
Abstract
BACKGROUND:
Hemorrhage anticipation and management has shifted significantly over the past decade due to evolution of data surrounding management of obstetric hemorrhage. Limited data exists which describe the practical use and clinical application of hemorrhage management. Our goal was to identify obstetric hemorrhage management patterns in a cohort of practicing Maternal Fetal Medicine physicians.
METHODS:
We administered a survey to Maternal Fetal Medicine (MFM) fellows and faculty that addressed the management of hemorrhage including risk assessment, uterotonic use, antifibrinolytic use, cell saver use, and abnormal placentation management. An email was sent out regarding the survey to a listserv of all Maternal Fetal Medicine fellow program coordinators to disseminate to their faculty and fellows. Eighty responses were obtained.
RESULTS:
A total of 78 surveys were analyzed. Participants preferred methylergonovine as a first line agent (n = 57; 73%, n = 62; 80%). Most participants would consider using cell salvage when also activating MTP (28, 48%) or during scheduled deliveries who are high risk of hemorrhage (40, 69%). Approximately a third of providers would use TXA (tranexamic acid) prophylactically (n = 21; 28%). Only 26% of MFM fellows felt comfortable performing cesarean hysterectomy without Gynecologic Oncology.
CONCLUSION:
In comparison to prior reports, TXA use has increased substantially. Further, when looking at the management of abnormal placentation, the use of magnetic resonance imaging and embolization have both increased. Possibly due to the rise in centers of excellence for treatment of accreta spectrum disorders, Maternal Fetal Medicine fellows still feel largely unprepared to perform a cesarean hysterectomy without Gynecologic Oncology.
Keywords
Introduction
Obstetric hemorrhage remains a leading cause of maternal morbidity and mortality in the United States [1]. Importantly, hemorrhage anticipation and management has shifted significantly over the past decade due to evolution of data surrounding management of obstetric hemorrhage. Limited data exists which describe the practical use and clinical application of hemorrhage management protocols [2] and existing studies are outdated by recent advancements. Examples include addition of hemorrhage risk prediction tools for identifying high risk patients, development of standardized hemorrhage management protocols, and the use of tranexamic acid (TXA) in obstetric hemorrhage [3–7].
Further, abnormal placentation and its management continues to evolve. Most of the literature surrounding abnormal placentation is limited to case reports, case series and retrospective cohort studies. Thus, there is large variability in management. Ahmadzia, et al. performed a survey study in 2012 which highlighted a wide practice variation on management of obstetric hemorrhage among MFM Fellows [8].
Given the continued growth in the field of hemorrhage management, the goal of this study aims to identify attitudes and practices surrounding obstetric hemorrhage through sampling current Maternal Fetal Medicine (MFM) fellows and faculty working at tertiary care centers across the United States. This includes hemorrhage risk stratification, uterotonic use, cell salvage use, and abnormal placentation.
Methods
This was a cross-sectional survey created to address modern obstetric hemorrhage management. The survey was developed and by the research investigators of this study and is included in Appendix A. Our survey was developed based on a prior survey administered in 2012 with a new emphasis placed on modern aspects of hemorrhage management that have changed since the initial study [8]. Permission was obtained from the George Washington University Institutional Review Board and the survey was considered exempt IRB#NCR191767 as it presented no risk to those completing the survey. Study data were collected and managed using REDCap electronic data capture tools. An email was sent out regarding the survey to a listserv of all MFM fellow program coordinators to disseminate to their faculty and fellows. The survey was sent out four times through the listserv between 2020–2021. The survey was then also sent out via Society of Maternal-Fetal Medicine (SMFM) to their listserv as a Research Survey of Interest on Nov 10th, 2020.
Survey data collected included basic demographic information and hemorrhage management practices in the following domains: uterotonic use, antifibrinolytic agents (i.e. TXA), cell salvage use in obstetrics, and abnormal placentation management. Participants were prompted on the online platform to answer questions based on level of training (faculty versus fellow) and prior responses. After an initial 33 responses, additional questions regarding level of maternal care, number of labor and delivery beds, and subspecialist availability were added to give more insights on hospital characteristics. Statistical analysis of variables was performed with Microsoft Excel, with a p≤0.05 as considered significant.
Results
A total of 80 surveys were submitted in response to our listserv query and 73 contained complete responses (91%). One survey was uninterpretable due to missing data and one survey did not report a key demographic indicator (faculty or fellow) and thus these two surveys were excluded from the final analysis. The five other incomplete surveys contained key information and thus were appropriate for inclusion, making our final sample size 78.
All surveys were completed between March and December 2020. Seventy percent of respondents were MFM faculty. Most respondents were from Level IV centers (n = 28; 62%) and most centers had Gynecologic Oncology, Interventional Radiology, and Urology on staff (all >95%). Institutional protocols related to obstetric hemorrhage or massive transfusion protocol were nearly universal (n = 77, 99%). Sixty percent of participants (n = 47) reported that their hospital utilized an obstetric hemorrhage risk prediction tool upon admission for delivery. Of those who reported use of a hemorrhage risk prediction tool, sixty-eight percent (n = 32) reported reassessment of hemorrhage risk in the intrapartum time period. The most reported risk prediction tool was AWOHHN (n = 17; 36%) and the CMQCC (n = 9; 19%). Three respondents reported having their unique hemorrhage risk tool, and the rest did not know (n = 12; 26%) or left the type of risk prediction tool blank (n = 6; 13%). Sixty percent of respondents reported administration of the scoring by a nurse (n = 28). The other responses listed the provider or resident (n = 15; 32%), or both the provider and nurse (n = 3; 6%).
We then evaluated preference of uterotonics administration in an ongoing hemorrhage (Figs. 1 and 2). When assessing the order of medication management preferences, participants preferred methylergonovine as a first line agent for both vaginal and cesarean deliveries following standard administration of oxytocin administration (n = 57;73%, n = 62;80%). Second choice was most often carboprost (n = 35;45%, n = 42;55%). TXA was more commonly used as a third line agent in cesarean delivery, whereas TXA and misoprostol were almost equally used as a third line agent in vaginal delivery.
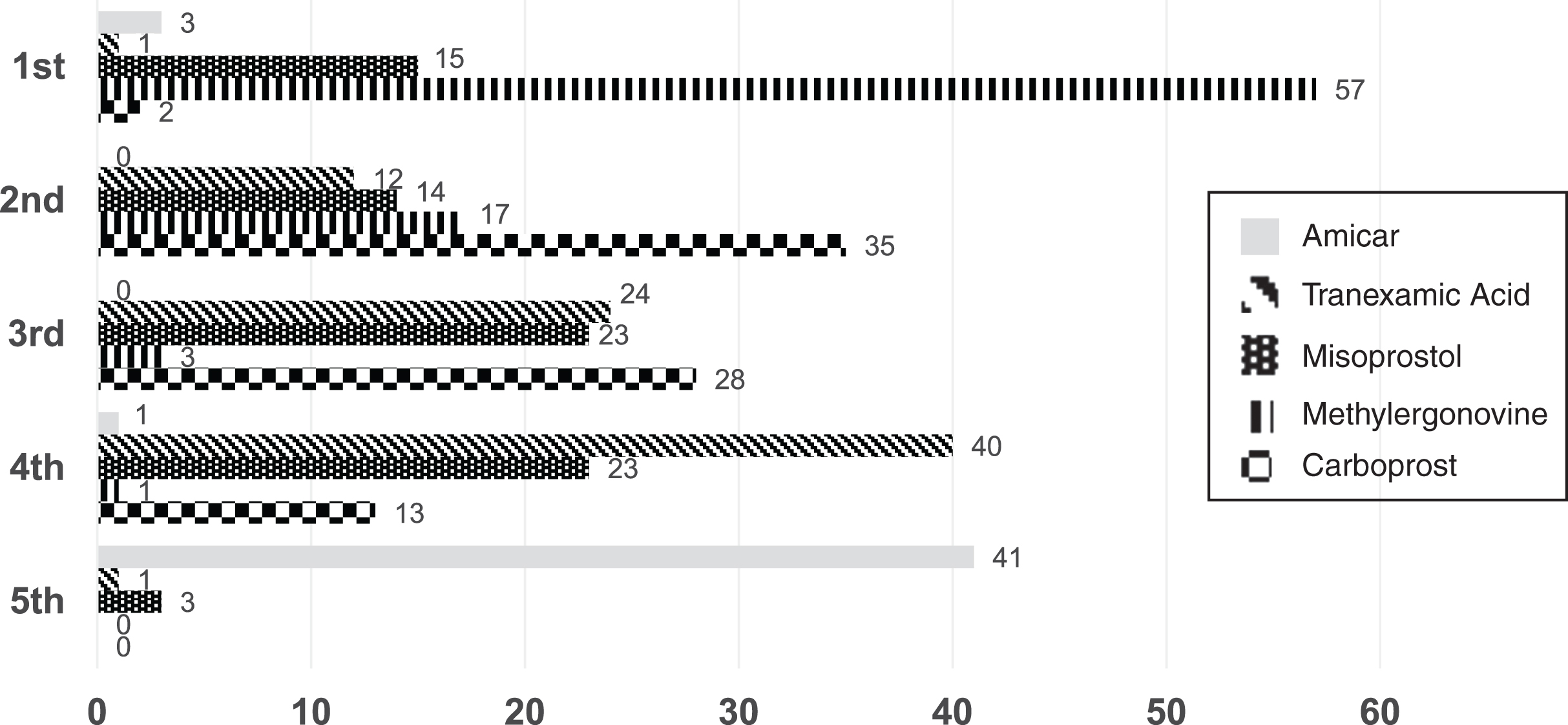
Vaginal delivery medication preferences.
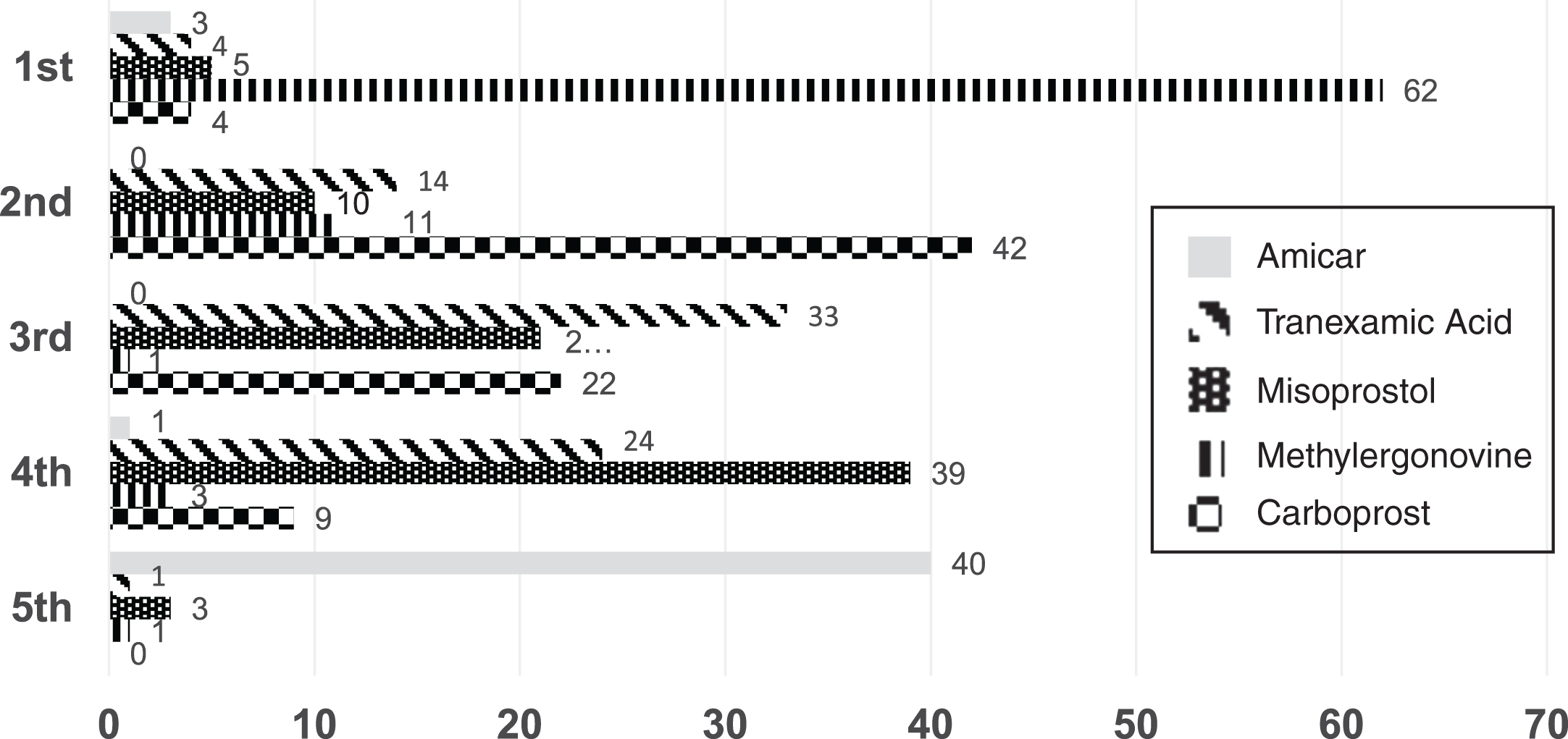
Cesarean delivery medication preferences.
Antifibrinolytic agents were used widely amongst those who responded to the survey with the most reported agent as TXA (n = 75; 96%). The most commonly reported dose was 1 gram intravenous at 1 mL/min (n = 67, 89.3%). However, there was more variability noted in responses to re-dosing—only 43 (58.1%) of respondents said they would use multiple doses of TXA, and of those, most would re-dose after 30 minutes (n = 24; 55.8%). Approximately a third of providers endorsed they would use TXA prophylactically (n = 21; 28%).
Seventy-six percent of respondents reported access to cell salvage during an obstetric hemorrhage. However, when asked regarding quickness of access, only 8 (13.6%) physicians stated that they had it available to them in less than 10 minutes. During a cesarean hemorrhage, 26% of providers responded that they would often (n = 3) or sometimes (n = 12) use cell salvage. The majority of participants would never consider using cell salvage during vaginal obstetric hemorrhage (n = 39, 67%). However, some participants reported that they would consider use of cell salvage during cesarean obstetric hemorrhage (sometimes n = 2, 3%; rarely n = 17, 30%). Most participants would consider using cell salvage when also activating MTP (n = 28, 48.3%) or utilizing it during scheduled deliveries who are identified as high risk for hemorrhage (n = 40, 69%).
Demographic information
*Data are expressed in number (%) **these demographics were collected halfway through data collection; thus are displayed separately.
Anticipated peripartum hysterectomy management in cases with suspected abnormal placentation (n = 77)
Regarding abnormal placentation, most of these respondents were MFM faculty members. Planned cesarean hysterectomy for abnormal placentation most often was scheduled in the main operating room and not on labor and delivery (52, 68%). In most cases, an antifibrinolytic agent was used when performing a peripartum hysterectomy (64, 83%). The most used preoperative consultation services were Gynecologic Oncology and Anesthesia. Femoral balloons were uncommonly placed, as well as Interventional Radiology placement of guide wires prior to delivery (Table 3).
Anticipated peripartum hysterectomy management in cases with suspected abnormal placentation
Surgeon role and comfort level was also assessed amongst MFM fellows who responded to the survey (n = 23). In residency, the average peripartum hysterectomy involvement was quoted as 4.1 (standard deviation 3.6). Only 42% of fellows responded that they were primary surgeon in at least half of the cesarean hysterectomies for abnormal placentation. When asked if they felt prepared to perform a hysterectomy as an attending, about half felt prepared to perform one with Gynecologic Oncology available. Only approximately 26% felt comfortable performing a cesarean hysterectomy independently. In contrast, a little over half of MFM faculty felt comfortable without Gynecologic Oncology as backup.
This survey attempts to capture and describe the variety of hemorrhage practice amongst MFM providers. Over half of respondent’s institutions reported they had a hemorrhage risk assessment protocol. The majority preferred methylergonovine use as a second line treatment (following oxytocin) no matter the mode of delivery. Most participants would never consider using cell salvage during vaginal obstetric hemorrhage. However, most participants would consider using cell salvage when activating massive transfusion protocol (n = 28, 48.3%) or utilizing it during scheduled deliveries who are identified as high risk for hemorrhage.
Surgeon role and comfort level was also assessed amongst MFM fellows who responded to the survey (n = 23). Only approximately 26% felt comfortable performing a cesarean hysterectomy independently. In contrast, a little over half of MFM faculty felt comfortable without Gynecologic Oncology as backup.
This study was compared to a prior study completed in 2012 by one of the authors of this study. In comparison to the 2012 study where no participants had used an antifibrinolytic in the setting of a postpartum hemorrhage, TXA use has increased substantially, with wide adoption of the agent as an adjunctive treatment in the management of obstetric hemorrhage [9]. Prophylactic use of TXA was also demonstrated within this survey, with 28% of respondents stating they would consider using TXA prophylactically in an obstetric hemorrhage. When looking at trends in the management of abnormal placentation, there were some key differences noted between this most recent survey and the one performed of MFM fellows in 2013 [2, 8]. Both have similar preoperative consultation trends. The use of MRI has increased, as well as the use of embolization.
There have been a multitude of advances in obstetric hemorrhage over the last decade. This survey attempts to capture and describe the variety of hemorrhage practice amongst MFM providers. Over half of respondent’s institutions reported they had a hemorrhage risk assessment protocol. This likely represents a trend towards overall standardization of hemorrhage management at level IV facilities. This change in management can likely be attributed to recent publications that demonstrate possible improvement in management of postpartum hemorrhage with standardization including decreased blood product use and decreased incidence of disseminated intravascular coagulopathy [10]. Further, the release of national safety bundles for obstetric hemorrhage has demonstrated a decrease in maternal morbidity and mortality [3, 11]. Although implementation of risk stratification is an important first step in early detection and response to postpartum hemorrhage, there are still many variations in practice management that remain as demonstrated by the responses to the remainder of the survey.
In those who responded, the majority preferred methylergonovine use as a second line treatment no matter the mode of delivery. This may reflect availability at the institutions surveyed or could be related to a more favorable side effect profile when compared to other common side effects of other uterotonics. The preference of methylergonovine as predominant second line agent is analogous to the pattern demonstrated by a prior study [12].
Prophylactic use of TXA was also demonstrated within this survey, with 28% of respondents stating they would consider using TXA prophylactically in an obstetric hemorrhage. This change in practice is likely accounted for by the now widely accepted results of the WOMAN trial, and endorsement of TXA use by ACOG [10]. In contrast, the TRAAP study in France, a randomized control trial of approximately 3800 women completed in 2017 did not demonstrate any change in the rate of postpartum hemorrhage > 500 ml after a vaginal delivery with use of both prophylactic oxytocin and TXA within 2 minutes of delivery. However, it did demonstrate a decrease in the rate of clinically significant hemorrhage and the use of additional uterotonic agents for bleeding [6]. The Cochrane review from 2018 also supports TXA use by demonstrating that it reduces the risk of maternal mortality [4]. Further, there are many other studies summarized in a paper by Ahmadzia et al which demonstrate decreased blood loss associated with use of TXA [9].
Cell salvage and autotransfusion is a new therapy in the management of obstetric hemorrhage. Due to barriers in access and education, cell salvage in obstetrics has not yet been widely adopted in the United States [13, 14]. It is endorsed in the 2017 ACOG practice bulletin and the placenta accreta spectrum practice guidelines [15]. Our data demonstrate that cell salvage is most utilized during cesarean hemorrhage. However, emerging data demonstrate preliminary safety data for autotransfusion of vaginally shed blood [16, 17]. Despite this, our data demonstrate that the majority of participants would never use cell salvage in the case of vaginal obstetric hemorrhage. However, we did demonstrate some receptiveness to its potential use within providers during a vaginal obstetric hemorrhage.
When looking at the management of abnormal placentation, this shift towards increased use of MRI and embolization may be attributed to increased recognition and creation of centers of excellence for treatment of accreta spectrum disorders. These criteria were established in 2015, and likely paved the way for further interdisciplinary management of these disorders, and thus further use of MRI and embolization when compared to the prior study. Further, there was a 2018 systematic review that demonstrated the accuracy of diagnosis with MRI for accreta, percreta, increta as 94, 100, and 87 percent, respectively [18]. However, these outcomes are largely dependent on the expertise of the physician reading the study.
Surgeon role and comfort level data obtained was low within this study, however it continues to demonstrate that MFM fellows feel largely unprepared to perform a cesarean hysterectomy without Gynecologic Oncology backup. This re-emphasizes the need for continued interdisciplinary care, or even further specialization for treatment of placenta accreta spectrum disorders post fellowship training. This lack of preparedness may also be accounted for by increased availability of these centers of excellence, thus leaving fewer of these procedures with larger trainee involvement.
This study highlights a lack of acceptance of cell saver use among providers. It demonstrates a need for further research into understanding the barriers and practical use of cell salvage in obstetrics. This study also represented a small cohort of MFM fellows (n = 23), but there was a notable variety in training with regard to accreta spectrum disorders. Larger scale studies in this area may help highlight an educational gap amongst fellowship programs. Also, this study would benefit replication on a much larger scale to form a deeper understanding of practice patterns related to hemorrhage amongst all general obstetricians.
There were some limitations in the generalizability of these outcomes. The survey respondents were mostly MFM faculty at Level IV facilities. Further, there is likely a large selection bias in those institutions who responded—given our mode of reaching out through the SMFM listserv are far more likely to be institutions to participate and therefore reading more recent literature. Given that the survey was distributed broadly amongst program coordinators to fellows and faculty, we also do not have a way of calculating the response rate, nor verifying how many providers came from each institution. If many providers responded from one institution, this could have skewed our results unknowingly. Further, we recognize that at many institutions the generalists are often those initiating initial hemorrhage management, and that those providers are not captured by this study.
Conclusions
Overall, this study served to describe the large variation in practice throughout the country regarding postpartum hemorrhage and placenta accreta spectrum disorders. We found that most facilities have adopted recent obstetric hemorrhage guidelines, utilizing hemorrhage risk prediction tools and TXA in the management of obstetric hemorrhage. Our study highlights the most common management strategies for obstetric hemorrhage in Level IV maternity centers.