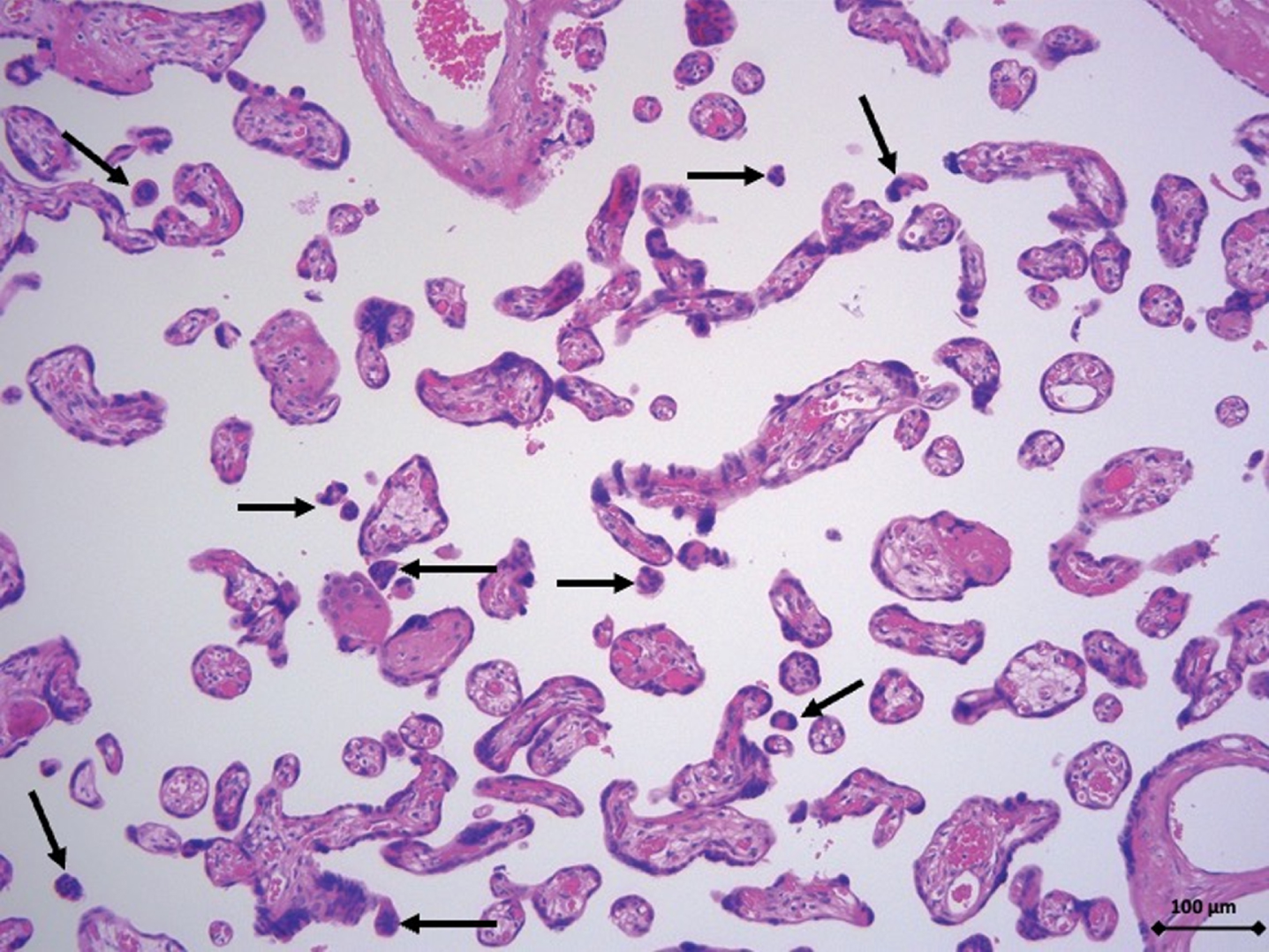
Accelerated villous maturation characterized histologically by villous paucity and increased syncytial knots (black arrows). Hematoxylin-Eosin staining (cell nuclei are stained purple and cytoplasm pink), x100 magnification. Scale bar: 100μm.
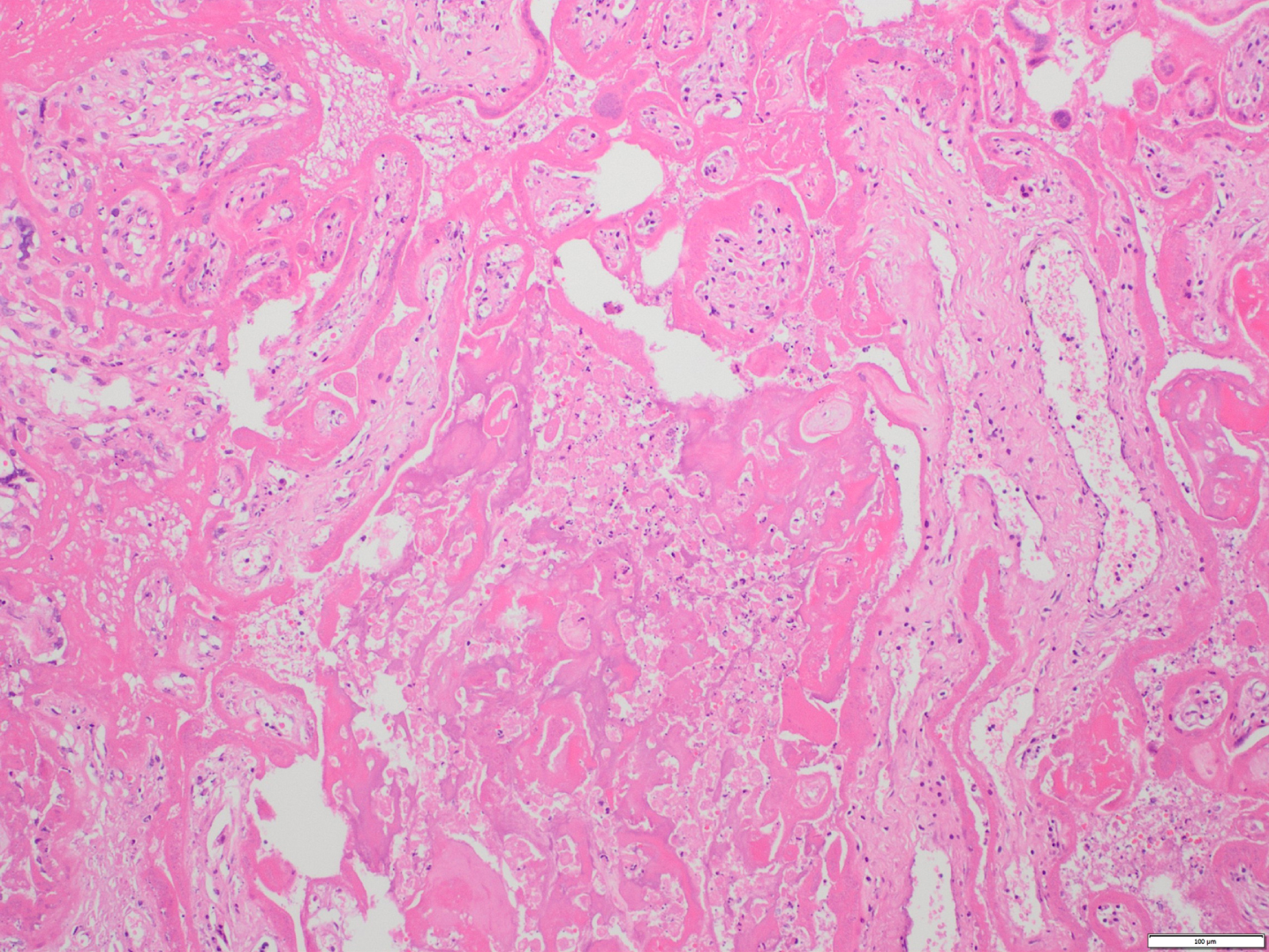
A villous infarct characterized histologically by contiguous degenerating villi showing collapse of the intervillous space with intervening fibrin and degenerative changes in the villous stroma. Hematoxylin-Eosin staining, x100 magnification. Scale bar: 100μm.
Covid-19 can affect pregnant people because they become an extremely sensitive group during any pandemic of viral infections due to altered immune functions and susceptibility to infection. In addition, SARS-CoV-2 infection has been reported to potentially affect the placenta and cause placental pathology.
Vaccines against SARS-CoV-2 have been recommended for all people including pregnant patients. To the best of our knowledge, the prevalence of placental pathology in vaccinated pregnant patients with active SARS-CoV-2 infection has not yet been compared with those unvaccinated cases. We therefore aimed to address whether vaccination can prevent the development of placental disease in SARS-CoV-2 infected mothers and found that vaccination has a preventive effect.
There are some limitations of our study including the lack of ability to identify causal mechanisms, lack of pregnancy and neonatal outcomes data, and small number of vaccinated and unvaccinated cases. Besides, it is not possible to compare placental findings by type of vaccine because all patients were vaccinated with the same type of vaccine.
Despite limitations in the study, our findings reveal that SARS-CoV-2 vaccination in pregnancy is associated with a significantly lower prevalence of pathological changes in the placenta. Thus, COVID-19 vaccination likely lowers the risk of newborn morbidity in pregnant patients with SARS-CoV-2, minimizing the impact of the virus on the placenta and fetal environment. In addition, our findings add to the growing literature supporting the effect of SARS-CoV-2 infection in pregnancy on development of placental pathologies.
In conclusion, we compared placental pathology in pregnant COVID positive patients who were and were not vaccinated. Our findings show that vaccination can protect their placenta and prevent development of the placental pathologies.