
Abstract
BACKGROUND:
Late preterm (LPT) infants are increasingly treated for hypoxic-ischemic encephalopathy (HIE). However, neurodevelopmental differences of LPT infants may independently influence the neurologic exam and confound care.
METHODS:
Perinatal and outcome characteristics were extracted along with the worst autonomic and state/neuromuscular/reflex Sarnat components in a cross-section of infants with moderate/severe HIE. Infants were classified as late preterm (LPT, 34–36 weeks) or term (>36 weeks).
RESULTS:
250 infants were identified, 55 were late preterm. LPT infants had lower mean gestational age and birthweight and greater length of stay (LOS). LPT infants had higher median scores for the Moro and respiratory autonomic components, but no difference in total score.
CONCLUSIONS:
LPT infants had increased LOS, worse Moro reflex, and respiratory status, but no clinically or statistically significant differences in total Sarnat scores. Although it is important to note the impact of immaturity on the exam, it is unlikely to independently alter management.
Keywords
Introduction
Neonatal encephalopathy is a condition with variable clinical expression including encephalopathy, hypotonia, apnea, seizures, and death [1, 2]. Hypoxic ischemia in the perinatal period is the most commonly attributed cause, but genetic or metabolic causes are identified in some cases [3]. Estimates for the incidence of neonatal encephalopathy vary, although are generally estimated to fall between 1.5 and 9 per 1000 live births in upper income countries [4–6]. The incidence is markedly higher in low- and middle-income countries. Early identification of infants at risk for neonatal encephalopathy is an essential component of a neuroprotection strategy and shortens the time to the primary intervention, therapeutic hypothermia (TH), which remains the only widely available treatment to reduce death or severe neurodevelopmental disability [7].
The benefits of therapeutic hypothermia were demonstrated over a series of randomized trials conducted in the United States [8], the United Kingdom [9], Europe [10, 11], and other multinational settings [12]. Like most randomized trials, inclusion and exclusion criteria were strict: limiting enrollment to infants born after 36 completed weeks of gestation and with moderate or severe encephalopathy. Practices have drifted since the publication of trial results and infants of lower gestational ages and with milder degrees of encephalopathy are now routinely cooled at some centers [13–16].
The decision to initiate TH is based on the presence of risk factors (cord blood acidosis, low Apgar scores, need for resuscitation) and evidence of moderate or severe encephalopathy, typically diagnosed using the modified Sarnat exam [17, 18]. For purposes of assessing encephalopathy in the setting of HIE, the total Sarnat score is typically calculated as the sum of the most severe score of the autonomic components and the six state, neuromuscular, and reflex components. Late preterm infants (gestational age 34–36 weeks) are screened for encephalopathy and undergo therapeutic hypothermia following the same approach as term-born peers at many centers [14]. However, differences in neuromuscular maturity in late preterm infants may independently influence the Sarnat exam and cause a falsely high number of late preterm infants to undergo cooling. In this project, the goal was to examine the differences between late preterm and term infants with HIE to determine if neurodevelopmental differences due to gestational age systematically influenced the Sarnat score and, subsequently, determined which infants underwent TH.
Methods
Cohort development
In this retrospective cross-sectional study, data was collected for all neonates who were admitted between 1 January 2015 and 31 December 2021, were diagnosed with moderate or severe encephalopathy, and underwent therapeutic hypothermia in the Level IV NICU of St. Louis Children’s Hospital, serving urban, suburban, and rural populations predominantly in Missouri, Illinois, and Arkansas. Inclusion criteria were gestational age (GA) of 34 completed weeks or greater, moderate or severe encephalopathy, treatment with therapeutic hypothermia, and no known congenital or genetic anomalies. Although institutional guidelines suggest TH should be considered primarily for infants ≥35 completed weeks of gestation, infants born at 34 weeks were included in the study both to encompass the full definition of late prematurity (34–36 weeks) and to capture eligible infants treated outside of the guideline recommendations. Gestational age was derived by best obstetrical estimate most often based on last menstrual period (LMP), but in some cases, ultrasound estimation was used instead (1st, 2nd, and rarely 3rd trimester).
Standard clinical practice
During the entire study period, the standard clinical practice was to perform screening encephalopathy exams for all infants with a cord blood gas pH ≤7.10 and or base deficit ≥12 mmol/L starting 60 minutes after birth. Exams were repeatedly hourly until either a) moderate or severe encephalopathy was identified (at which point TH was initiated), b) the exam was normal on two sequential exams, or c) the infant was older than 6 hours. Moderate encephalopathy was defined as the presence of moderate abnormalities in at least 3 of the Sarnat components. Severe encephalopathy was defined as the presence of severe abnormalities in at least 3 of the Sarnat components, consistent with NICHD NRN trial definitions [8].
Infants were treated with therapeutic hypothermia if they were less than 6 hours old and had at least one of the following: umbilical cord pH ≤7.10, base deficit ≥12, or 10-minute Apgar score ≤5, or need for prolonged resuscitation (defined as PPV and/or chest compressions for more than 10 minutes) in addition to having moderate/severe encephalopathy on exam. Infants were cooled to 33.5°C for 72 hours and slowly rewarmed to 36.5°C over an additional 24 hours using a servo-controlled water blanket (CritiCool, Belmont Medical Technologies, Billerica, MA). After TH was initiated, infants received sedation for comfort and to reduce shivering. Morphine was used as first line sedation for infants born 2015–2020, dexmedetomidine for infants born 2020 and later. All infants underwent full montage video EEG for at least 24 hours after TH start, extended in the case of seizures or severe background abnormalities, and at least one MRI performed on day of life 4 or 5.
Clinical data collection
A chart review of the electronic medical record was performed for all infants meeting inclusion criteria. Data collection included sex, birth weight (BW), race, gestational age at birth, 5- and 10-minute Apgar scores, lowest umbilical cord blood gas pH, known sentinel events [19] (defined as umbilical cord mishap, abruption, shoulder dystocia, maternal hemorrhage, trauma, cardiopulmonary arrest, and/or seizures), electrographically-confirmed seizures, hospital length of stay (LOS), sedation and/or anti-epileptic medication administration, and mortality. Infants were then grouped into late preterm (34–36 week GA) and term (>36 week GA) cohorts, with the latter serving as the comparison group.
Encephalopathy exam data
During the study period, all screening neurologic exams were recorded in the electronic medical record using a structured tool (locally referred to as the Neonatal Encephalopathy Assessment Tool or NEAT) based on the modified Sarnat exam, allowing an element-by-element record of each assessment. Component scores of the most severe exam in the first six hours of life (typically the final exam before TH initiation) were extracted and assigned point values (normal = 0, mild = 1, moderate = 2, and severe = 3, Table 1).
Sarnat exam scoring system
Sarnat exam scoring system
Univariate comparison between groups were made using the Mann-Whitney U-test or Fisher’s Exact test, where appropriate, and considered significant where p < 0.05. All statistical testing was performed using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics approval
The study protocol was reviewed and approved by the Human Research Protection Office (IRB) at Washington University under a wavier of informed consent pursuant to 45 CFR §164.512.
Results
Descriptive statistics and outcomes
Two hundred and fifty infants met inclusion criteria, fifty-five of whom were late preterm. Forty percent of the late preterm infants were of the female sex as opposed to thirty-five percent of the term infants. There was no statistically significant difference in 5- and 10-minute Apgar scores, mean pH, race/ethnicity, or in the number of infants in each cohort who died. Late preterm infants had a slightly greater proportion of severe encephalopathy (18% vs. 10%, p = 0.13), a lower mean GA and BW, and a greater hospital length of stay (21 vs 13 days, p < 0.01). Term infants had a greater incidence of seizures (31 vs 13%, p < 0.01, Table 2).
Demographic and outcome characteristics
Demographic and outcome characteristics
As shown in Table 3, mothers of late preterm infants were statistically more likely to have a delivery complicated by pre-eclampsia (20 vs 9%, p = 0.02) while mothers of term infants were more likely to have no identified perinatal factors (37 vs 16%, p = 0.01). The rates of sentinel events were approximately the same between late preterm and term infants and were not significantly different (18 vs 14%, p = 0.53).
Obstetrical complications and sentinel events
aclinical findings of maternal fever, maternal tachycardia, and/or fetal tachycardia, bdefined as birth at 41 or more weeks of gestation, cdefined as ROM >18 hours.
Late preterm infants had higher neurologic exam scores for the Moro reflex (indicating greater abnormality) with a median score of 3 compared to a median score of 2 for the term infants. Late preterm infants also had higher neurologic exam scores for the respiratory component, with a median score of 1 compared to a median score of 0 for the term infants. There was otherwise no statistically significant difference in the level of consciousness, spontaneous activity, tone, posture, suck, pupils, or heart rate scores between the two groups (Fig. 1, Table 4). Likewise, there was no statistically significant difference in total Sarnat score between the two groups.
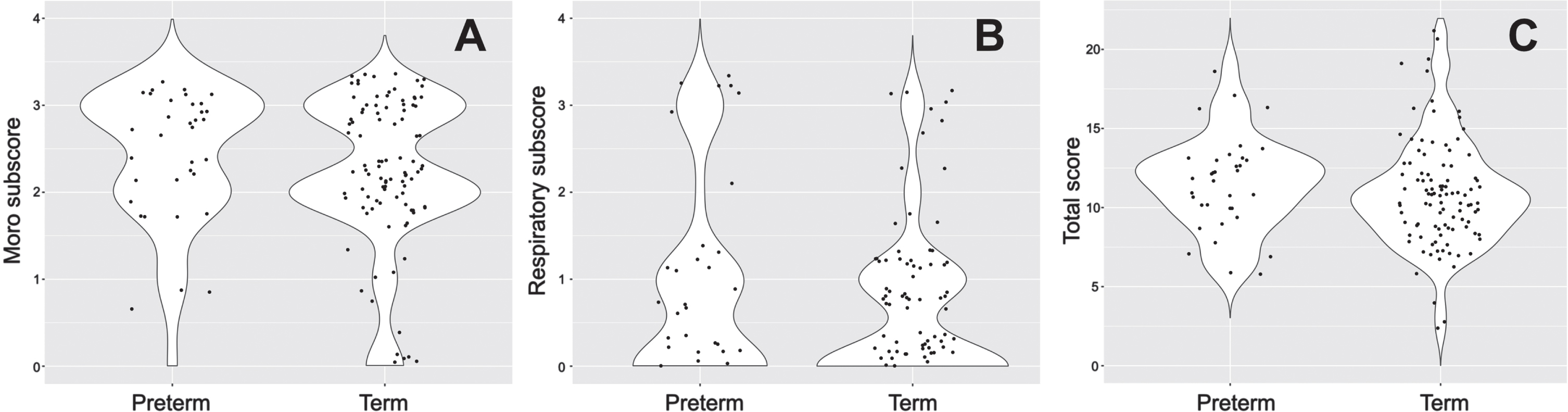
Violin plots of Sarnat scoring elements for preterm and term infants. In panel A, a shift towards a Moro reflex subscore of 3 in preterm infants is apparent. In panel B, a similar but more subtle shift in the distribution of respiratory subscore can be seen. In panel C, a broader distribution of the total Sarnat score is seen for term infants, at high and low levels. Total scores for preterm infants are much more consistent with a clinically insignificant shift of the center of the distribution.
Sarnat score comparison
Components scored where 0 = none, 1 = mild, 2 = moderate, 3 = severe.
The Sarnat score has provided a structured, common framework for the identification of infants at risk for moderate-severe encephalopathy since the 1970 s [17, 20–22]. Although developed long before the cooling era, this tool has formed the basis of repeated clinical trials and remains in widespread clinical use. During that time, very little modification [8] has been made to the exam, despite extension to a range of new uses, including evaluation of the late preterm infant. In this single-center retrospective study, we sought to evaluate if neurodevelopmental immaturity systematically influenced exam results, potentially driving a decision towards more therapy in these infants. Although differences between term and late preterm infants were identified (term infants having more seizures and late preterm infants having a greater hospital LOS), there was not a clinically or statistically significance difference in total Sarnat exam scores between the two groups. During the study period, TH treatment was considered for all infants with moderate or severe encephalopathy defined by the presence of moderate or severe abnormalities in at least 3 Sarnat exam components. Using our scoring rubric, this corresponds to a total score of at least 6. Regardless of the subtle differences in scoring between the populations, these data suggest that encephalopathy screening can be utilized in the late preterm population without risk of over identification on the basis on neurologic or neuromuscular immaturity. A late preterm infant demonstrating moderate or severe encephalopathy has a real condition and should be treated at a facility with TH capabilities.
Apnea is a common phenomenon in the NICU setting, especially in preterm infants [23, 24]. All infants, regardless of degree of prematurity, have a parasympathetic-dominant autonomic nervous system [25]. Any source of stress, whether it be a painful procedure, infection, or seizures, can lead to apnea. Prematurity exacerbates this tendency, with decreased sensitivity of central and peripheral chemoreceptors leading to spells of periodic breathing and/or apnea of prematurity (AOP) [23, 27]. Compounding issues with central control of breathing in preterm and late preterm infants is immature neuromuscular status of the upper airways, which may cause partial or complete collapse of the airway and the potential for obstructive apnea [28]. While apnea of prematurity is most prevalent in infants born before 32 weeks of gestation, it is common even beyond that time. At 34 weeks gestation, about 20% of infants are affected by AOP with the incidence dropping steadily to less than 10% of infants by 37 weeks [29]. While the recorded Sarnat exams in this study do not constitute a formal diagnosis of apnea of prematurity, there was a clear shift towards more immature breathing patterns for encephalopathic late preterm infants.
Although the potential for differences in the neuromuscular exam driven by maturity would be anticipated, it has not been systematically studied. In one report from Pavageau and colleagues [30], inter-rater reliability of the Sarnat exam was studied in term and late preterm subgroups. Interestingly, the Moro exam was found to have the lowest inter-rater reliability and was the most unreliable for the subgroup of infants born between 32 and 36 weeks, although differences in scores were not compared. In our study, we utilized the scores recorded in the patient’s chart. Although it is our clinical practice for scoring to be performed by two providers, only the consensus score is recorded in the chart, thus further examination of inter-rater reliability cannot be assessed.
Hypoxic-ischemic encephalopathy is a significant cause of infant mortality [7, 31]. About 60% of infants with severe HIE die and neurodevelopmental disability, including intellectual impairment and cerebral palsy, is common in survivors. Therapeutic hypothermia works to alleviate hypoxic-ischemic injury by decreasing cerebral metabolic demands in order to prevent secondary energy failure and neuronal death [31, 32]. After worldwide rollout of therapeutic hypothermia for the treatment of moderate to severe HIE, there has been a significant (although incomplete) reduction in infant death and disability [7, 33]. Although generally well tolerated, TH is not without risks. There can be cardiovascular (i.e., bradycardia, arrhythmias, hypotension) or respiratory (i.e., pulmo-nary hypertension, impaired surfactant production) complications, electrolyte imbalances, coagulopathy, increased risk of sepsis, intolerance of enteral feeds, and increased sedation needs [34, 35]. Relevant to this study, a previous report suggested an increased risk of adverse events associated with TH use in the late preterm infant including hypo- and hyperglycemia, leukopenia, and need for early rewarming [15].
The balance of risks and potential benefits lies at the heart of a parallel clinical conundrum: the use of TH in mild encephalopathy. While it is clear that children diagnosed with mild encephalopathy have notable rates of brain injury on MRI and an increased risk of mild-moderate neurologic disability as toddlers, it remains unclear if TH improves this outcome [36–38]. However, in contrast to the infants with mild encephalopathy, all infants included this study had moderate or severe encephalopathy and would be expected to obtain some benefit from TH treatment, similar to that achieved in RCTs. Indeed, reports of HIE in late preterm infants suggest a greater burden of brain injury than term equivalent peers [15]. While this report, and others, continue to demonstrate a lower risk of seizures in the late preterm HIE infant, TH has a noted anti-epileptic effect and should be of benefit to this population for this alternate indication, despite being outside of the original trial inclusion criteria.
There are several important limitations to this study. First, this was a single-center retrospective study and validation in an external cohort will be important to confirm the findings. Next, although the compulsory Sarnat exam and standardized scoring flowsheet provided a robust and structured source of data, they are limited only to those fields. Additional observations or findings were not necessarily available, nor would have been entered with the same standardized rigor. Third, the encephalopathy exams were performed by different providers at different stages of training or experience level. While our clinical practice is for all scoring to be done with at least one senior-level provider, the neurologic exam is fundamentally subjective and there is no certainty of uniformity. Finally, we only studied infants who had been cooled. The primary question at hand was to assess if late prematurity causes a sufficient systematic difference in the neurologic exam as to shift TH treatment decisions, a concern not supported by the data. However, a significantly greater number of infants are screened for encephalopathy than are treated with encephalopathy and these infants were not included in this study. Future studies should consider examining this population, especially if TH treatment for mild encephalopathy is being considered, where a minute difference in exam may carry more weight.
Conclusion
In a series of RCTs with strict inclusion and exclusion criteria, therapeutic hypothermia was found to reduce the risk of death or severe neurodevelopmental disability. Natural practice drift has led to an increasing number of infants being screened and treated with TH. This study provides important data demonstrating that differences in neuromuscular or respiratory maturity in late preterm infants are responsible for a clinically and statistically insignificant difference in the overall exam score and the risk of overidentifying infants on the basis of immaturity alone is slight. Future validation studies are needed to ascertain the interaction between late prematurity and mild encephalopathy or the long-term neurodevelopmental outcomes of late preterm infants undergoing therapeutic hypothermia treatment.
Conflict of interest
The authors report no conflicts of interest.
Funding
NIH Career Development Award K23 NS111086 [Vesoulis].
None of the authors have potential or actual financial interests relevant to the topics discussed in the manuscript.