
Abstract
Streptococcus gallolyticus subspecies pasteurianus is a subtype of Streptococcus bovis (S. bovis) that has become increasingly recognized as a sepsis-causing pathogen in neonates. It is well documented that S. bovis species have a predilection to both cardiac and gastrointestinal tissue, and in adult populations, isolating these organisms in the bloodstream often triggers further evaluation for co-morbid complications such as colon cancer or endocarditis. However, no such guidance currently exists in neonatal literature. We present a case of a preterm infant with S. gallolyticus subsp. pasteurianus bacteremia presenting as necrotizing enterocolitis (NEC) not previously described in the literature. Furthermore, through a complete diagnostic evaluation, including an echocardiogram, our patient was found to have the rare complication of endocarditis.
Keywords
Introduction
Over the past few decades, Streptococcus bovis (S. bovis) has undergone significant taxonomy classification changes. First discovered in 1919, S. bovis is a gram-positive cocci in pairs or short chains. Later studies further divided S. bovis into biotype I or II and subdivided phenotypic biotypes into subspecies [1, 2]. As the ability to appropriately classify these organisms advanced, it became clear that these pathogens showed a predilection for specific tissues. Adult literature demonstrates an association between S. bovis and colorectal cancer or infective endocarditis [3, 4].
The ability to use genetic-based classification has further advanced the classification into S. gallolyticus subsp. pasteurianus, S. infantarius subsp. coli, and S. infantarius subsp. Infantarius [2, 5]. In the pediatric literature, S. gallolyticus subsp. pasteurianus is a rare but increasingly recognized cause of neonatal sepsis and meningitis [6, 7]. While adult literature supports further diagnostic workup of gastrointestinal and cardiac pathology when S. bovis species are identified in the bloodstream [8], no current recommendations exist in the pediatric literature. To our knowledge, we present the first reported case of a neonate with S. gallolyticus subsp. pasteurianus bacteremia with both necrotizing enterocolitis (NEC) and infective endocarditis (IE).
Case presentation
Our patient is a preterm infant male born at 33 +0 weeks of gestational age via emergent cesarean section because of maternal pre-eclampsia with severe features and non-reassuring fetal heart tracings. Pregnancy was complicated by intrauterine growth restriction first noted on routine anatomy scan at 20 weeks gestational age. Maternal prenatal care was unremarkable, with normal prenatal labs; however, group B Streptococcus status at delivery was unknown. At delivery, the infant required continuous positive airway pressure (CPAP) during resuscitation and was transferred to the Neonatal Intensive Care Unit (NICU) for continued respiratory support and management of prematurity. He was quickly weaned to room air on day of life (DOL) 1. Otherwise, he had an uneventful NICU course outside of intermittent hypoglycemia managed with dextrose-containing IV fluids while advancing enteral feeds.
On DOL 27, concerns arose for increased fussiness with difficulty consoling the infant. At the time of evaluation, the infant had tachycardia, abdominal distension, guarding, and hypoactive bowel sounds. Laboratory evaluation was significant for an elevated immature to total (I/T) neutrophil ratio of 0.35 and elevated C-reactive protein of 19.72 mg/dL. His electrolytes were within normal limits, extended respiratory viral panel PCR was negative, and a blood culture was obtained. An abdominal radiograph showed distended bowel loops, multiple areas with a reticular pattern, and evidence of pneumatosis intestinalis along the distal colon (Fig. 1). Given radiographic and clinical findings, our patient was diagnosed with necrotizing enterocolitis (NEC), made NPO, and started on broad-spectrum antibiotics with Vancomycin and Piperacillin/Tazobactam.
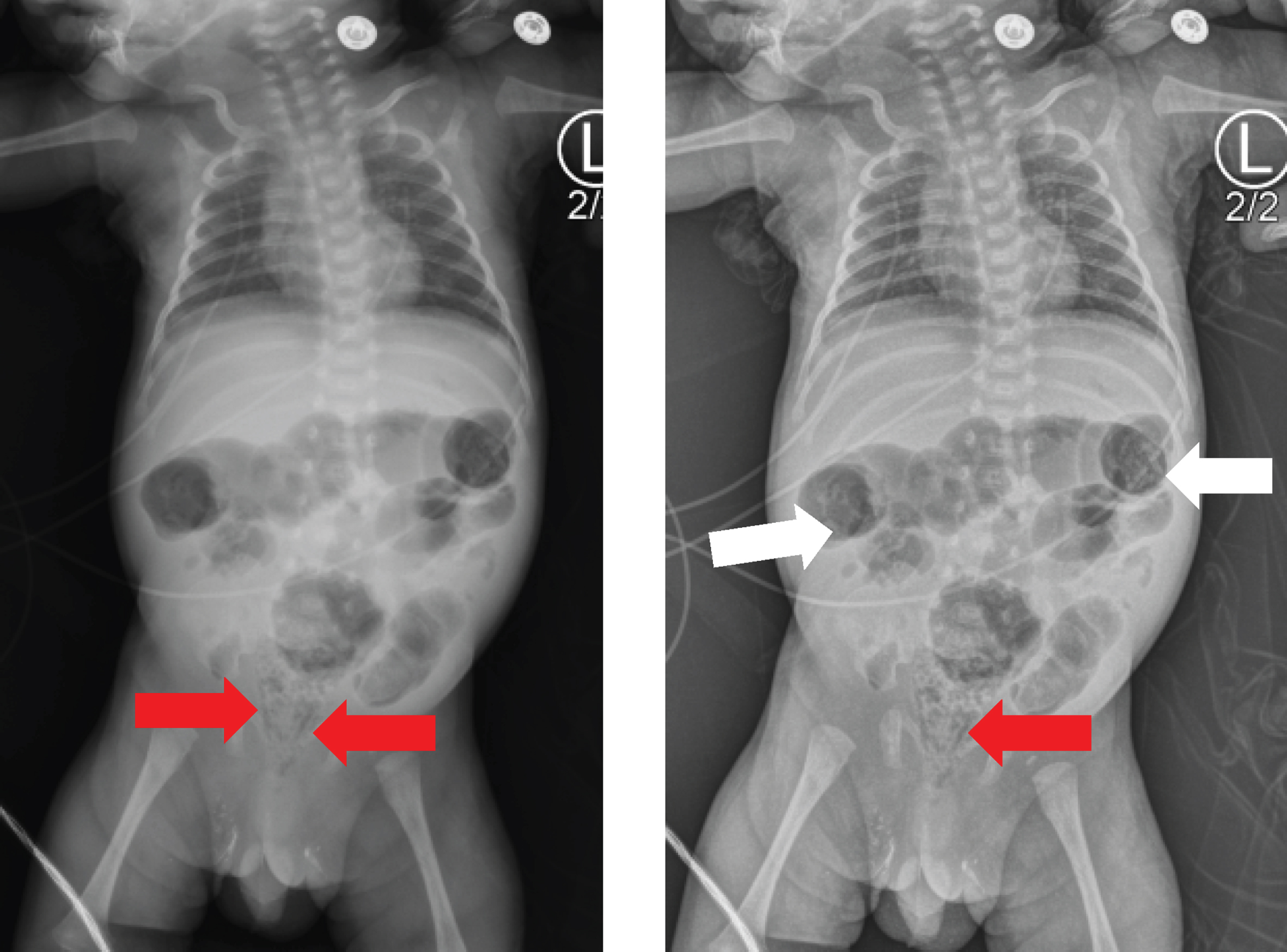
Portable abdominal x-rays showing distended bowel loops, multiple areas with reticular pattern (white arrows), and areas along the distal colon concerning for pneumatosis intestinalis (red arrows).
Shortly after initiating antibiotic treatment previously drawn blood culture resulted positive at twelve hours for gram-positive cocci, later speciated to Streptococcus gallolyticus subspecies pasteurianus. Cerebrospinal fluid and urine cultures were obtained; both resulted in no growth. Based on speciation and sensitivities, antibiotics were narrowed to single coverage with Penicillin G with the initial intention to treat for 14 days for bacteremia. Upon review of the literature and noting a predilection for S. gallolyticus species to endocardial tissue, the decision was made to obtain an echocardiogram to evaluate for any evidence of endocarditis/arteritis. Echocardiogram showed an 8 mm echo-lucent object within the remnant of the PDA consistent with vegetation (Fig. 2) concerning for infective endocarditis (IE).
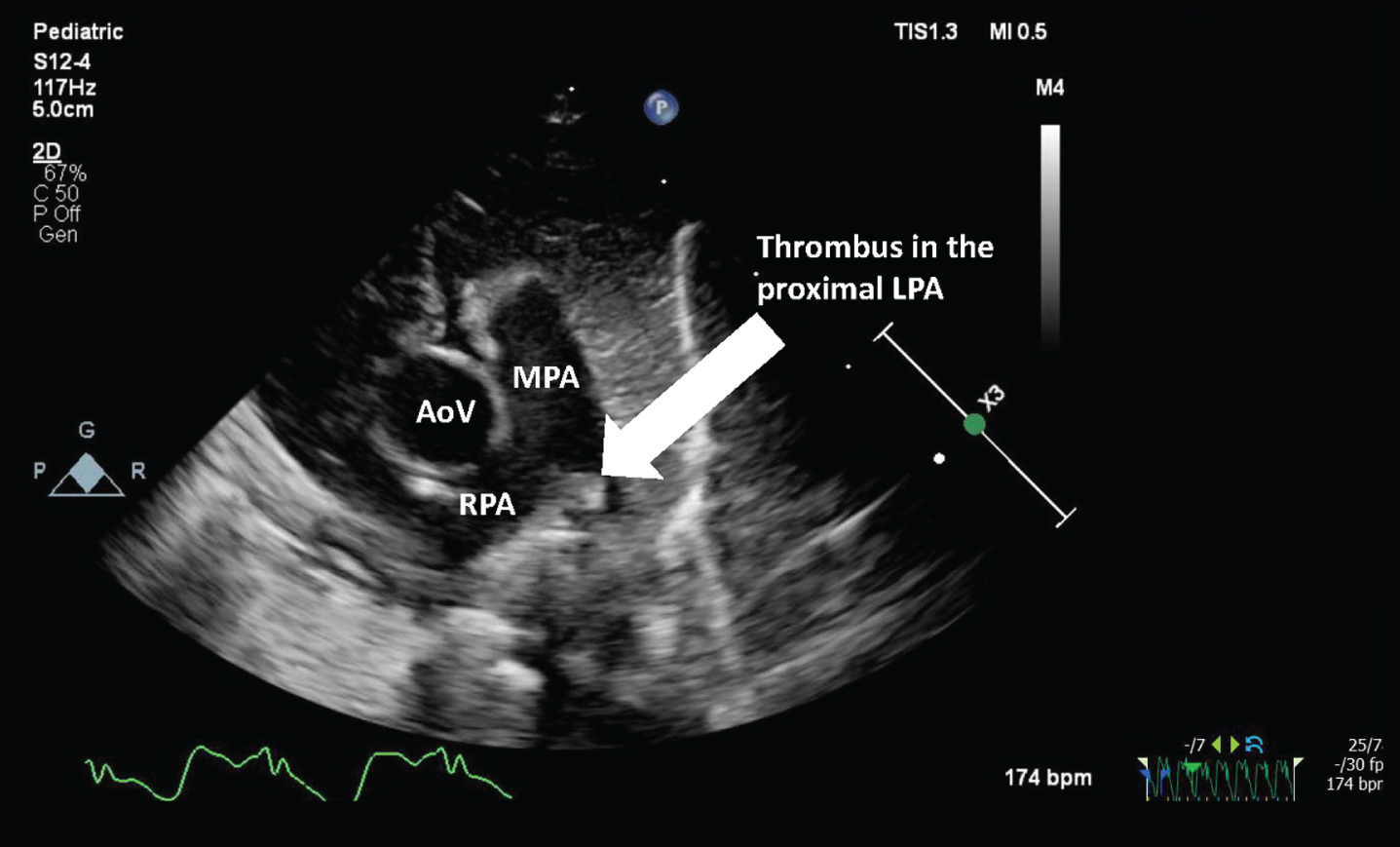
Modified parasternal short axis view showing an 8 mm echo-lucent object (white arrow) proximal left pulmonary artery (LPA) at the pulmonary artery bifurcation. AoV- Aortic Valve, RPA- Right pulmonary artery, MPA- main pulmonary artery.
Ultimately the decision was made to extend treatment with Penicillin to 28 days for an endocarditis treatment course, which our patient completed without further complications and was able to discharge home on DOL 55. The infant has since been followed outpatient with routine pediatrics care without further clinical concerns.
We highlight a case of late-onset sepsis in the preterm infant caused by S. gallolyticus subsp. pasteurianus with both necrotizing enterocolitis and infective endocarditis. This case was complicated by a unique presentation of NEC in a nearly four-week-old infant who was well-established on enteral feeds without other predisposing risk factors. A diagnostic evaluation demonstrated S. gallolyticus subsp. pasteurianus bacteremia, which we believe was the initial insult leading to NEC.
As taxonomy for group-D strep advances, the goal is to focus clinical evaluations based on the specific pathogen identified. Early research has shown that different biotypes have significantly different rates of associated diseases. Recent literature reviews have found the true prevalence of S. gallolyticus infection and its subspecies remains unknown as there are cases of neonatal infection by S. bovis that have not been identified at the subspecies level [9]. In adults, there have been drastically higher rates of endocarditis or colonic neoplasia in patients with S. bovis biotype I bacteremia than those with biotype II [10]. However, a recent study reported biotype II is the most common pathogen among S. gallolyticus in neonatal infections, most commonly presenting as neonatal sepsis and meningitis [6, 10]. Interestingly our patient’s primary manifestation was NEC, and he was subsequently found to have bacteremia but a negative CSF culture.
The decision to obtain an echocardiogram was widely discussed among the care team for this neonate. While review of the literature showed a lesser rate of IE among S. gallolyticus subsp. pasteurianus (biotype II) bacteremia, it was still seen in a small percentage of cases. Additionally, although S. gallolyticus has been linked with cases of endocarditis in adult patients, this is only the second case to have been reported in the neonatal population [9]. We recognized that the scarce availability of genetic or molecular sequencing for sub-speciation continues to obscure the literature, and only a little of the literature is in pediatrics. Ultimately, the decision to obtain an echocardiogram was based on the known predilection for S. bovis species for gastric and cardiac tissue. This decision led to the findings concerning for IE in our patient, which determined the longer course of antibiotics.
Our novel case highlights a current uncertainty about the significance and complications of S. bovis infections in neonates. This case stresses the need for more access to testing allowing the proper microbiological classification of S. bovis infections, and the importance of further research on neonatal manifestations of these infections. Until then, we suggest a thorough CSF, gastrointestinal, and cardiac evaluation in any neonate with a S. bovis bacteremia.
Ethics statement
Written consent was obtained from the legal guardians of the patient for publication of this case report and all accompanying images prior to writing or submitting this manuscript.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding
The authors have no funding sources to disclose.
Disclaimer statement
The views and opinions expressed are those of the authors alone and do not represent the opinions of the United States government, United States Army, Defense Health Agency, or Tripler Army Medical Center.