
Abstract
BACKGROUND:
Little is known about preterm infant feeding and growth in the outpatient setting, and there are no standardized post-hospital discharge feeding guidelines. This study aims to describe post-neonatal intensive care unit (NICU) discharge growth trajectories of very preterm (<32 weeks gestational age (GA)) and moderately preterm (32–34 0/7 weeks GA) infants managed by community providers and to determine the association between post-discharge feeding type and growth Z-scores and z-score changes through 12 months corrected age (CA).
METHODS:
This retrospective cohort study included very preterm infants (n = 104) and moderately preterm infants (n = 109) born 2010–2014 and followed in community clinics for low-income, urban families. Infant home feeding and anthropometry were abstracted from medical records. Repeated measures analysis of variance calculated adjusted growth z-scores and z-score differences between 4 and 12 months CA. Linear regression models estimated associations between 4 months CA feeding type and 12 months CA anthropometry.
RESULTS:
Moderately preterm infants on nutrient-enriched vs. standard term feeds at 4 months CA had significantly lower length z-scores at NICU discharge that persisted to 12 months CA (–0.04 (0.13) vs. 0.37 (0.21), respectively, P = .03), with comparable length z-score increase for both groups between 4 and 12 months CA. Very preterm infants’ 4 months CA feeding type predicted 12 month CA body mass index z-scores (β=–0.66 (–1.28, –0.04)).
CONCLUSION:
Community providers may manage preterm infant post-NICU discharge feeding in the context of growth. Further research is needed to explore modifiable drivers of infant feeding and socio-environmental factors that influence preterm infant growth trajectories.
Keywords
Background
Preterm birth, defined as birth less than 37 weeks gestational age (GA) affects 1 out of every 10 infants in the U.S [1]. Preterm birth has been associated with long-term health morbidity, such as neurocognitive impairment and obesity [2–4]. Obesity in children with history of preterm birth is thought to be related to rapid growth in the first years of life and has implications for chronic disease later in adulthood [5–8]. Understanding and interpreting preterm infant growth patterns and nutritional needs is crucial to support optimal early childhood development for this high-risk population. Yet less is known about how primary care pediatric providers are managing preterm infant feeding and growing in the months after neonatal intensive care unit (NICU) discharge.
Many very preterm infants are considered growth-restricted by the time of hospital discharge [9]. The majority of these preterm infants are discharged home with nutrient-enriched dietary feeding plans with milk enriched with additional calories and protein to support enhanced growth and limit neurodevelopmental impairments [9–11]. These feeding plans are comprised of fortified expressed human breastmilk for breastfed infants and commercially available nutrient-enriched formula milk for formula-fed infants. Pediatric providers in the outpatient setting then assume the responsibility for managing and monitoring preterm infant diet and growth. However, there are currently no globally standardized feeding guidelines for preterm infants after hospital discharge, and the optimal duration to continue an infant’s enriched diet in the outpatient setting is not fully understood.
There is inconsistent evidence to support preterm infant increased weight gain and linear growth on nutrient-enriched feeds compared to standard term formula and/or breast milk after NICU discharge [12]. Inconsistency in study conclusions may be due to variability in randomized control trial sample sizes, populations, locations, duration of enrichment, duration of the trial, and feeding methods and frequency [10, 12–14]. Conflicting conclusions and variability in methodology present a challenge to primary care pediatric providers seeking evidence-based recommendations on preterm infant post-discharge nutrition and growth monitoring, especially for preterm infants on nutrient-enriched feeding regimens at hospital discharge who require individualized nutritional management [15]. It is unclear when primary care pediatric providers may be making adjustments to preterm infant home milk feeding type after NICU discharge from infant growth measures at ambulatory follow-up visits. Describing primary care pediatric provider management of preterm infant feeding and growth in the community setting will inform future research into early child development and potential modifiable risk factors for future overweight and obesity in preterm infants after NICU discharge.
This study aimed to (i) describe and compare home feeding types and growth (weight, length, and body mass index (BMI) z-scores) from 4 months to 12 months corrected age (CA) and (ii) examine the relationship between feeding type at 4 months CA and anthropometry at 12 months CA in a cohort of low-income, urban preterm infants. Study infants were all discharged from the NICU on nutrient-enriched feeding regimens and followed by board-certified primary care pediatric attending providers and pediatric trainees, including interns and residents. The study hypothesized that there would be significant differences in growth z-scores between infants continued on nutrient-enriched feeds vs. infants transitioned to standard term feeds by 4 months CA.
Methods
A single-center retrospective cohort study of a preterm infants≤34 0/7 weeks GA who were discharged on nutrient-enriched feeds from a New York City urban teaching hospital from 2010–2014 and followed in the hospital-affiliated community-based primary care clinics was conducted. Of the 1,773 preterm infants≤34 0/7 weeks GA discharged from the NICU from January 2010–December 2014, there were 279 infants (16%) discharged on nutrient-enriched feeds who followed in the hospital-affiliated primary care clinics (Fig. 1). Of these 279 infants, only 213 infants were included in the analytic sample due to having complete anthropometry documented through 12 months CA. Infants were excluded from the study if they were discharged from the hospital NICU on only human milk and/or standard full-term formula feeding regimens; had systematic diseases that affected weight gain and required outpatient management by cardiology, gastroenterology, and/or pulmonology specialists; or were lost to primary care follow-up prior to reaching 12 months CA. The hospital-affiliated primary care clinics only care for children with public insurance for low-income families (such as Medicaid) or the New York State Children’s Health Insurance Program plan for low-income children. As moderate and late preterm infants account for the majority of preterm births in the U.S. [16], the infants in this study were categorized as either very preterm if GA was < 32 weeks or as moderately preterm if GA was 32 to 34 0/7 weeks. Preterm infant categories were based on subgroups proposed by the World Health Organization (WHO) [17]; infants 34 0/7 weeks GA were included in the moderately preterm group as these infants are cared for and discharged from the hospital NICU. Infant CA was defined as the menstrual age plus chronological age.
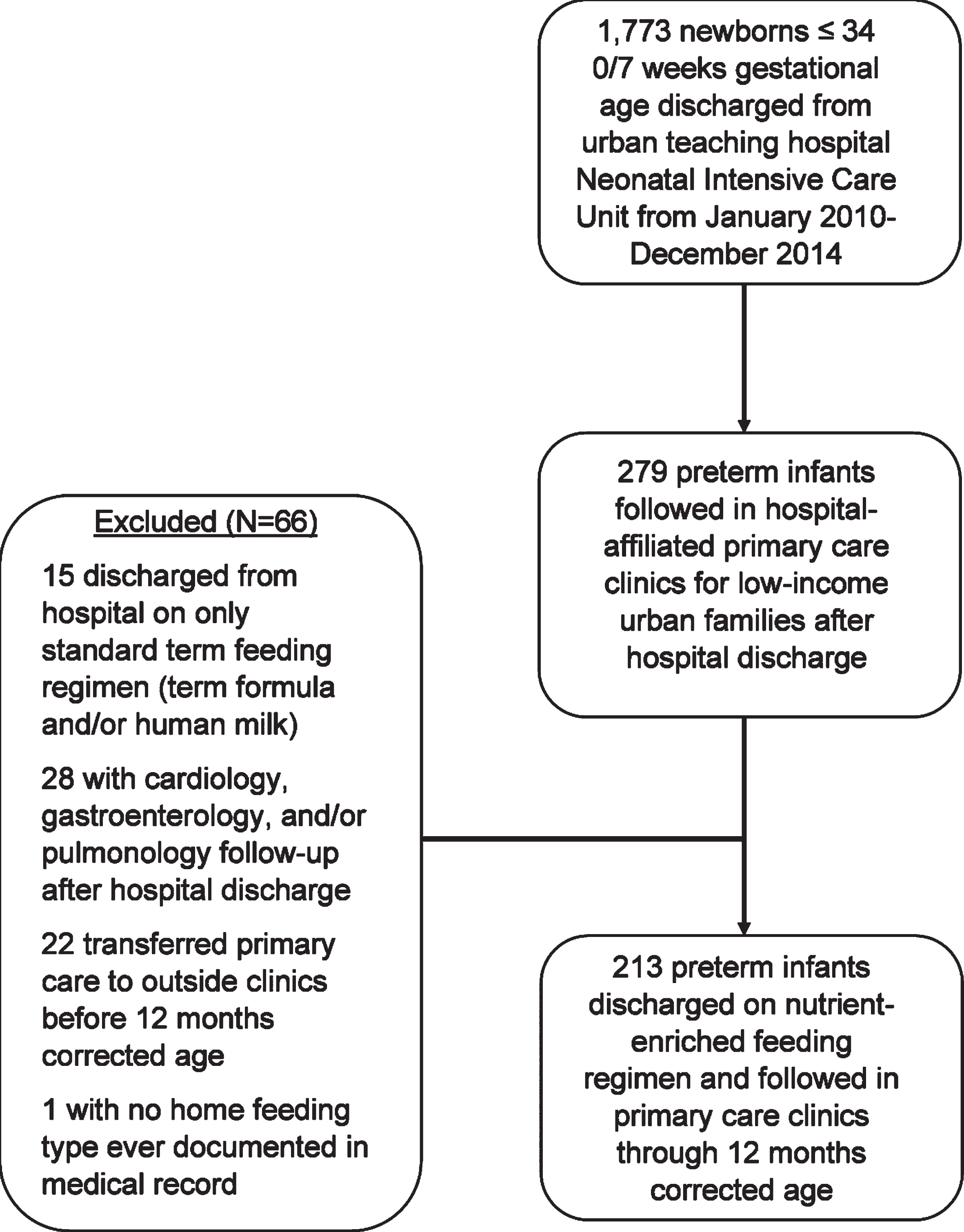
Study cohort selection flow diagram
Infants who were lost to follow-up were not significantly different by gestational age, birth weight, sex, or ethnicity compared to infants who continued to follow at the primary care clinics through 12 months CA.
The primary predictor was type of milk feeding at 4 months CA, as primary care providers are accustomed to timing of solid food introduction at 4–6 months for term infants [18]. Type of infant home feeding at 4 months CA was categorized as either Nutrient-enriched feeds, as a continuation of the NICU discharge feeding regimen, or exclusively Standard term feeds, representing a transition in the outpatient setting from the NICU discharge feeding regimen to a new feeding plan. Nutrient-enriched feeds were categorized as post-hospital discharge formula with a minimum caloric density of 22 kcal/oz only or post-hospital discharge formula and human breastmilk. Standard term feeds were categorized as full-term infant formula with caloric density of 20 kcal/oz only, full-term formula and human breastmilk, or human breastmilk only. Information on formula manufacturers, volume and frequency of formula consumption, daily breastfeeding frequency, time of introduction of solid food, and daily volume and frequency of solids and juice intake were not available for analysis due to high variability in pediatrician documentation.
The primary outcomes were weight-for-age z-score, length-for-age z-score, and BMI-for-age z-score at 12 months CA and the difference in z-scores between 4- and 12-months CA by gestational age group and type of home feeding at 4 months CA. Weight (in kilograms (kg)) and length (to the nearest 0.5 centimeter (cm)) of infants were measured according to standard hospital and clinic procedures. BMI was calculated from the documented length and weight in the medical chart at the corrected age of interest. Z-scores for birth and discharge weight and length were calculated using the validated sex-specific Fenton Preterm Growth Charts [19]. Birth BMI z-scores and small for gestational age (SGA) status at birth were calculated using the validated Olsen 2015 BMI curves for preterm infants [20]. All growth z-scores at 4 months CA and 12 months CA were calculated using the World Health Organization (WHO) Anthro 3.2.2 anthropometric calculator (January 2011), a software that facilitates application of the WHO Child Growth Standards in monitoring growth [21]. Use of WHO Growth Standards is recommended for all children less than 24 months by the U.S. Centers for Disease Control [22]. In addition to the application of the WHO Growth Standards for infant weight and length z-scores through 12 months CA [23], WHO Anthro-calculated BMI z-scores greater than +2.0 at 12 months CA were considered overweight.
Covariates included available demographic characteristics and birth and NICU-related factors. Available demographic characteristics included maternal age at delivery, parity, and mode of delivery, and self-reported ethnicity based on the U.S. Census Bureau categories of Hispanic or Latino or Not Hispanic or Latino. Birth and NICU-related factors included designation as small-for-gestational age at birth, NICU length of stay, corrected age at NICU discharge, and number of preterm infants receiving any human breastmilk at time of NICU discharge.
All data were abstracted from the electronic medical record by the research team based on provider documentation during infant clinical visits. The data abstraction process was partly informed by a medical record abstraction framework proposed by Zozus et al. [24]. The research team created a hypothesis, reviewed the literature to operationalize measures, created a codebook to guide abstraction methods, and conducted team abstraction reviews to share feedback on the accuracy of abstraction and make adjustments as needed.
Statistical analyses
Comparison of descriptive characteristics between very preterm and moderately preterm infants were conducted using Chi-square and Fisher exact tests for categorical variables and Student’s t tests and Wilcoxon Rank Sum tests for continuous variables. Given the unbalanced group sizes of infants on nutrient-enriched vs. standard term feeds at 4 months CA, least square (adjusted) means for growth z-scores at birth, hospital discharge, 4 months CA, and 12-months CA were estimated for infants by gestational age group and type of feeding at 4 months CA, adjusted for birth z-score parameter. Differences in adjusted means for growth z-scores between 4 and 12 months CA in infants who were transitioned to standard term feeds vs. infants who were maintained on nutrient-enriched feeds by 4 months CA in the very preterm group and in the moderately preterm group were compared for very preterm and moderately preterm infant groups. Difference in mean growth from 4 to 12 months CA between infants on nutrient-enriched feeds vs. standard term feeds at 4 months were quantified for the very preterm and moderately preterm infant groups using repeated measures analysis of variance (ANOVA), controlling for birth parameter z-score. Linear regression models estimated the relationship between type of feeding at 4 months CA and anthropometry at 12 months CA in the entire sample, adjusting for birth z-score parameter. SAS® software (Version 9.4, SAS Institute, Inc.) was used for all statistical analyses. Statistical tests were 2-sided and statistical significance was carried out at the P < .05 level.
Results
Of the 213 infants in the analytic sample, n = 104 were very preterm and n = 109 were moderately preterm. Characteristics of infants are available in Table 1. Very preterm infants had significantly lower birth weight (1127±370 g vs. 1994±432 g, respectively), longer hospital stay (61±28 days vs. 17±11 days, respectively), and an older corrected age at hospital discharge (37.1±2.7 vs. 35.6±1.3, respectively). There were no significant differences between the preterm infant groups by maternal age or mode of delivery, sex, Latino ethnicity, and small for gestational age at birth status. About 25% of very preterm infants, compared to 50% of moderately preterm infants, were also documented as receiving some human breastmilk at time of NICU discharge (P = .0002), and only 4% of very preterm infants and 6% of moderately preterm infants were still receiving any human breastmilk at 4 months CA (P = .80). Eighty-seven percent of very preterm infants and 72% of moderately preterm infants were continued on nutrient-enriched feeds at 4 months CA. By comparison, 13% of very preterm infants and 28% of moderately preterm infants were transitioned to standard term feeds by their primary pediatric provider by 4 months CA (P = .009). None of the very preterm infants and 21% of the moderately preterm infants were transitioned from nutrient-enriched feeds to standard term feeds between 4 months and 6 months CA. Five percent (n = 5) of very preterm infants and 8% (n = 11) of moderately preterm infants had BMI z-scores greater than +2.0 and were considered overweight at 12 months CA.
Characteristics of very preterm (<32 weeks GAa) and moderately preterm (32–34 weeks GA) infants (N = 213)
Characteristics of very preterm (<32 weeks GAa) and moderately preterm (32–34 weeks GA) infants (N = 213)
aGA, gestational age. bBMI, body mass index. cCA, corrected age. dContinous variables reported as mean±standard deviation.

Adjusted mean length z-scores through 12 months corrected age by feeding type at 4 months corrected age (CA). •— Very preterm + Nutrient-enriched feeding, ▴— Very preterm + Standard term feeding, ∘— Moderately preterm + Nutrient-enriched feeding, Δ— Moderately preterm + Standard term feeding, Adjusted mean length z-scores of infants through 12 months corrected age (CA) by type of home milk feeding at 4 months CA and by gestational age. Length z-scores are displayed as adjusted mean z-scores±standard error of means from repeated measures analysis of variance with an unstructured covariance matrix was performed, adjusted for birth length z-score. Moderately preterm infants on enriched feeds had persistently lower adjusted mean length z-scores at 4 and 12 months CA compared to moderately preterm infants on standard term feeds, although the difference was not statistically significant by 12 months CA.
The adjusted mean growth z-scores at birth, hospital discharge, 4 months CA, and 12 months CA for infant GA groups stratified by type of home feeding at 4 months CA are visualized in Figure 2 (length z-scores), Figure 3 (weight z-scores), and Figure 4 (BMI z-scores). Moderately preterm infants on nutrient-enriched feeds at 4 months CA had significantly lower adjusted mean weight [–0.26 (0.11) vs. 0.34 (0.18), P = .005] and length z-scores at 4 months CA compared to infants on standard term feeds [–0.35 (0.13) vs. 0.10 (0.21), P = .03 respectively], though there were no significant differences in raw arithmetic mean birth weight or length z-scores between the groups. Moderately preterm infants on nutrient-enriched vs. standard term feeds at 4 months CA had significantly lower length z-scores at NICU discharge that persisted to 12 months CA (–0.04 (0.13) vs. 0.37 (0.21), respectively, P = .03); both groups demonstrated comparable catch-up growth in length z-score increase between 4 and 12 months CA (+0.27 vs. +0.30, respectively, Table 3). There were no significant differences in the adjusted mean growth z-scores at 4 and 12 months CA of very preterm infants receiving nutrient-enriched vs. standard term feeds at 4 months CA.
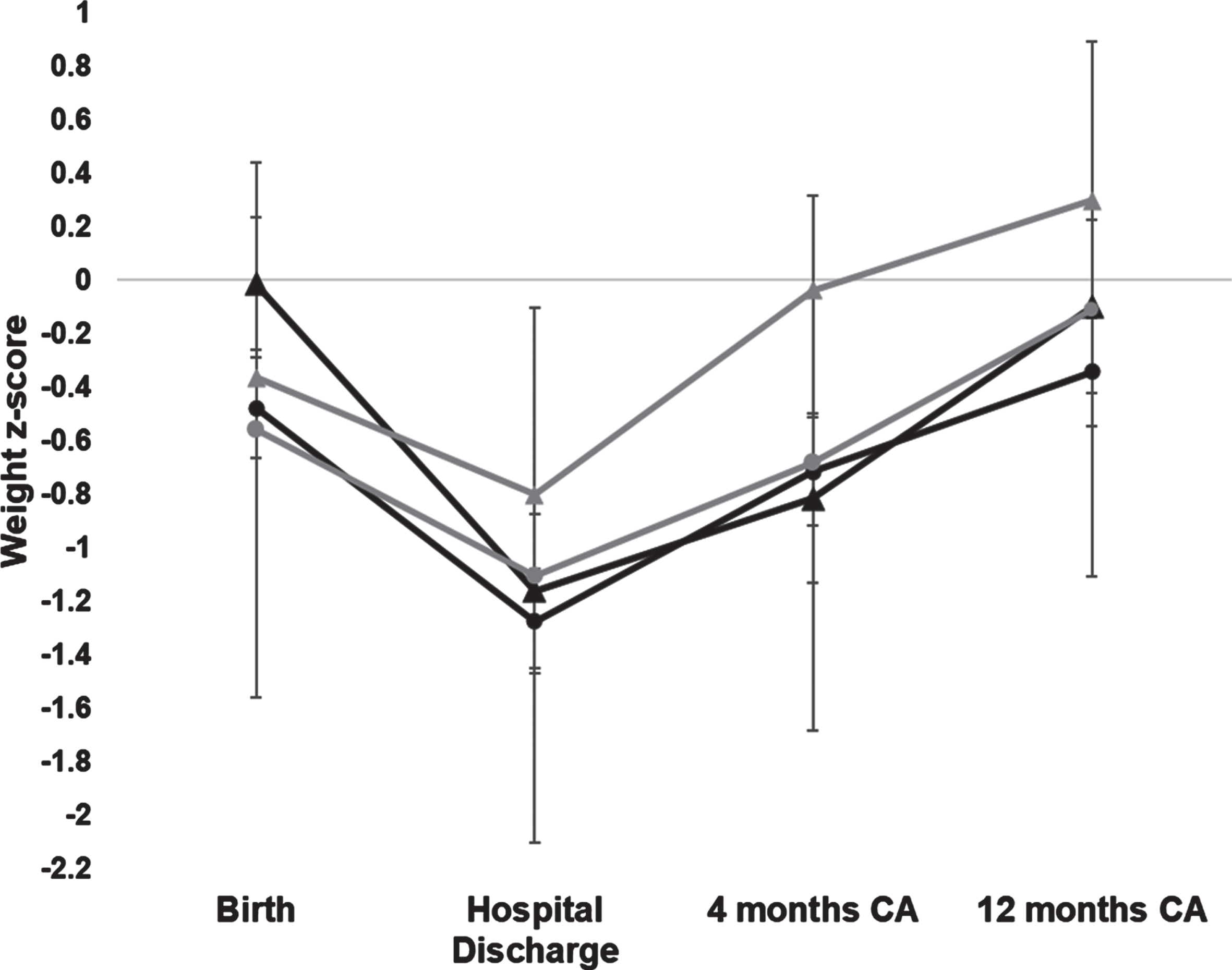
Adjusted mean weight z-scores through 12 months corrected age by feeding type at 4 months corrected age (CA). Adjusted mean weight z-scores of infants through 12 months corrected age (CA) by type of •— Very preterm + Nutrient-enriched feeding, ▴— Very preterm + Standard term feeding, ∘— Moderately preterm + Nutrient-enriched feeding, Δ— Moderately preterm + Standard term feeding, home milk feeding at 4 months CA and by gestational age. Weight z-scores are displayed as adjusted mean z-scores±standard error of means from repeated measures analysis of variance with an unstructured covariance matrix was performed, adjusted for birth weight z-score. Moderately preterm infants on nutrient-enriched feeds had significantly lower adjusted mean weight z-scores at 4 months CA compared to moderately preterm infants on standard term feeds.
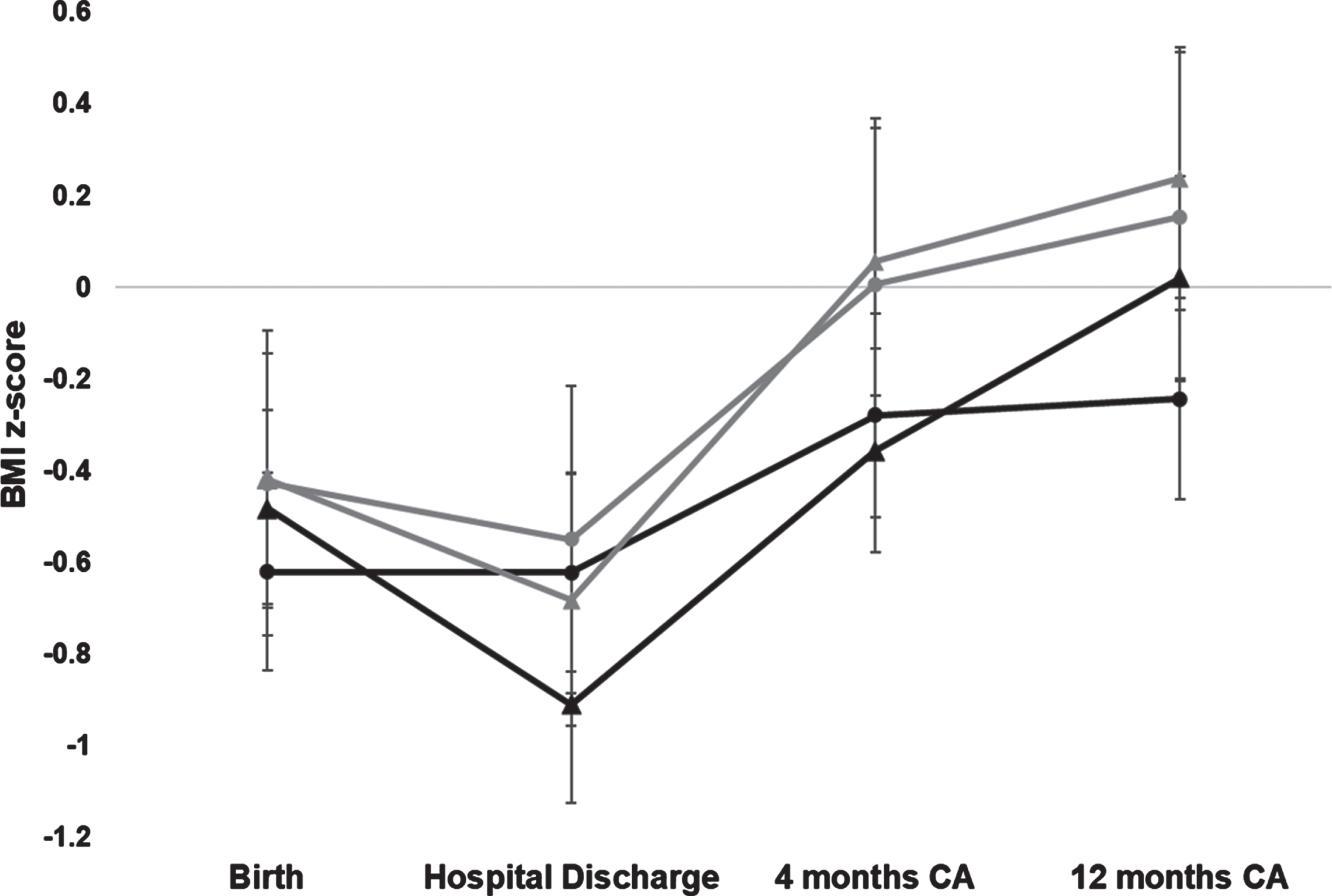
Adjusted mean body mass index z-scores through 12 months corrected age by feeding •— Very preterm + Nutrient-enriched feeding, ▴— Very preterm + Standard term feeding, ∘— Moderately preterm + Nutrient-enriched feeding, Δ— Moderately preterm + Standard term feeding, type at 4 months corrected age (CA). Adjusted mean body mass index (BMI) z-scores of infants through 12 months corrected age (CA) by type of home milk feeding at 4 months CA and by gestational age. BMI z-scores are displayed as adjusted mean z-scores±standard error of means from repeated measures analysis of variance with an unstructured covariance matrix was performed, adjusted for birth BMI z-score. There was no significant difference in adjusted mean BMI z-score between very preterm infants on nutrient-enriched feeds vs. standard term feeds. There was no significant difference in adjusted mean BMI z-score between moderately preterm infants on nutrient-enriched feeds vs. standard term feeds.
Very preterm infants transitioned to standard term feeds by 4 months CA had significantly higher adjusted change in weight z-score (Δweight=0.37, P < .0001) and change in length z-score (Δlength=0.97, P = .003) from 4 months CA to 12 months CA (Table 2). Similarly, very preterm infants maintained on nutrient-enriched feeds through 4 months CA had significantly higher adjusted change in weight (Δweight=0.37, P < .0001) and change in length (Δlength=0.49, P < .0001) z-scores from 4 months to 12 months CA. Moderately preterm infants transitioned to standard term feeds by 4 months CA had a significantly higher adjusted weight z-score at 12 months CA compared to 4 months CA (Δweight=0.33, P = .02) (Table 3). Moderately preterm infants maintained on nutrient-enriched feeds through 4 months CA had significantly higher adjusted change in weight (Δweight=0.58, P < .0001) and change in BMI z-scores at 12 months CA (ΔBMI=0.34, P = .03). There was no significant difference in the magnitude of the change in z-score for weight, length, or BMI z-score for either very preterm infants or moderately preterm infants when comparing infants transitioned to standard term feeds vs. maintained on nutrient-enriched feeds through 4 months CA.
Adjusteda growth Z-scores and growth Z-score difference from 4 months to 12 months corrected age (CAb) for very preterm infants, by feeding type
aRepeated measures analysis of variance (ANOVA) to test difference in least-square means, adjusted for birth z-score measure. bCA, corrected age. cSE, standard error. dBonferroni correction for multiple testing applied.
Adjusteda growth Z-scores and growth Z-score difference at 4 months vs. 12 months corrected age (CAb) for moderately preterm infants, by feeding type
aRepeated measures analysis of variance (ANOVA) to test difference in least-square means, adjusted for birth z-score measure. bCA, corrected age. cSE, standard error. dBonferroni correction for multiple testing applied.
Results of adjusted linear regression models estimating the association between type of home milk feeding and 12-month CA weight, length, and BMI z-scores are reported in Table 4 for very preterm infants and Table 5 for moderately preterm infants. Type of home feeding at 4 months CA significantly predicted 12-month CA BMI z-scores in very preterm infants (β=–0.66 (–1.28, 0.04), P = .03), adjusting for birth z-score parameter.
Association of type of home feeding at 4 months CAa with anthropometry at 12 months CA in very preterm infants, adjusted for birth Z-score parameter
aCA, corrected age. bValues reported as adjusted standardized β coefficient (95% confidence interval).*p < .05; **p < .01.
Association of type of home feeding at 4 months CAa with anthropometry at 12 months CA in moderately preterm infants, adjusted for birth Z-score parameter
aCA, corrected age. bValues reported as adjusted standardized β coefficient (95% confidence interval). *p < .05; **p < .01.
In this sample of low-income urban very preterm and moderately preterm infants in hospital-affiliated primary care clinics, the majority of infants were on nutrient-enriched feeds through at least 4 months CA. However, both very preterm infants and moderately preterm infants demonstrated significant weight z-score increases from 4 months CA to 12 months CA, irrespective of type of feeding at 4 months CA. Very preterm infants had no significant differences in adjusted weight, length, or BMI z-scores at 4 months CA or 12 months CA between nutrient-enriched and standard term feed groups. This suggests that primary care pediatricians may have considered additional factors beyond gestational age and infant growth measurement when managing preterm infant home feeding.
By contrast, moderately preterm infants maintained on nutrient-enriched feeds through at least 4 months CA had a persistently significantly lower adjusted length z-score from 4 months CA to 12 months CA compared to infants transitioned to standard term feeds at 4 months CA. Whether this significant difference in length z-scores is clinically meaningful remains a question for further research, given the continued global conversation on ideal curves to monitor linear growth of preterm infants after hospital discharge [19, 26]. While nutrient-enriched feeds have an increased amount of protein thought to contribute to greater linear growth [27], non-nutritional factors may also influence linear growth of preterm infants. This is especially pertinent given that moderately preterm infants on nutrient-enriched feeds at 4 months CA had no significant difference in adjusted weight z-score at 12 months compared to infants transitioned to standard term feeds at 4 months CA.
Type of feeding at 4 months CA significantly predicted 12 months CA mean BMI z-scores in very preterm infants when adjusting for birth z-score parameter. Further research quantifying preterm infant home feeding frequency and volume through at least 4 months CA will help provide pediatric primary care providers with a timeframe to re-evaluate infant home milk feeding and to consider ramifications on future growth.
There are unique challenges with the care of preterm infants, and the absence of standardized home feeding guidelines can increase difficulties faced by primary care pediatric providers in monitoring and managing preterm infant feeding and growth. A range in the awareness of breastfeeding guidelines for preterm infants was seen in a study of outpatient pediatricians in New York on challenges with preterm infant care after NICU discharge [28]. There was a decrease in breastfeeding rates after hospital discharge amongst mothers of both very preterm and moderately preterm infants. The results are consistent with those of a multiregional European study that found very preterm infants had a significantly lower probability of breastfeeding continuation if they received formula at discharge and their mothers were younger age and less educated [29]. Additionally, a study on breastfeeding cessation found that U.S. younger mothers and those with limited socioeconomic resources were more likely to stop breastfeeding within the first month after delivery [30]. Given that breastmilk is highly suggestive to reduce weight gain velocity and BMI in full-term infants [31], it is possible that continued breastfeeding in the study population may have decreased the weight z-scores seen at 12 months CA.
This study suggests an importance of supporting primary care pediatric providers’ efforts to educate families on the benefits of breastmilk for preterm infant growth after hospital discharge and to develop practice-based lactation support services targeting families of preterm infants [32], Forty-eight percent of community pediatricians caring for NICU graduates reported a lack of clinical experience with high-risk infants as an impedance to providing quality care to NICU graduates when surveyed in the Northeast U.S. [33]. Community pediatric providers can support families who may have difficulty understanding the preterm infants’ discharge feeding plans, especially when mixing of formula powder and milk or water on hospital discharge instructions differs from the instructions on the formula container or human milk fortifier packet [34, 35].
Pediatric primary care providers have many preterm infant growth charts, including the Fenton 2013 and the INTERGROWTH-21st Preterm Postnatal Growth Standard 2015, that can be used to monitor growth and guide nutritional management up to term or post-term through about 3–6 months CA [20, 36]. The growth monitoring tool selected by the pediatric primary care provider can depend on the provider’s preference and local norms, with ramifications for provider assessment on normal or abnormal preterm infant growth [26]. Use of birthweight-for-gestational age charts, constructed from cross-sectional birth size, to monitor growth over time may promote rapid growth to approximately match intra-uterine fetal growth trajectories or to exceed intra-uterine growth trajectories as catch-up growth. Goal weight gain of g/kg/day or reaching the 5th–10th percentile on the term infant growth chart to monitor preterm infant growth in the primary care setting may be limited by variability of periods of accelerated growth among different infants. Variability in birth weight, morbidity, sex, and feeding can contribute to differing interpretations of rapid weight gain and catch-up growth. Distinguishing rapid infant weight gain as catch-up growth in lean mass vs. fat mass and the cause and timing of either can be difficult to ascertain without costly body composition measurement tools. Preterm infant growth either matching an intra-uterine growth trajectory or exceeding an intra-uterine growth trajectory raises significant and separate implications for future development and potential child obesity risk [37, 38]. Lack of consensus on best methods to assess preterm infant growth in the primary care setting contributes to challenges comparing growth between infants when different methods are utilized.
Model instability from the small sample size of infants with elevated BMI z-score precluded an analysis of the association of post-discharge feeding type with overweight status. Yet the presence of preterm infants with elevated BMI z-score raises implications for early obesity risk in a vulnerable population. Lower-income communities in the U.S. in general have greater prevalence of overweight and obesity among both adults and children [39, 40]. The literature suggests there are unique postnatal maternal-, household-, and socio-structural-level factors experienced by low-income communities that may contribute to specific preterm infants developing an elevated BMI z-score [41–43]. Primary care pediatric providers should give consideration to risk for overweight and obesity as part of infant growth and milk feeding type management strategies [44].
There was no significant difference in the magnitude of the change in z-score for weight, length, or BMI between 4 months CA and 12 months CA for either very preterm infants or moderately preterm infants. This suggests the need for additional research with a larger sample of very preterm and moderately preterm infants to improve the power to detect a significant difference in 12 month adjusted mean growth z-scores. There are also likely additional factors, unmeasured in this study, that have previously been associated with preterm infant growth after hospital discharge, such as maternal factors (pre-pregnancy BMI, education, and smoking), household attitudes and beliefs around infant feeding, milk feeding volume and frequency, and preterm activity and sleep [27, 46]. Mothers of preterm infants have reported experiencing anxiety and stress around identification of infant hunger and satiety cues, variability in infant feeding effectiveness, management of feeding volumes, and knowing how and when to advance feeds at home [47, 48].
This study had several limitations. This was a single center, observational study that utilized a retrospective cohort. A causal relationship between type of home feeding at 4 months CA and 4 and 12 months CA growth measures could not be determined. While collecting data in one health care system was accessible and cost-effective, the results may not be generalizable across primary care sites and clinics. Type of home feeding and infant anthropometry were obtained from medical chart review rather than objectively collected or verified. Nutritional data could have been subject to recall bias or social desirability bias by caregivers wishing to appear to be following the primary care pediatricians’ nutrition management instructions. Reliance on secondary data may also have increased susceptibility to recall bias by pediatricians to accurately record the infant home feeding at the follow-up visits.
Inconsistencies in primary care provider documentation of volume and frequency of home milk feeds and introduction and frequency of intake of complementary foods and beverages other than milk before 12 months CA precluded the use of this information in the analyses. These home feeding factors have also been shown to influence infant growth and may have contributed to the anthropometry findings at 12 months CA. Additionally, early growth in formula-fed preterm infants may be associated with specific composition of nutrient-enriched formula with regards to ratios of energy, protein, and mineral content [49]. Although caloric density of feeding was evaluated, neither the brand name of formula used by the infants’ families nor patterns of breast milk fortification nor exact formula composition information were consistently documented and could not be used in analyses. Study limitations also included inconsistent information on maternal characteristics that have been associated with infant weight and growth as several infants were transferred to the urban teaching hospital NICU for management after their births at outside institutions. There may have been other unmeasured socio-environmental factors that had residual confounding effects on both infant feeding and growth, such as food and housing hardship experienced by the families and neighborhood activity spaces. This study used BMI z-score to identify infants at risk for obesity as per previous literature [50], yet there is not yet an international consensus on definitions of overweight and obesity in infants < 24 months and the U.S. Centers for Disease Control define cut-offs for obesity in children > 24 months of age [51]. In spite of these limitations, the study’s strengths included a sample of infants of largely Latino ethnicity from a low-income urban background, a population largely underrepresented in research. Additionally, a follow-up period for growth measures data extending to 12 months CA allowed us to capture the important time period between post-hospital discharge and late infancy.
This study contributes to the literature by characterizing the primary care pediatrician-managed home milk feeding and growth of low-income urban very preterm and moderately preterm infants in the community in the months after hospital discharge. Future research aims to collect longitudinal quantitative and qualitative data on preterm infant home feeding frequencies and volumes, introduction of complementary foods, participation in the government nutrition assistance programs, and caregiver beliefs around preterm infant feeding and growing. Describing and comparing early infant and childhood growth patterns of preterm infants with different types of home milk feeding patterns has implications for primary care pediatric provider management of preterm infants after hospital discharge.
Conclusions
A lack of consensus on post-hospital discharge feeding guidance can present a challenge to the primary care pediatric provider caring for preterm infants in the community setting. The study demonstrated that moderately preterm infants on enriched feeds had persistently lower length z-score at 4 and 12 months CA compared to moderately preterm infants on standard term feeds. Type of home feeding at 4 months CA predicted BMI z-score at 12 months CA for very preterm infants. Future work is needed to longitudinally investigate home milk feeding volume and frequency and to determine household and clinical factors that may contribute to primary care pediatric provider care of preterm infants to optimize their early development.
Footnotes
Acknowledgments
I would like to thank Dr. Sudha Kashyap for her guidance and assistance with the project and Drs. Robert Whittington and Melissa Stockwell for their valuable comments on previous drafts of this manuscript.
Financial disclosure statement
This publication was supported by a Health Resources and Services Administration Ruth L. Kirchstein National Research Service Award Institutional Research Training Grant [T32HP10260] and the National Center for Advancing Translational Sciences, National Institutes of Health [UL1TR001873]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the HRSA of the NIH.
Human research statement
The Institutional Review Board for Human Investigations at the Columbia University Irving Medical Center approved this study protocol with waiver of informed consent (Protocol AAAM8602). All research involving human subjects was conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration of 1975.
Data accessibility
The dataset used during the current study is available from the corresponding author upon reasonable request.