
Abstract
Lymphatic malformations are rare benign developmental anomalies of the lymphatic system that can be diagnosed by prenatal ultrasound. Depending on their anatomical site and size, the lesions can cause a variety of aesthetic and functional deficits. Several treatment options are available, the most suitable is still under debate. The experience gained at our Centre and the review of the literature can be useful to improve prenatal counseling, that is challenging due to the heterogeneity of clinical presentation and treatment.
Introduction
Lymphatic malformations (LM) are rare benign lymphatic anomalies. Although in most cases these are small lesions of little clinical impact, depending on their site and size the medical implications can become significant. The rarity of such malformations, the variability of clinical presentation and the heterogeneity of possible treatments make prenatal counselling challenging. The aim of the study is to collect cases diagnosed prenatally at our Center, focusing on the prenatal ultrasound appearance and postnatal treatment. In addition, the purpose of the study is to review the literature on lymphangiomas to optimize prenatal counseling, providing the couple with updated and complete information.
Etiology
The etiology of LM is still unclear, but these lesions are thought to be an error in embryological development of the lymphatic system, on a multifactorial genetic basis. The lymphatic system derives from primordial endothelial buds sprouting from the developing venous system. These buds later coalesced into plexus and continuous channels. LM result from aberrant primordial buds that develop and fail to re-establish connections with the venous plexus from which they originated [1].
Incidence
The overall incidence is not exactly known, it is estimated to range from 0.008% to 0.18%, without gender differences [1, 2]. The real incidence might be underestimated because of the underreporting of medically or cosmetically insignificant malformations. LM frequently occur in lymphatic-rich areas. The cervico-facial region is the most common site (48–75%) but they can be seen in any anatomical region, in particular mediastinum, axilla, chest wall, groin, retroperitoneum [1, 3].
Classification
According to the International Society for the Study of Vascular Anomalies (ISSVA) classification [4], common LM are classified as macrocystic, microcystic or combined lesion, depending on the cyst size. There is no consensus definition or size cut-off, but the term macrocystic generally refers to a lesion greater than 1–2 cm and microcystic to a lesion smaller than 1–2 cm. Some authors define lesions with a prevalence (> 50%) of cysts greater than 2 cm of diameter as macrocystic, lesions that have no cysts larger than 2 cm as microcystic, and lesions with a prevalence (> 50%) of cysts less than 2 cm as combined [5]. The microcystic lesions have infiltrating characteristics, instead the macrocystic ones tend to compress and displace the surrounding structures without infiltration [6].
Clinical presentation
LM are evident in 50% of cases at birth and in 90% of cases within the first two years of life. However, they can potentially occur at any age [7].
Depending on their anatomical site and size, LM cause specific symptoms. There are several case reports in the literature describing the possible clinical manifestations associated with the different localizations. For example, when located at the cervical or mediastinal level these malformations can cause dyspnea or dysphagia due to ab extrinsic compression of the trachea and esophagus. When developed predominantly in the mediastinum, they can lead to vein compression with reduced venous return, heart compression or mediastinal shift that can lead to heart failure. In case of extensive growth in the prenatal period, they may cause pulmonary hypoplasia [8]. When LM are localized viscerally, whose main site is the small intestine followed by the mesentery, the most frequent clinical presentation is abdominal pain although in most cases the diagnosis is incidental [9]. As further examples, when located in the eye socket they may present clinically with ptosis, proptosis, ocular motility limitation, compressive optic neuropathy, and facial deformities [10], while near the joints they can cause reduced mobility and impaired ambulation. However, small uncomplicated lesions can be asymptomatic.
The spontaneous regression of lesions is a rare event, and should be considered as the effect of fibrosis secondary to inflammatory-infective complications. The progressive slow growth of lesions, proportionately with the size of the patient, is the most frequent phenomenon. The risk of progression increases during puberty or pregnancy due to estrogen-dependent changes. For this reason, some authors consider early treatment of even asymptomatic lesions indicated [11]. Not infrequently, the lesions may sharply increase in volume due to local inflammatory complications or intracystic haemorrhages for trauma or spontaneous intralesional bleeding, causing fever, pain and symptoms for compression of adjacent anatomical structures [6].
Diagnosis
LM can be diagnosed by prenatal ultrasound in 50–65% of cases [8]. The literature reports possible prenatal diagnosis starting from the 12th week [6]. The prenatal diagnosis of cervical or mediastinal lesions is crucially important since these lesions can lead to airway obstruction. The ultrasound visualization of the trachea and larynx is challenging, while prenatal MRI allows a better evaluation of airway and therefore the determination of the need for ex utero intrapartum therapy (EXIT). Thus, prenatal diagnosis can influence the mode, timing, and place of delivery improving the fetal prognosis.
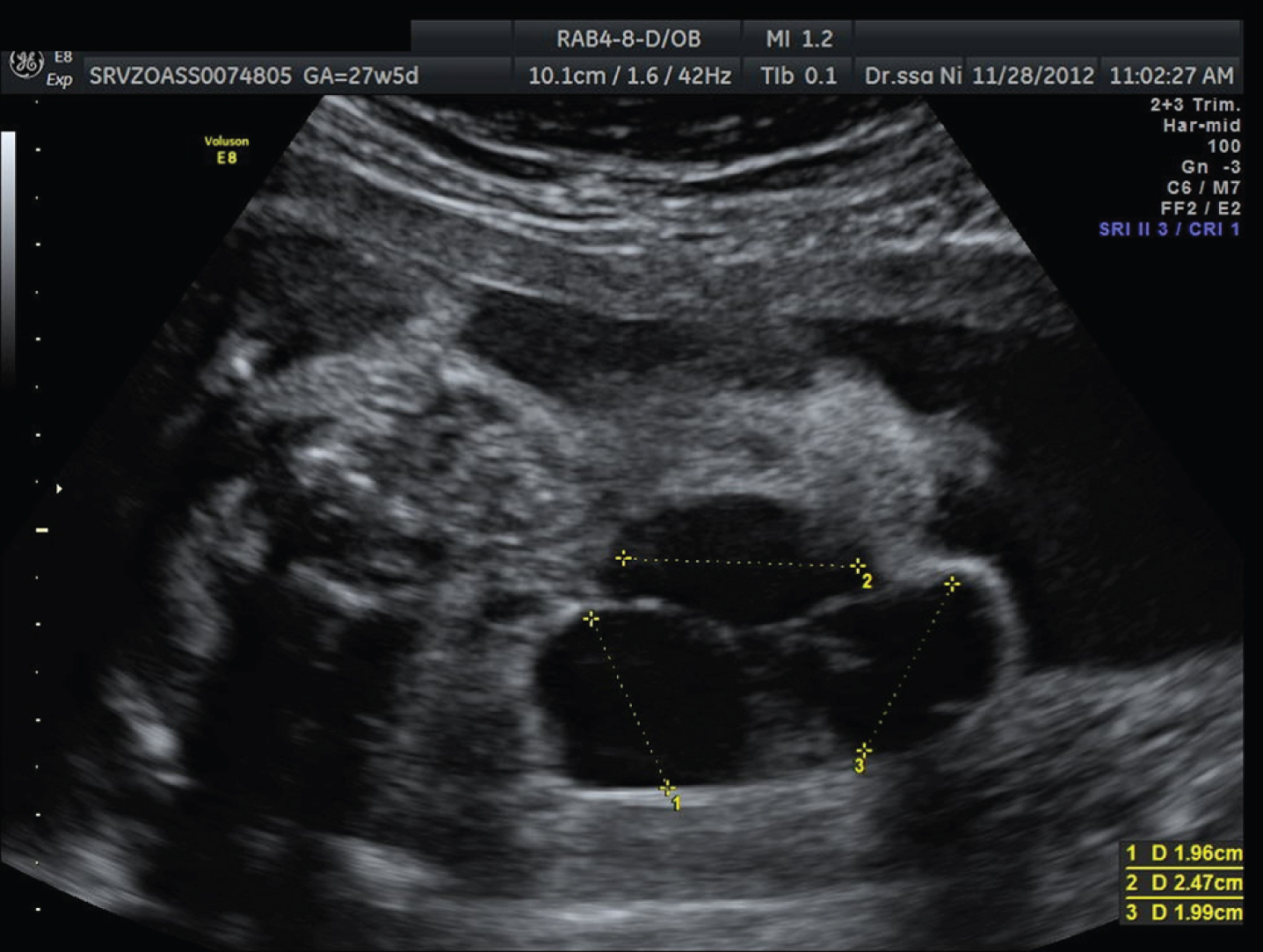
The typical prenatal ultrasound appearance is characterized by single or multiple anechoic cystic areas, giving the lesion a honeycomb appearance, without color flow on Doppler sonography, with a tendency to increase in size during the gestation [12]. Prenatal misdiagnosis is quite common. For example, mediastinal and chest wall LM should be differentiated from CPAM, cervical mono-LM should be differentiated from a pyriform cyst, celiac LM should be differentiated from ovarian cyst, intestinal duplication, retroperitoneal cystic teratoma, meconium peritonitis [8].
Post-natally, most cases are promptly diagnosed by physical examination. Macrocystic lesions are usually suspected on the basis of the presence of a soft, compressible or tense-elastic, painless swelling with undamaged overlying skin. Instead, superficial microcystic lesions have the appearance of oozing and bleeding vesicles. Deeper lesions could be suspected on the basis of compression symptoms of nearby organs or functional deficits [6]. The clinical diagnosis has to be confirmed by ultrasonography, which allows to evaluate the characteristics and extent of the malformation. MRI represents the second level diagnostic examination that can clearly demonstrate the relationship of the lesions with the deep tissues and organs and above all it allows to highlight areas of infiltration [1, 6]. The indication to perform a biopsy is limited to the rare cases in which instrumental investigations do not allow an adequate differential diagnosis [6]. Differential diagnosis, based on clinical appearance, localization, and imaging, should be done with cystic lesions such as dermoids, epidermoids, or ciliated cysts and with neoplastic lesions, such as teratomas, lipoblastomas, or rhabdomyosarcomas [3].
Treatment options
The best postnatal treatment is still debated. Complete recovery is often impossible, and the treatment goals are palliation of symptoms, reduction of functional deficits and aesthetic improvement. There are several therapeutic options: surgery, sclerotherapy, laser therapy, radiofrequency ablation and pharmacologic therapy (off-label). According to some Authors, surgery should be reserved for microcystic lesions, while sclerotherapy should be reserved for macrocystic ones [6].
Sclerotherapy involves the injection of some agents into the lesion inducing endothelial inflammation, thrombosis, occlusion, and fibrosis [1]. A number of sclerosing agents are used (like OK-432, sodium tetradecyl sulfate, bleomycin combined with dexamethasone), but it remains unclear which one is superior in terms of efficacy and safety [13]. OK-432 is a lyophilized mixture of group A Streptococcus pyogenes of human origin incubated with penicillin G that induces fibrosis by activating the Transforming growth factor-1. OK-432 can lead to complete resolution of LM in 50–90% of cases, with few complications (such as mild transient fever and local reaction) and less fibrosis of surrounding healthy tissue than other sclerosing agents [14, 15]. Sodium tetradecyl sulfate is an anionic detergent sclerosant that, at low concentration, induces coagulation and consequently fibrosis. Multiple treatments are usually required to achieve results. Adverse effects include only local reactions [16]. Bleomycin and dexamethasone injections can result in response rates close to 90 percent, with low recurrence rates. The sclerosing mechanism of bleomycin is not fully understood, nor is the synergistic action with dexamethasone currently known. The use of bleomycin requires caution because of the risk of pulmonary fibrosis at high doses [17].
Surgery is often limited by impossibility of radical excision due to the infiltrating nature of microcystic lesions leading to high relapse rate. The major complications of surgery are lymphorrhea, chylothorax, infections, bleeding, transient and permanent neurological damage [6].
Currently, most case reports indicate prenatal expectant management, but a few cases of in utero treatment have been reported. Prenatal drainage of voluminous lymphangiomas, proposed in some case reports before delivery to reduce the risk of mechanical dystocia [18], appears to be currently abandoned. Given the risks related with the EXIT procedure [19], prenatal treatment by intralesional injection of sclerosing agents into voluminous cervical or mediastinal LM has been proposed. Ultrasound-guided injection of OK-432 demonstrated progressive volumetric reduction of the lesion during pregnancy [20]. However, data are limited and need further study.
Case series
We have collected the cases of fetal LM diagnosed at our Department, between 2011 and 2021, in order to analyse their prenatal ultrasound features, obstetric management and, neonatal outcomes. The newborns were managed at the Pediatric Surgery Department of the same hospital. A total of six cases were identified during the study period.
Data were retrieved from medical records and from an electronic database (Viewpoint version 5, GE Healthcare, Munich, Germany) which collects information about pregnancy, ultrasound examinations, delivery and neonatal outcomes.
Case 1: Right laterocervical LM
In a 27-year-old woman at her first pregnancy, with a low-risk cf-DNA test, a voluminous right posterolateral cervical neoformation measuring 66×60×50 mm, with thickened walls and mixed cystic-solid content without significant vascular component, was identified at 31 + 2 weeks of gestation (Fig. 1). Fetal MRI confirmed the diagnosis and ruled out significant airway compression. During prenatal follow up, there was a slight increase in size, mainly exophytic. At 37 + 6 weeks of gestation, a cesarean section was performed and the newborn appeared healthy. After birth, two injections of a sclerosing agent (3% sodium tetradecyl sulfate) were performed with significant clinical improvement.

Right laterocervical LM.
In a 37-year-old woman, gravida 3 para 0, with a monochorionic diamniotic twin pregnancy, a multiloculated, nonvascularized, 37×14×48 mm left chest wall neoformation and bilateral club foot was diagnosed in one fetus at 20 + 5 weeks of gestation (Fig. 2). The other fetus was normal. A fetal MRI confirmed the diagnosis, excluding thoracic cavity invasion. Karyotype and array-CGH were normal. At 33 + 5 weeks of gestation, a cesarean section was performed for nonreassuring cardiotocography in the setting of twin-to-twin transfusion syndrome. The affected infant (recipient twin) was intubated at birth. Three sclerotherapies with 3% sodium tetradecyl sulfate were performed over the following three months, with significant regression of lesion size.

Left chest wall LM in a twin pregnancy.
In a 33-year-old woman, gravida 2 para 1, a biloculated cystic mass in the temporal and laterocervical site was identified at 20 + 6 weeks of gestation. The lesion measured 43×22×26 mm and was related to the right eye socket (Fig. 3). Karyotype and array-CGH were normal. A destructive effect on cranial bone structures was identified at 22 + 3 weeks of gestation. The pregnancy was terminated by intracardiac KCl injection. Autopsy confirmed the prenatal diagnosis.

Temporal LM involving right ocular orbit.
A 38-year-old woman, gravida 4 para 2, was diagnosed at 20 + 6 weeks of gestation with a 29×26×19 mm fetal multi-chamber cystic formation located below the right mandibular branch with a central vasculature originating from the right superficial carotid artery (Fig. 4). Fetal MRI confirmed the diagnosis and excluded upper aerodigestive tract compression. The karyotype was normal. The size increased during pregnancy. At 38 weeks of gestation an elective cesarean section was performed and the newborn was healthy. Four percutaneous sclerotherapies with OK-432 were performed during the first year of life, with partial size reduction and functional improvement.
Laterocervical LM involving parotid and submandibular regions.
A 22-year-old woman, gravida 2 para 1, was diagnosed with a voluminous fetal LM of the right thoraco-abdominal wall (110×90×135 mm) during the second trimester screening scan (Fig. 5). The patient was referred to our center in the third trimester. The size of the lesion remained stable during follow up, the neck appeared uninvolved. At 37 + 4 weeks of gestation a cesarean section was performed, and the infant was healthy. Post-natal MRI also showed an extension to the right upper limb (Fig. 6). In the first six months of life, three sclerosing treatments with 3% sodium tetradecyl sulfate were performed with good results on the macrocystic components (Fig. 7). Due to a widespread microcystic components, experimental systemic therapy with Ripamycin was attempted.
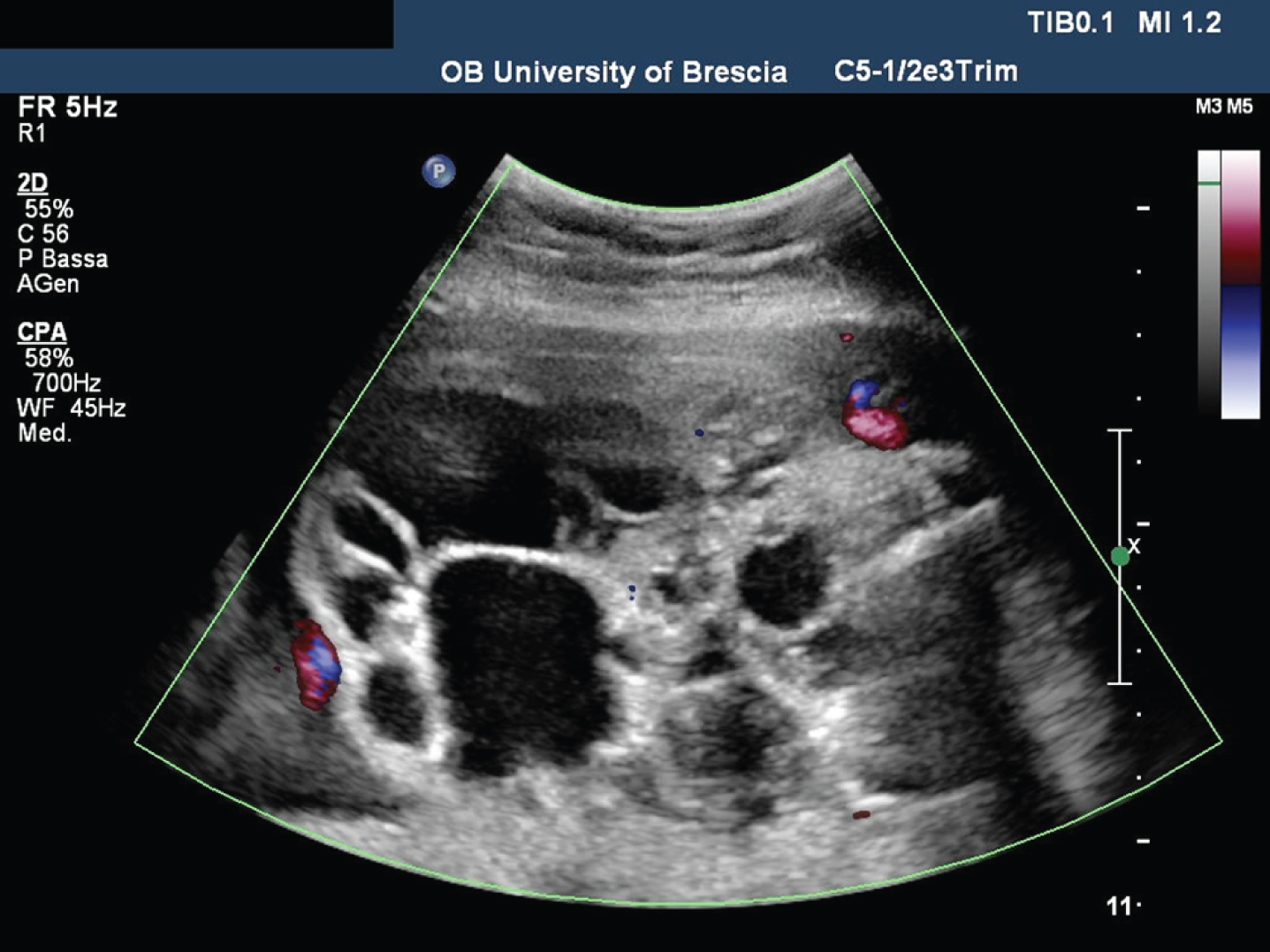
Voluminous LM of the right thoraco-abdominal wall.

Post-natal MRI showing two large bilateral hemolymphangiomas of the chest wall. The right lesion extends to the axillary region and the upper limb.
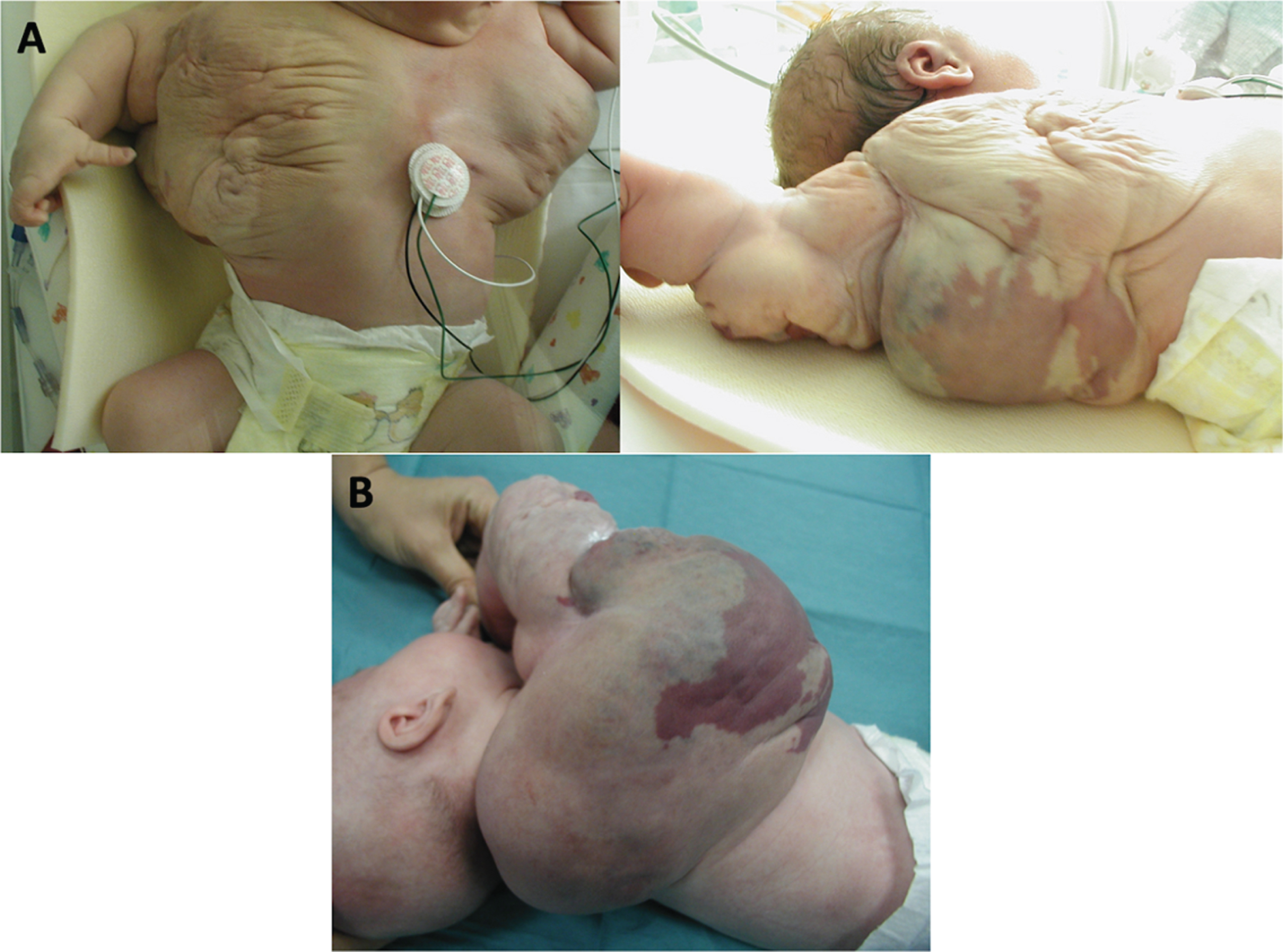
A: Lesions apperance at birth. B: Partial improvement of the lesions after the initial sclerosing treatment.
A 25-year-old primigravid was diagnosed with a bilateral fetal hydrothorax and left mediastinal solid-cystic neoformation at 32 weeks of gestation. The lesion extended to the neck, marking the pharyngeal wall, and LM was suspected (Fig. 8). Fetal MRI showed almost complete compression of the aerodigestive tract with contralateral displacement. At 37 weeks of gestation an elective cesarean section with EXIT procedure was performed. The newborn was intubated and four days later a tracheostomy was performed (removed 14 months later) and a PEG was placed (removed 26 months later). Four sclerotherapies, with 3% sodium tetradecyl sulfate and OK-432, were performed in the first four months of life, with marked improvement. At three years of life, clinical development was good, without need for further sclerotherapy.

Cervico-mediastinal LM associated with bilateral fetal hydrothorax, that required EXIT procedure because of airway compression.
Our case series confirms the rarity of these malformations and the heterogeneous clinical presentation. Probably because of these features and the low rate of prenatal diagnosis, to the best of our knowledge there are no randomized clinical trials in the literature, only case reports and small retrospective studies.
The lesions in our cohort were located at several sites, with a slight prevalence for the cervical and laterocervical regions. Indeed, in accordance with the literature, LM frequently occur in lymphatic-rich areas, and the cervico-facial region appears to be the most common site [1, 3]. The neoformations presented the same solid-cystic pluri-chambered ultrasound appearance, in the absence of vascularization. In addition, they showed a tendency to increase in size during follow up. The ultrasound identification of deep infiltration and airway obstruction appeared challenging. According to the literature, fetal MRI seems useful to better define the relationship of the lesion with the aerodigestive tract [21], so it was performed in all the cases who carried pregnancy to term, except one who referred to our center only in the advanced third trimester. The recognition of any compression or infiltration of the great vessels, airways or digestive tracts is essential. Indeed, correct and early diagnosis can allow optimal definition of the timing and mode of delivery and planning of postnatal interventions. Due to prenatal identification of airway obstruction, case 6 underwent an EXIT procedure that allowed neonatal survival with good outcome.
In all the cases where the karyotype was performed, it was normal. Usually, LM appear as isolated malformations with normal karyotype [22–24], but karyotyping is generally recommended in the literature [6]. Further genetic investigations are not currently possible, as the presentation is sporadic, multifactorial and free from inheritance. In our case series, no associated fetal abnormalities were found except for one fetus with bilateral clubfoot, however in the context of a monochorionic diamniotic twin pregnancy.
Delivery in a tertiary care center with pediatric surgery is recommended if emergency surgery may be necessary. In all cases we performed an elective cesarean section. It appears to be the most suitable mode of delivery, except for small and not clinically significant malformations. Large lesions could complicate vaginal delivery with mechanical dystocia, fetal malposition, abnormal presentation, and fetal trauma [23, 25]. Currently, there is no evidence in the literature that planning delivery before 37 weeks is beneficial. When a high risk of airway compression is recognized, the EXIT procedure should always be considered. This procedure, performed by a multidisciplinary team of obstetricians, anesthesiologists, pediatric surgeons, neonatologists, and otolaryngologists, allows satisfactory access to the airway by intubation or tracheostomy while the fetus is still oxygenated by the placenta. This procedure allows fetal protection from acute hypoxia and brain damage [26].
Several treatment options are proposed in the literature, the most suitable one is still debated also in relation to the wide diversity of therapeutic response between microcystic and macrocystic lesions [27]. In our cohort, infants were treated with multiple sclerotherapy (3% sodium tetradecyl sulfate or OK-432) of macrocystic lesions, with significant cosmetic and functional improvement. The most commonly used sclerosing agent at our Center is 3% sodium tetradecyl sulfate because of its low and predominantly local toxicity. The first injection was generally performed in the first two weeks of life, and the following within the first few months of life. In only one case, in consideration of the widespread microcystic components, the inclusion in an experimental protocol with Ripamycin following sclerosing therapies was opted for [28]. In this case, the suspicion that it may be a CLOVES Syndrome or a PROS (PIK3CA-related overgrowth spectrum) is high, so investigations are ongoing.
In conclusion, LM are benign lesions whose localization and size are essential to predict clinical outcome. They can be disabling pathologies with significant functional, aesthetic, and psychological impact. Specialist care in referral centers with multidisciplinary management is suggested, both in the prenatal phase, with appropriate counseling and targeted diagnostic investigations, and in the postnatal phase, ensuring access to neonatal intensive care and urgent surgical treatment. Currently, there is no shared treatment protocol and above all there is no curative treatment. The therapeutic goal is to improve patients’ quality of life by reducing functional and cosmetic impact. It must be clearly explained to parents in order to set realistic expectations. In our experience, the use of conservative sclerosing therapies was associated with good clinical outcomes in most cases. The experience gained at our Centre can be useful in order to improve prenatalcounseling.
Disclosure
The authors declare that the research was conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration.
The authors have no conflicts of interest.