
Abstract
OBJECTIVES:
Hypernatremia may facilitate the diffusion of bilirubin through the blood-brain barrier and increase the risk of bilirubin encephalopathy. This study was conducted to compare the prognosis of jaundice infants with those with jaundice and hypernatremia.
METHODS:
A total of 615 term infants with idiopathic jaundice with or without hypernatremia were enrolled in this cohort study with 24-months follow-up at Ghaem Hospital, Mashhad, Iran, between 2010 and 2022. An in-house questionnaire including the laboratory evaluation and neonatal characteristics was used as the data collection tool. The follow-up of neonatal development status was performed using the Denver test II at 6, 12, 18, and 24 months after discharging from hospital.
RESULTS:
Normal outcomes were seen in 555 (90.2%) out of 615 studied infants, while 60 cases (9.8%) showed abnormal outcomes. Serum levels of sodium (P = 0.017), bilirubin (P = 0.001), urea (P = 0.024), and creatinine (P = 0.011) as well as hyperthermia (P = 0.046) and unconsciousness (P = 0.005) showed significant differences between the two groups. Approximately 16% of the newborns with both jaundice and hypernatremia, and 9% of those with only jaundice had unfavorable prognoses. Also, bilirubin level had the most predictive power (91.3%).
CONCLUSIONS:
Our results suggest that hypernatremia or jaundice alone, may affect the prognosis of infants aged 2 years; but jaundice and hypernatremia together, will intensify the developmental problems in jaundice infants. However, the role of hyperbilirubinemia in the incidence of complications is more than hypernatremia.
Acronyms and abbreviations
neonatal intensive care unit
Glucose 6-phosphate dehydrogenase
Introduction
Neonatal jaundice is the most common reason for clinical visits during the first week of infantile period. The hospitalization rate due to infantile hyperbilirubinemia has been reported as 17–19% [1, 2]. Low breast milk intake during the first days of life is considered as a risk factor in the severity of hyperbilirubinemia that can lead to weight loss and hypernatremia. According to a previous study, 12% of infants with hyperbilirubinemia suffer from hypernatremia [3]. Low breast milk intake leads to dehydration and increased bilirubin levels, hypernatremia, and azotemia that all together can cause cerebral damages [4, 5].
As a defensive mechanism against decreased breast milk intake, infants’ kidneys increase sodium reabsorption and fluid retention. The ultimate consequences are hypernatremia and prerenal azotemia. Infants’ kidneys are very sensitive to dehydration and decreased perfusion. In addition, insensible water loss from the skin and lungs continues due to skin immaturity. All these issues along with jaundice can affect the prognosis of icteric infants. The incidence and actual amount of weight loss and changes in sodium level in infants with jaundice is unknown [6, 7].
The symptoms of acute kernicterus are lethargy, poor feeding, loss of Moro reflex, decreased deep tendon reflexes, opisthotonos, bulging fontanelles, abnormal facial and organ movements, seizures, and organ spasms or rigidity [8]. Agitation, irritability, lethargy, seizures, jaundice, reduced breastfeeding, hyperthermia, weight loss of over 10%, hypotension, hypovolemia, poor perfusion, depressed anterior fontanelle, sunken eyes, severe thirst and polydipsia, skin thickening, and mucous dryness are the most common symptoms of hypernatremic dehydration [9–11].
Since the complications of jaundice are preventable, the American Academy of Pediatrics (AAP) has suggested that its etiologies should be recognized; the necessary examinations should be performed, the proper breastfeeding should be supported; and due to the fact that the jaundice peak is on the 3rd to 5th days of life, newborns should be followed-up during this period [12, 13].
Several studies have shown that neonatal hypernatremia may affect the infant development later [14, 15]. On the other hand, neonatal hyperbilirubinemia has also the same negative effects on the prognosis of infants; but it is still unclear whether hypernatremia with hyperbilirubinemia were existed together; what are the future effects on infants; and which one is more effective. Thus, we decided to carry out a prospective study to evaluate the prognosis of infants with jaundice and compare it with infants with both hypernatremia and jaundice.
Methods
Using convenience sampling method, a total of 670 term idiopathic jaundice infants with or without hypernatremia, aging 2–28 days, who were hospitalized in the neonatal intensive care unit (NICU), emergency, and pediatric wards, Ghaem Hospital, Mashhad, were enrolled in this cohort study with 24-months follow-up during 2010 to 2022. Ghaem Hospital is a referral general hospital with NICU (12 beds), nursing care level II (12 beds) and maternity ward (with nursing care level I), with annually about 2000 deliveries. In this study, the prognosis of infants with jaundice has been evaluated by various variables such as sodium, bilirubin, urea, and creatinine and compared with infants with both hypernatremia and jaundice. This study was approved by the Ethics Committee of Research Deputy of Mashhad University of Medical Sciences. An informed consent was signed by the infants’ parents before enrolling in the study. Jaundice was defined as yellow appearance with bilirubin level above 17 mg/dl in term infants. Also, hypernatremia was defined as serum sodium level above 150 mM/L. A checklist was completed based on the infant physical examinations, daily weight laboratory tests (sodium, bilirubin, urea, creatinine, hematocrit, and platelets), and complete maternal and neonatal characteristics (age, sex, chief complaint, first breastfeeding time, breastfeeding frequency). All examinations and paraclinical tests were performed/requested by the attending physician.
Infants over 37 weeks of pregnancy, newborns aged more than 2 days, infants with jaundice (serum bilirubin level≥17 mg/dl) and those with a requested serum sodium testing by the attending physician were included in the study.
Infants with jaundice due to blood group and RH incompatibility (n = 8) or G6PD deficiency (n = 3), cephalohematoma (n = 3), congenital anomalies (n = 4), neonatal sepsis (n = 2), meningitis (n = 1), family history of developmental delay (n = 3), formula-feeding (n = 8), and cases with incomplete data (n = 23) were excluded from the study.
The follow-up evaluation of neonatal development status was performed by one physician using Denver Developmental Screening Test II at 6, 12, 18, and 24 months after discharging from hospital. Denver test II is an international test for assessing the growth and development of infants from birth to 6 years old. It includes four categories of personal-social, language, fine motor, and gross motor skills. It is commonly used to identify speech and learning disorders, autism, mild to moderate mental retardation, and psychosocial problems. The titles in Denver test II have been precisely selected in all subgroups and cultures in terms of reliability and comprehensiveness of norms. In our study, infants with problems in any of the aforementioned categories were considered as developmental delay. Problem in only one category was considered as mild; in two categories as moderate; and in three or more categories as severe developmental delay. Idiopathic jaundice infants with or without hypernatremia were divided into two groups of normal outcomes (normal in all categories) and abnormal or unfavorable outcomes (delay in one or more categories or death). Also, the combination of sodium, bilirubin, in predicting unfavorable prognosis in idiopathic jaundice infants with or without hypernatremia is studied.
Data analysis was performed by T-test, Chi-square test, ROC curve, and regression models using SPSS software (version 20). The results were described in tables and statistical charts and then comparison between the idiopathic jaundice infants with or without hypernatremia with normal and abnormal outcomes was done. Chi-square test was used to define the risk ratios in predicting poor outcomes.
The following regression models were used to determine the predictive factors: The Hosmer and Lemow test was used to evaluate how well the model’s predicted probabilities match the observed probabilities of the outcome variable. We divided the data into multiple groups based on predicted probabilities and compared the observed and expected outcomes within each group. The test yields a chi-square statistic, and a significant result suggests that the model’s predicted probabilities do not fit well with the observed data. The Nagelkerke R Square is a measure of the proportion of variance explained by a logistic regression model. Ranging from 0 to 1 a Nagelkerke R Square of 0 indicates no explanatory power, while a value of 1 indicates that the model perfectly predicts the outcome variable. The Cox & Snell R Square was used to assess the proportion of variance explained by the model as a conservative measure. The – 2 log likelihood was used to quantify the probability of observing the data given the model’s parameters. A lower – 2 log likelihood indicates a better fit of the model to the data.
The significance level in all cases was considered as P≤0.05.
Results
Our results showed that 555 out of 615 studied infants (90.2%) had normal outcomes and 60 cases (9.8%) had abnormal outcomes among whom, 4 cases died during the follow-up and 56 cases were diagnosed with developmental delay. Sixty percent of the cases were boys and 40% were girls. A significant relationship was found between the serum sodium level and final outcome of the infants. This means that increased serum sodium level will lead to increased developmental delay; as, 8% of infants with serum sodium level of 151–160 mEq/L and 66.7% with serum sodium level of above 180 mEq/L had developmental delay at the age of two (Fig. 1).
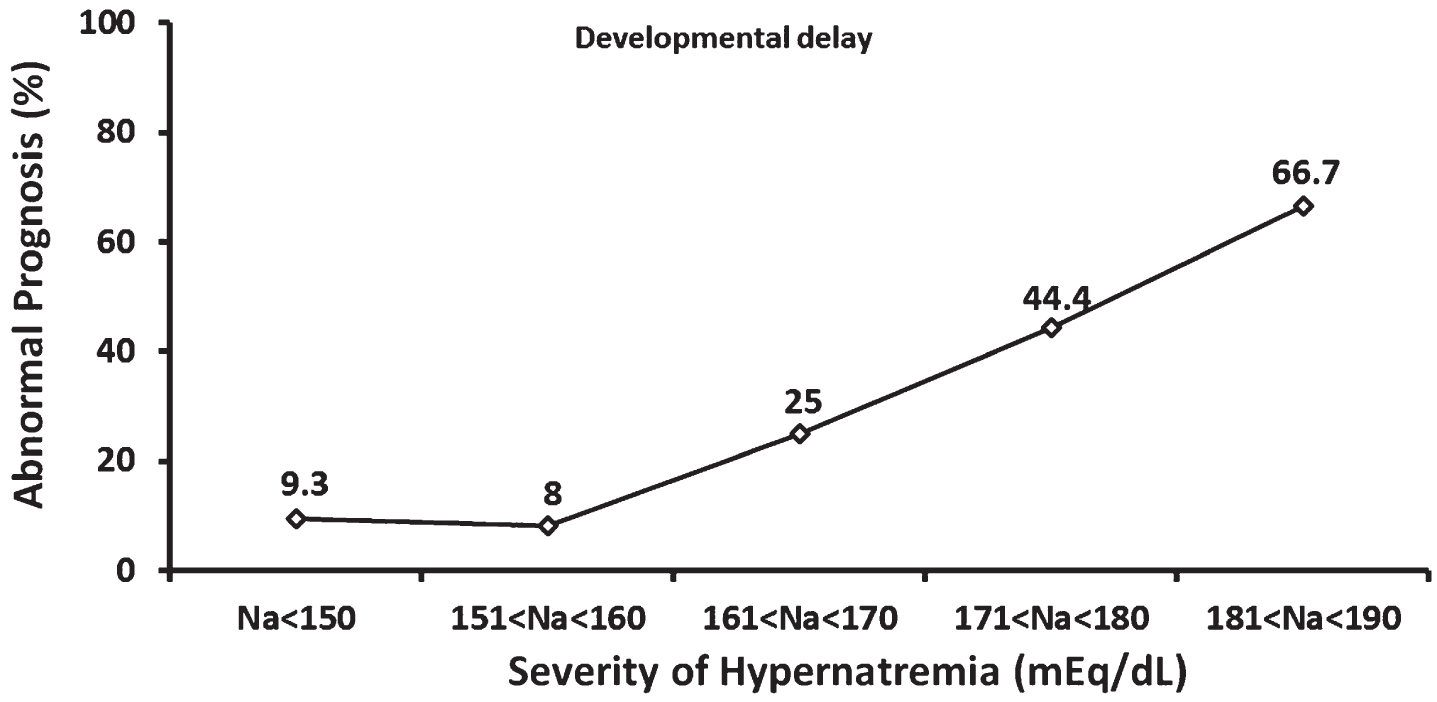
Percentage of abnormal prognosis (developmental delay) at the age of 2 years in infants with different hypernatremia severities. Na: sodium.
The significant relationship between the serum bilirubin level and final outcome of infants (P = 0.001) indicates that increased serum bilirubin level will lead to increased developmental delay (Fig. 2).
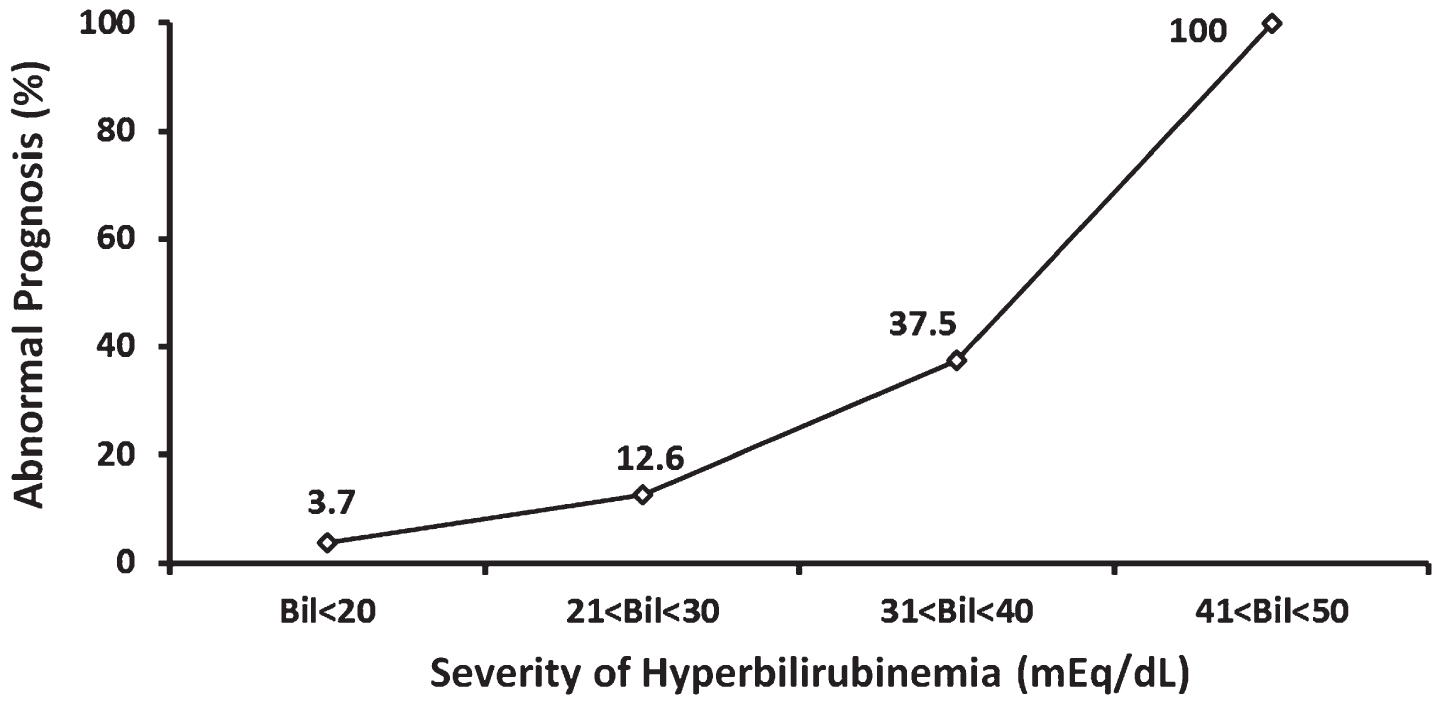
Percentage of abnormal prognosis (developmental delay) at the age of 2 years in infants with different hyperbilirubinemia severities. Bil: bilirubin.
Chi-square test also showed significant differences in the percentage of abnormal outcomes at the age of 2 years between various severities of combined hypernatremia and hyperbilirubinemia (P = 0.001) (Fig. 3).
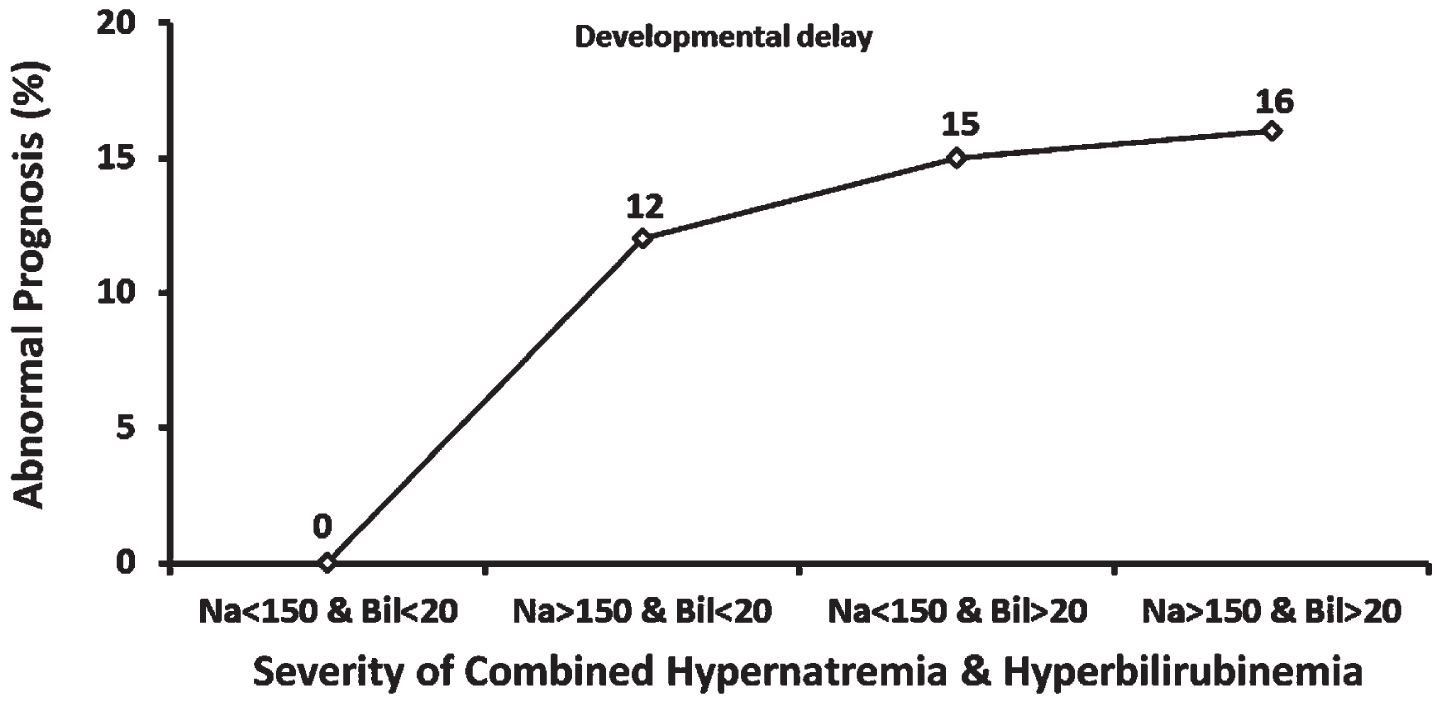
The incidence of developmental delay at 2 years old in different severities of combined hypernatremia and hyperbilirubinemia. Na: sodium; Bil: bilirubin.
Significant differences were seen in serum levels of sodium, bilirubin, urea, and creatinine between the children with and without abnormal outcomes (Table 1). This means that increased sodium, bilirubin, urea, and creatinine levels may raise the risk in infants with idiopathic jaundice with or without hypernatremia.
The overall comparison between the predictive variables of infants with and without normal outcomes
Infants with serum bilirubin levels above 25 mg/dL were found to be at an almost six times higher risk for development delays after two years. Also, Infants with serum sodium levels above 160 mEq/L were found to be at an almost three times higher risk for development delays after two years. Moreover, Infants with both bilirubin levels above 25 mg/dL and serum sodium levels above 160 mEq/L were found to be at an almost 17 times higher risk for development delays after two years (Table 2).
The risk ratios for high bilirubin and sodium based on Chi-square analysis
Regression models showed that bilirubin had a high predictive power (91.3%) in determining the unfavorable prognosis in idiopathic jaundice infants with or without hypernatremia (Table 3). however, hypernatremia, high creatinine levels, and hyperuricemia, respectively, had high sensitivity in predicting the complications (Table 1).
Comparison of the combination of sodium, bilirubin, in predicting unfavorable prognosis in idiopathic jaundice infants with or without hypernatremia
Na: sodium.
Our results suggest that jaundice and hypernatremia are factors to consider in brain development. Newborns with bilirubin levels over 20 mg may have high risk for developmental delay as newborns with severe hyperbilirubinemia.100% of infants with increased bilirubin level over 40 mg/dl, 40% with increased bilirubin level over 30 mg/dl, and 12% with increased bilirubin level over 20 mg/dl, were involved with developmental delay.
Neonatal jaundice has been shown to be associated with neurodevelopmental disorders [16]. It has been shown that an increase in mild neurological disorders in the first year of life may occur in healthy infants with a history of moderate hyperbilirubinemia [17]. The relationship between moderate hyperbilirubinemia in term infants and developmental delay has been shown to be significant [18]. The results of a study in a Kenyan village showed that severe neonatal hyperbilirubinemia (often with non-hemolytic causes) was associated with a high incidence of neurological and developmental disorders at 18–32 months [19]. Also, according to a two-year follow-up study on infants with hyperbilirubinemia and hypernatremia, about 90.2% of cases had normal outcomes and 9.8% had abnormal outcomes. Serum sodium, bilirubin, urea, and creatinine levels as well as clinical signs have shown important roles in determining the unfavorable prognosis in idiopathic jaundice infants with or without hypernatremia. Combination of variables such as sodium, urea, creatinine, lethargy, state of fontanels, convulsion, loss of consciousness, state of breast during postpartum, inverted nipple and brain CT scan has shown a high predictive power (98.6%) in determination of unfavorable prognosis in infants with hypernatremic dehydration [14].
Our study showed that hypernatremia worsens the neonatal prognosis. Increased blood osmolality followed by hypernatremia may cause cerebral damage with massive hemorrhage, clots, and subdural effusion that either leads to death or permanent nerve disorders. Infants with serum sodium levels above 160 mmol/l have been reported to be at high risk of neurodevelopmental disorders, seizures, and death [20]. Also, developmental delay has been shown to increase with enhanced severity of hypernatremia.
Hypernatremia may lead to disturbances in blood-brain barrier and result in the diffusion of bilirubin from the barrier and hence, increasing of the risk of bilirubin encephalopathy [21]. Our results showed that 20% of infants had a combination of hypernatremia and severe hyperbilirubinemia (bilirubin > 25 mg/dl). According to the results of our previous study, severe hyperbilirubinemia associated with severe hypernatremia occurs in 36.9% of infants which can be considered a hazardous clinical deterioration. This situation can lead to renal complications and long-term neurological outcomes. Hypernatremia can cause dysfunction in the blood-brain barrier, so, bilirubin can cross the barrier and increase the risk of encephalopathy [6].
The results of our study showed that the highest sensitivity in the prediction of developmental delay was related to serum bilirubin levels. Infants with mild and major disabilities have shown higher total serum bilirubin levels compared to those with normal neurodevelopmental outcomes. Also, term infants with a history of hyperbilirubinemia had delayed gross motor skills at the age of 6 months [22]. After severe hyperbilirubinemia, hypernatremia, high creatinine levels, and hyperuricemia, respectively, have high sensitivity in predicting the complications. Dehydration and prerenal azotemia can be seen in healthy infants who are hospitalized due to hyperbilirubinemia. Thus, measuring urea, creatinine, and blood electrolytes in infants with significant weight loss and hyperbilirubinemia is highly recommended [23]. A positive correlation has been seen between the serum sodium and urea or creatinine levels, while, there was a negative correlation between serum sodium and glucose levels of infants [24]. Hypernatremia complications occurred by increase in serum sodium level [25]. The results of our former study showed that if jaundice infants aged less than 10 days with a total weight loss of more than seven percent or with daily weight loss of more than 1.5 percent, serum sodium level must be checked. According to the direct relationship of serum sodium with serum urea and creatinine, if hypernatremic dehydration is diagnosed, they should be examined as well [26].
Conclusion
Our data showed that also hypernatremia is a factor to consider in neonatal prognosis; while combination of these two disturbances can intensify the developmental problems. However, the role of hyperbilirubinemia in the incidence of complications is superior to hypernatremia. In addition to high serum sodium and bilirubin levels, high serum urea and creatinine levels were also involved in determining the unfavorable prognosis in idiopathic jaundice infants with or without hypernatremia, but serum bilirubin level had the highest predictive power.
Therefore, considering the warning signs such as hyperthermia, jaundice, loss of consciousness, and reduced breastfeeding, early detection of hypernatremia and hyperbilirubinemia is necessary so that early and proper treatment can be performed. Considering the clinical symptoms, breast feeding position and laboratory examinations in suspected cases can be helpful in early diagnosis of hypernatremia and hyperbilirubinemia as well as reduction of unfavorable outcomes such as developmental delay. On the other hand, proper training of breastfeeding to mothers and enhancing their awareness about the benefits of breast milk as well as proper breastfeeding can reduce the risk of hypernatremia and severe hyperbilirubinemia and can lead to improvement of neonatal health.
Footnotes
Acknowledgments
This study was funded via Mashhad University of Medical Sciences.
Funding
We did not have any funding.
Conflict of interest
The authors declare no conflicts of interest.