
Abstract
BACKGROUND:
Congenital syphilis is a vertical infection caused by Treponema pallidum. Despite the implementation of preventive strategies during pregnancy, its incidence is increasing, and it constitutes an important public health problem. Most patients with congenital syphilis are asymptomatic; however, a small group may develop severe disease at birth with the need of advanced resuscitation in the delivery room, acute hypoxemic respiratory failure, and hemodynamic instability. Therefore, awareness is needed.
METHODS AND RESULTS:
This series describes the clinical course of two late preterm infants with congenital syphilis who developed acute hypoxemic respiratory failure, pulmonary hypertension, and circulatory collapse early after birth. Integrated hemodynamic evaluation with neonatologist-performed echocardiography (NPE) and therapeutic management is provided.
CONCLUSIONS:
A comprehensive hemodynamic evaluation including early and serial functional echocardiography in these patients is needed to address the underlying complex pathophysiology and to help to establish accurate treatment.
Keywords
Introduction
Congenital syphilis (CS) is a vertical infection caused by Treponema Pallidum. Since 2012, its incidence has been increasing every year in parallel with the rising incidence of syphilis in reproductive age women [1, 2]. In 2019 in the United States, the incidence was 48.5 cases per 100,000 live births, which represented a 477% increase relative to 2012 [1]. Transmission of T. pallidum can result via transplacental route or from birth canal due to contact with maternal genital lesions. The risk of transmission depends on the gestation age (increasing in later weeks), and the stage of maternal disease (with a higher risk in early syphilis, especially in secondary syphilis) [2, 3].
The clinical features of congenital syphilis are the result of active infection by T. pallidum and the inflammatory response in the different organs and tissues. It is associated with fetal death, spontaneous abortion, fetal hydrops, intrauterine growth restriction and preterm delivery [3].
Most infants born to untreated mothers have no signs of infection and may develop symptoms later in childhood if they are not treated (late CS) [2, 3].
Common manifestations of early congenital syphilis include hematologic abnormalities, hepatomegaly, hepatitis, mucocutaneous lesions, rhinitis, ocular alterations, pneumonitis, myocarditis, nephrotic syndrome, and bone abnormalities. Central nervous system involvement occurs in 50% of patients and its manifestations include seizures, strokes, pituitary dysfunction, or diabetes insipidus [3].
It is of note, however, that although a minority, infected foetuses may exhibit a severe form of early CS suffering acute hypoxemic respiratory failure secondary to pulmonary hypertension (PH), hypoxic-ischemic encephalopathy (HIE), liver failure and severe coagulopathy and need for advanced resuscitation at birth [4–6].
Case report
Case 1
A male infant was born to a 45-year-old woman after an uncontrolled gestation until week 24. Third trimester serology was positive for syphilis and the mother was treated with Penicillin G Benzathine (2.4 million IU single dose) without subsequent serological follow-up. The delivery was eutocic at 36+5 weeks of gestation.
At birth, the newborn showed non-regular respiratory drive and hypoxemia that prompted endotracheal intubation and mechanical ventilation with 100% oxygen.
Physical examination showed desquamative lesions on hands and feet, and enlarged liver and spleen. He developed severe coagulopathy (International normalized ratio, INR > 7, prothrombin activity < 3%), early cholestasis (direct bilirubin 6.94 mg/dL), thrombocytopenia (25.000/mcL) and bilateral lower limb metaphyseal osteitis. The baby started on Penicillin G (50 000 UI/kg/dose every 12 h) treatment immediately after birth.
Early acute hypoxemic respiratory failure resulted in persistent 100% oxygen needs despite no ventilation problems (pH 7.34, PaCO2 46.3mmHg, PaO2 44mmHg, PaO2/FiO2 44, oxygenation index 34) and a chest X-ray with no relevant findings. Echocardiography scan conducted in the first hour of life to rule out congenital heart defects and to assess pulmonary pressure and blood flow, showed right ventricular (RV) dilatation with tricuspid annular plane systolic excursion (TAPSE) of 10 mm (normal range 6,8–9,6 mm), tricuspid insufficiency (TI) that estimated supra-systemic PH, patent ductus arteriosus (PDA) and foramen ovale, both with right-to-left shunt. Based on findings suggestive of pulmonary hypertension, continuous sedation with fentanyl (2 mcg/kg/min) and inhaled nitric oxide at 20 ppm was prescribed, resulting in improved oxygenation and reduced oxygen requirement up to 50%. Despite of that, progressive circulatory failure and systemic hypotension, oliguria and metabolic acidosis (lactatemia up to 8.2 mmol/L at six hours from birth) was observed. Neonatologist performed echocardiography (NPE) was conducted at this time in order to obtain information on biventricular function and cardiac output, depicting RV dysfunction (severe IT and RV dilatation), high pulmonary pressures in the presence of systemic hypotension (75–80% of systemic pressure estimated by TI), TAPSE of 7.7 mm, and normal left ventricular (LV) function (60% ejection fraction) and LV output of 185 mL/Kg/min (Fig. 1A). Accordingly, epinephrine (maximum 0.13 mcg/Kg/min) was started. Even though systemic blood pressure and respiratory condition improved (FiO2 up to 40%), the echocardiographic findings continued to show signs of PH (Fig. 1B), severe RV dysfunction (TAPSE 6 mm), and mild LV dysfunction appeared (50% LV ejection fraction) and dobutamine (7 mcg/kg/min) was added, resulting in clinical stabilization and echocardiographic improvement (Fig. 2).

A: Significant tricuspid (left) and pulmonary (right) valvular insufficiencies. B: Large PDA of 5 mm with bidirectional shunt (30% R-L) suggesting significant pulmonary hypertension.

A: Large PDA of 3.2 mm with predominantly left-right shunt. B: Improvement of RV systolic function measurements. TAPSE 8 mm. C: LV ejection fraction of 69%, biplane mode.
Epinephrine and dobutamine were withdrawn on the 5th and 7th day of life, respectively and the infant was extubated on the 6th day of life.
The diagnosis of congenital syphilis was confirmed by positive serology at birth (IgM positive, IgG positive, Rapid Plasma Reagin positive), and polymerase chain reaction positive for syphilis in the skin lesions.
The patient was treated with intravenous penicillin G during 10 days.
A preterm male infant was born at 34+0 weeks’ gestation by emergency caesarean section. The mother was a 19-year-old woman that had a poorly controlled pregnancy. She presented positive serology for syphilis in the first trimester but did not complete the prescribed treatment. Non-responding bradycardia and absent respiratory effort at birth were observed and advanced resuscitation manoeuvres with endotracheal intubation and 100% of FiO2 were started. On admission to Neonatal Intensive Care Unit (NICU), the baby received surfactant followed by high frequency ventilation, with mean airway pressure of 23 cmH2O and 100% FiO2. Blood gas assessment showed severe mixed acidosis (pH 6.60, lactic acid 20 mmol/L, bicarbonate 5 mmol/L, PaCO2 108mmHg, PaO2 15,1 mmHg, PaO2/FiO2 15, oxygenation index 152) at first hour from birth.
The physical exam depicted desquamative skin lesions (Fig. 3) and lab tests showed hypertransaminasemia (AST 1585 IU/L, ALT 441 IU/L), cholestasis (direct bilirubin 8.85 mg/dL), anemia (10.3 g/dL), thrombocytopenia (23.000/mcL) and coagulopathy (INR 2.8, prothrombin activity 22%). Treatment with Penicillin G (50,000 IU/kg/dose every 12 h) was started and continued for 10 days. The diagnosis of congenital syphilis was confirmed at 24 hours of life after detection of T.pallidum in the skin lesions and positive serological tests in blood (IgM, IgG, RPR).
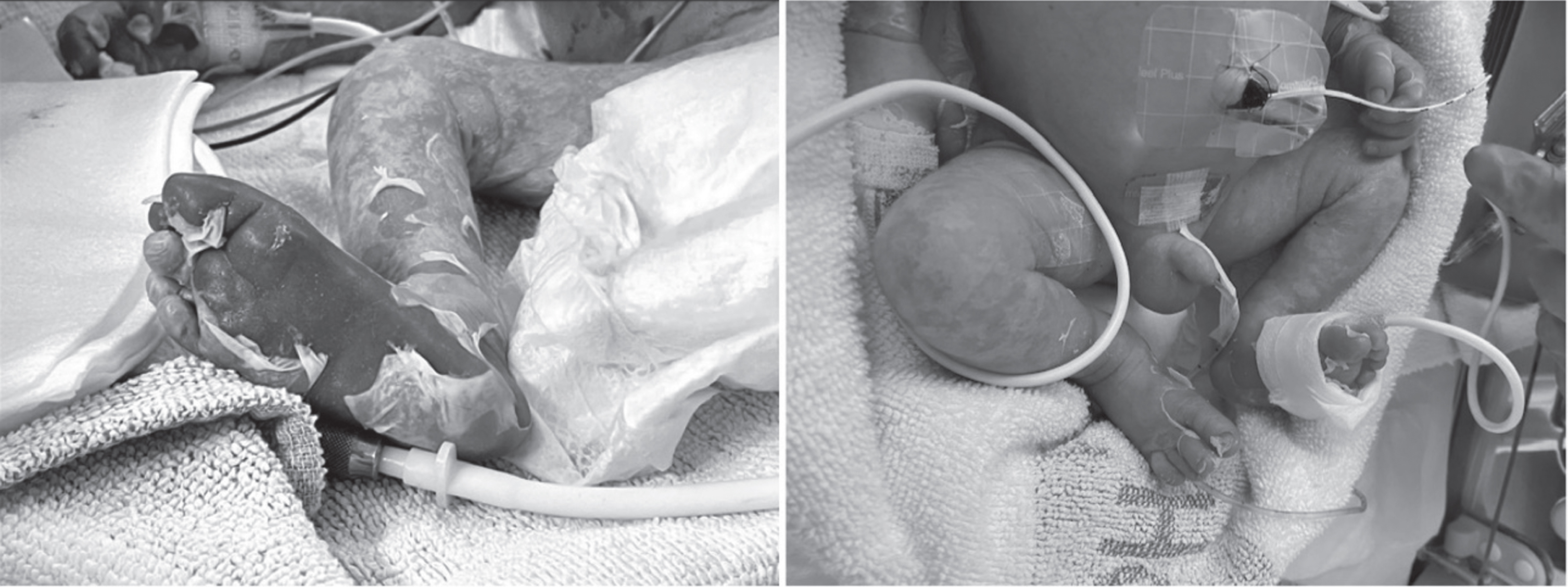
Desquamative lesions on lower extremities in first (left) and second (right) day of life.
NPE revealed signs of supra-systemic PH (50 mmHg estimated by TI for systolic blood pressure 40mmHg), RV dilatation, right-to-left shunt through the foramen ovale, and a large PDA (maximum diameter 3.5 mm) with bidirectional shunt.
Treatment was started with dobutamine (6 mcg/Kg/min) and inhaled nitric oxide (20 ppm) causing oxygenation improvement and lower FiO2 requirements up to 50%.
Clinical and biochemical signs of systemic perfusion improved along the first day of postnatal life. Serial NPE studies confirmed a progressive decrease of pulmonary pressures which permitted nitric oxide and dobutamine halting at 48 hours and 96 hours of birth, respectively. The patient was successfully extubated on the 5th day of life.
Two cases of CS with acute severe hypoxemic respiratory failure due to PH and circulatory insufficiency are presented. This condition associated with CS is rarely stated in the medical literature [4–6], or limited to old reports that are not representative of the current neonatal care [6]. Spear et al. [6] reported on a newborn with CS and PH who suffered a fatal outcome. Pillay et al. [4], reported a case series of symptomatic CS in a tertiary NICU in South Africa. In this series of 50 patients, 50% required resuscitation at birth and 65% NICU admission. PH was present in 12% of the cases. Aleem et al. [5], reported a retrospective case series of 5 patients with severe clinical forms of CS from June 2016 to February 2020. All of them required intubation at birth and 2 infants needed advanced resuscitation with chest compressions and epinephrine. One patient died in the delivery room. The remaining patients presented hypoxemic respiratory failure with PH, neonatal encephalopathy and coagulopathy. Neither Pillay nor Aleem provide data about how the diagnosis and management of PH and circulatory insufficiency were made, or how was the infants’ outcome as we do in the present report.
Acute PH in the newborn is defined as the failure of the normal decrease in pulmonary vascular resistance (PVR) after birth, which can associate or not RV systolic dysfunction. In the newborn, due to the presence of foetal channels, PH results in the shunting of deoxygenated blood from the pulmonary to the systemic circulation, causing hypoxemia. PH can also be caused by left ventricular dysfunction and increased pulmonary blood flow [7]. In severe forms of PH, the inability of the immature RV myocardium to compensate this increased afterload results in decreased pulmonary blood flow. Moreover, the decrease in pulmonary flow results in decreased LV preload, which is already compromised by leftward deviation of the interventricular septum [7, 8]. All these factors result in global cardiac dysfunction and systemic hypoperfusion state [7, 8].
Altered PVR may be associated with lung parenchymal diseases or systemic diseases, such as CS. Infection by T. Pallidum produces systemic inflammation in different organs and tissues, altering normal adaptation of PVR [3]. The approach includes agents to decrease PVR (NOi) and inotrope treatment to augment ventricular performance. The choice of inotropic agent is dependent on systemic arterial pressure, presence of RV dysfunction, LV dysfunction, or both. When RV dysfunction is involved, dobutamine or milrinone are the drugs of choice providing systemic blood pressure is maintained within normal ranges. However, treatment with low-dose epinephrine or norepinephrine should be prescribed in the case systemic hypotension is present [8].
Considering the complexity of PH assessment in the newborn and the condition severity if associated with circulatory failure, such is the case in the context of CS, a comprehensive evaluation with early and serial echocardiographic follow up are essential. This would help to establish as early as possible the most suitable, pathophysiology-oriented treatment in order to improve the short and the long-term infant’s outcomes.
Conflict of interest
None declared.
Patient consent for publication
Parents of patients provided informed consent for publication.