
Abstract
In this case report, we describe two repeated transcutaneous electromyography of the diaphragm (dEMG) measurements in an infant with suspected paresis of the right hemidiaphragm after cardiac surgery. The first measurement, performed at the time of diagnosis, showed a lower electrical activity of the right side of the diaphragm in comparison with the left side. The second measurement, performed after a period of expectative management, showed that electrical activity of the affected side had increased and was similar to the activity of the left diaphragm. This finding was accompanied by an improvement in the clinical condition. In conclusion, repeated measurement of diaphragmatic activity using transcutaneous dEMG enables the observation and quantification of spontaneous recovery over time. This information may assist the clinician in identifying patients not responding to expectative management and in determining the optimal timing of diaphragmatic surgery.
Introduction
In newborns, phrenic nerve injury can arise due to a traumatic birth (incidence ranging from 1/15.000 to 1/30.000 births), or after cardiothoracic surgery (prevalence between 0.3–12.8%) [1, 2]. Although the incidence is modest, the impact can be profound as phrenic nerve injury can result in a reduced diaphragm muscle strength (paresis) or extreme muscle weakness (paralysis) leading to symptoms of respiratory distress and difficulty/impossibility to wean the newborn from (non-)invasive ventilation. Current diagnostic tools are Chest X-ray (CXR) and diaphragm ultrasound. However, these techniques have limitations such as exposure to radiation, not applicable at the bedside, and paradoxical movements of the diaphragm leading to false-negative results [1].
Transcutaneous electromyography of the diaphragm (dEMG) measures the electrical activity of the diaphragm, a measure of breathing effort. In order to measure dEMG, adhesive electrodes, additional hardware and software are required. In contrast to CXR and diaphragm ultrasound, this technique is non-invasive, radiation-free, and easily applicable at the bedside. And more importantly, it provides continuous information on the diaphragm activity and can detect differences in electrical activity between both sides of the diaphragm, which could enable the diagnosis of diaphragmatic hemiparesis [3, 4].
In many patients with diaphragmatic paresis, an expectative approach is followed as spontaneous recovery may occur, thereby avoiding unnecessary surgical plication. However, the time needed for spontaneous recovery may vary. Therefore, there is a need for an adequate and easy-to-use method to determine whether recovery occurs [1, 5]. Such a monitoring tool could contribute to the process of clinical decision making on whether or not surgical plication is indicated, either on a short or a long term.
dEMG can quantify the change in diaphragmatic activity in response to different interventions [6, 7]. Therefore, monitoring recovery of unilateral diaphragmatic paresis using dEMG should also be feasible. To our knowledge no study has reported the use of dEMG for this purpose in infants. Our report describes the results of two repeated dEMG measurements in an infant with diaphragmatic hemiparesis, one at the time of diagnosis and one after recovery of diaphragm activity.
Case report
The index patient (gestational age 39 weeks, birth weight 2900 gram) had multiple congenital heart disorders, for which she underwent corrective surgery in the first three weeks of life. After a period of invasive mechanical ventilation, she was successfully extubated and received continuous positive airway pressure (CPAP). However, weaning of CPAP was unsuccessful and physical examination showed asymmetry of the chest and subcostal retractions on the right side. The CXR showed an elevated right hemidiaphragm and ultrasound revealed no diaphragm movement on this side. Based on these findings she was diagnosed with right-sided diaphragmatic paresis, most likely caused by phrenic nerve injury following thoracic surgery.
An expectative management was followed including physiotherapy focused on increasing respiratory muscle strength (daily at first followed by 2-3 times a week) for±2 weeks. Over time the patient’s clinical status improved with increased movement of the right chest, and the patient was successfully weaned from CPAP to high flow nasal cannula. Consistent with this finding a second ultrasound showed improved movement of the right hemidiaphragm. At the age of 5 months the patient was discharged home.
Transcutaneous dEMG measurement
To assess the ability of dEMG to diagnose diaphragmatic hemiparesis but also assess its recovery, two repeated dEMG measurements were performed with a duration of at least 30 minutes, each. First, when the patient could not be weaned of CPAP and there was a strong suspicion of diaphragmatic hemiparesis (age: 8 weeks). Second, after 2 weeks of expectative management followed by clinical improvement.
During each measurement, the left and right hemidiaphragm were measured separately as previously described [4]. Two skin electrodes (disposable Kendall H59P Electrodes; Covidien, Mansfield, MA) were placed bilaterally at the costo-abdominal margin in the nipple line, two bilaterally at the same height at the back and one reference electrode on the sternum. These electrodes were connected to a signal amplifier (Porti, TMSi, Oldenzaal, The Netherlands) to detect muscle activity. Customized software in Polybench (Applied Biosignals, Weener, Germany) was used to process the data and to obtain the diaphragm activity signal curves of the left (dEMGL) and right (dEMGR) hemidiaphragm [8]. Offline curve analysis was done in MATLAB (v2019b, MathWorks, USA).
To compare the electrical activity of the dEMGR and dEMGL, breath detection was performed in as table 1-minute period in both measurements. The amplitude (difference between highest and lowest electrical activity) was calculated per breath and visualized in a bar plot. Differences in average amplitude between dEMGR and dEMGL during the first measurement and between the two repeated dEMGR measurements were tested with an unpaired/paired t-test or Mann-Whitney U test, according to the data distribution.
Results
Two dEMG measurements were performed with a length of 80 and 105 minutes. A representative 1-minute tracing of the dEMGR and dEMGL was selected in both measurements (Fig. 1). The average amplitude during the first measurement was significantly lower in the dEMGR (1.8±0.4μV) compared to the dEMGL (5.1±1.9μV) (p < 0.001) (Fig. 2). The second measurement showed a significant increase in dEMGR (p < 0.001) and a decrease in dEMGL compared to the first measurement. As a result, the average amplitude was similar (2.5±0.6μV) on both sides during the second measurement.
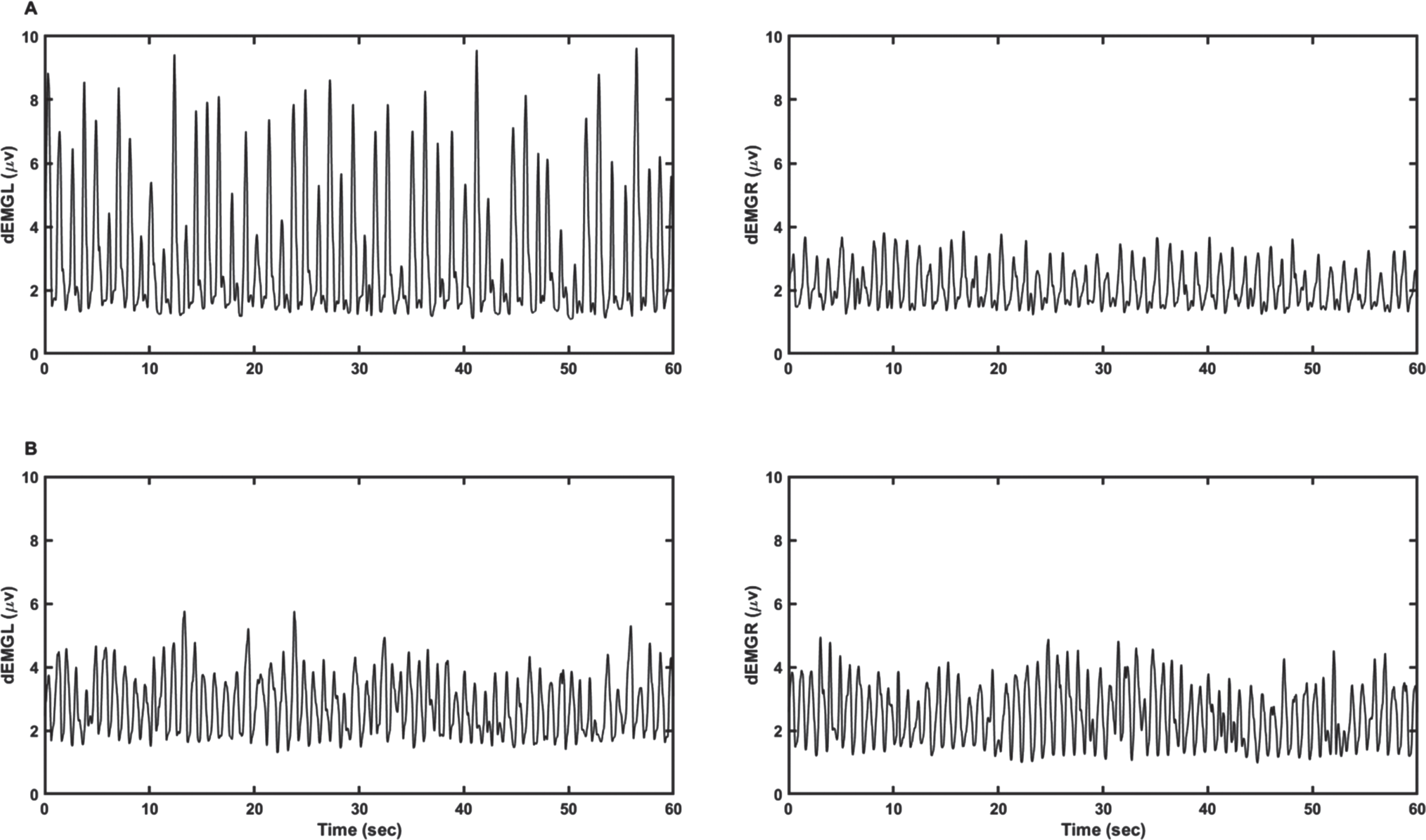
Measured diaphragm activity. 1-minute tracing of the electrical activity (μV) of the right (dEMGR) and left (dEMGL) diaphragm of the index patient of the first (A) and second measurement (B). In the first measurement, the dEMGR was reduced compared to the dEMGL. In the second measurement, the activity of the dEMGR was increased, while the dEMGL is decreased compared to the first measurement. Here, both sides showed a similar electrical activity.
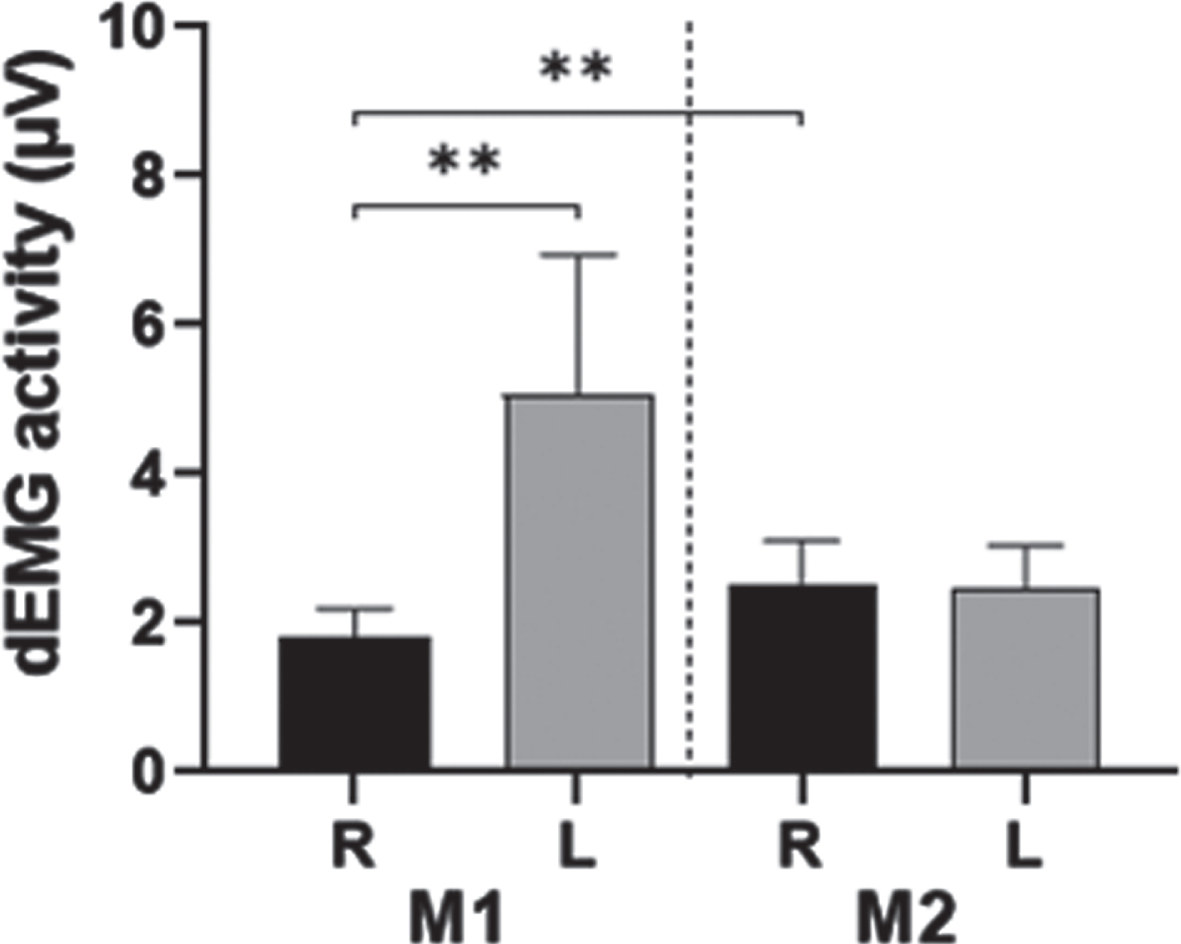
Amplitude. Bar plots (mean and standard deviation) of the amplitude of the detected breaths in the one-minute tracing of the right (R) and left (L) diaphragm of the first (M1) and second (M2) transcutaneous electromyography (dEMG) measurement. The average amplitude in the first measurement was significantly higher on the left side compared to the right side of the diaphragm. In the second measurement, the average amplitudes were comparable. **p < 0.001.
To our knowledge this is the first case report showing the ability of repeated transcutaneous dEMG measurements to monitor spontaneous recovery over time in an infant diagnosed with diaphragmatic hemiparesis.
After diagnosis of diaphragmatic hemiparesis, either an expectative or surgical approach can be followed. As the time needed for spontaneous recovery may vary between patients, monitoring the change in diaphragmatic activity of the affected side over time is crucial [5]. Based on the previously mentioned advantages, transcutaneous dEMG is an ideal candidate for this purpose. In addition, dEMG can quantify the diaphragmatic activity, which would theoretically allow it to monitor the stepwise improvement over time.
In this patient case, the electrical activity of the affected hemidiaphragm significantly increased over time and became similar to the unaffected side. These changes were accompanied by an improvement in the patient’s clinical condition and the ability to wean the non-invasive respiratory support. Therefore, this change in diaphragm activity can be seen as clinically significant. Similar findings were observed when measuring diaphragm activity with an esophageal catheter during a spontaneous breathing trial in infants with bilateral diaphragmatic paresis [9]. Interestingly, in our patient the dEMGL was higher at the first measurement than the second measurement, which is suggestive for compensation of function loss of the affected side. This could be considered an additional indication consistent with the diagnosis and recovery of one-sided diaphragmatic paresis.
A limitation of our method is that signal strength is also influenced by the muscle-to-electrode distance [10]. In case of diaphragmatic hemiparesis, diaphragmatic elevation may therefore contribute to the decrease in electrical activity on the affected side, as the electrodes are positioned at the costo-abdominal margin on both sides. Nevertheless, both reduced muscle activity and diaphragmatic elevation, are signs of diaphragmatic hemiparesis. The measured signal at the affected side of the diaphragm might also be (partly) caused by crosstalk, either originating from the unaffected side or from other (inspiratory) muscles [11]. This could potentially lead to false negative results as no normative dEMG values exist. Therefore, it is important to measure both sides of the diaphragm to enable direct comparison. Electrical interference could also influence the measured signal, which is prevented by using shielded electrode wires and constructing bipolar derivations of both sides of the diaphragm in our measurement set-up. In addition, movement influences the measured signal by introducing artefacts, which necessitates selecting stable signal segments as is performed in this case report.
Future research should focus on performing repeated or continuous dEMG measurements in patients with diaphragmatic paresis to assess the ability to monitor stepwise improvement over time. These data could also be used in combination with clinical information to determine a cut-off regarding the change in diaphragm activity of the affected side that represents clinically relevant recovery (e.g., reduction in the level of respiratory support). A validation study could investigate whether this cut-off can distinguish between patients in whom spontaneous recovery occurs and those in whom it does not. This may help in deciding whether or not surgical plication is necessary. Moreover, the ability to monitor diaphragmatic recovery should be confirmed in older children and adults.
Conclusion
Our study shows that repeated dEMG measurements or continuous dEMG monitoring can enable observation and quantification of spontaneous recovery of diaphragmatic hemiparesis. This could assist clinicians in determining if and when surgical plication is indicated.
Funding
No funding was obtained.
Ethical statement
Written informed consent was obtained from the infant’s parents for publication of this case report.