
Abstract
An infant with a corrected gestational age of 38 weeks, weighing 3.1 kg, was referred to our pediatric surgical department because of a fractured peripherally inserted central venous catheter in the left lower limb with the end retracting into the deep venous system. An operation was undertaken to remove the PICC. Because the central venous catheter was, unintentionally, placed in the left small saphenous vein and thus positioned in the left femoral vein, the left great saphenous vein was incised to gain access. Subsequently, the catheter could be removed successfully. Fracturing of a peripherally inserted central venous catheter is a rare occurance. Removal depends on vessel size, location and experertise.
Keywords
Introduction
Patients at the neonatal intensive care unit (NICU) often require placement of a peripherally inserted central venous catheter (PICC), enabling the administration of fluids, parenteral nutrition, and medication. Removal rarely poses any difficulties. Nevertheless, the PICC may sometimes resist removal and with simple maneuvers (warm packing or sterile soaks, rotation of the line, gentle traction, repositioning of the limb or massaging the limb) this procedure is ultimately successful [1–3]. However, in 1 to 10% of cases, a PICC may fracture during difficult removal and the retained part retracts deep into the limb requiring radiologically guided or surgical removal [4–6]. Here, we describe a case of a patient in whom the PICC fractured and retracted into the deep venous system, which was surgically removed.
Case
A boy was born after cesarean section due to deterioration of fetal status at a gestational age of 27 weeks and 5 days. Birth weight was 845 gram (below the 2nd percentile for gestational age). There were no congenital abnormalities. NICU admission was complicated by respiratory distress syndrome, treated with surfactant, mild BPD and coagulase negative staphylococcus sepsis, from which he recovered well. He was discharged home at a gestational age of 36 weeks and one day. At 38 weeks and 6 days postmenstrual age and weighing 3.1 kg he was readmitted to the NICU due to respiratory insufficiency caused by respiratory syncytial virus bronchiolitis with bacterial superinfection. He required intubation, fluid support and antibiotic treatment. Therefore, a 1 French peripheral intravenous central catheter (Lifecath PICC, Vygon, NL) was thought to be placed via the left great saphenous vein, positioning the tip deep in the left external iliac vein, with the Seldinger technique. Placement was uncomplicated and the PICC functioned well throughout his clinical course (Fig. 1). After recovery and extubation, it was attempted to remove the PICC, 13 days after placement. However, the line resisted traction at repeated attempts by different physicians. Therefore, gentle and increasing traction was exerted in order to remove the line. Ultimately, the line fractured with the end retracting into the limb. A control X-ray suggested that the line had been positioned in the popliteal vein with the tip in the external iliac vein. An indication for surgical removal was made and the patient was transferred to an academic center for pediatric surgical consultation.
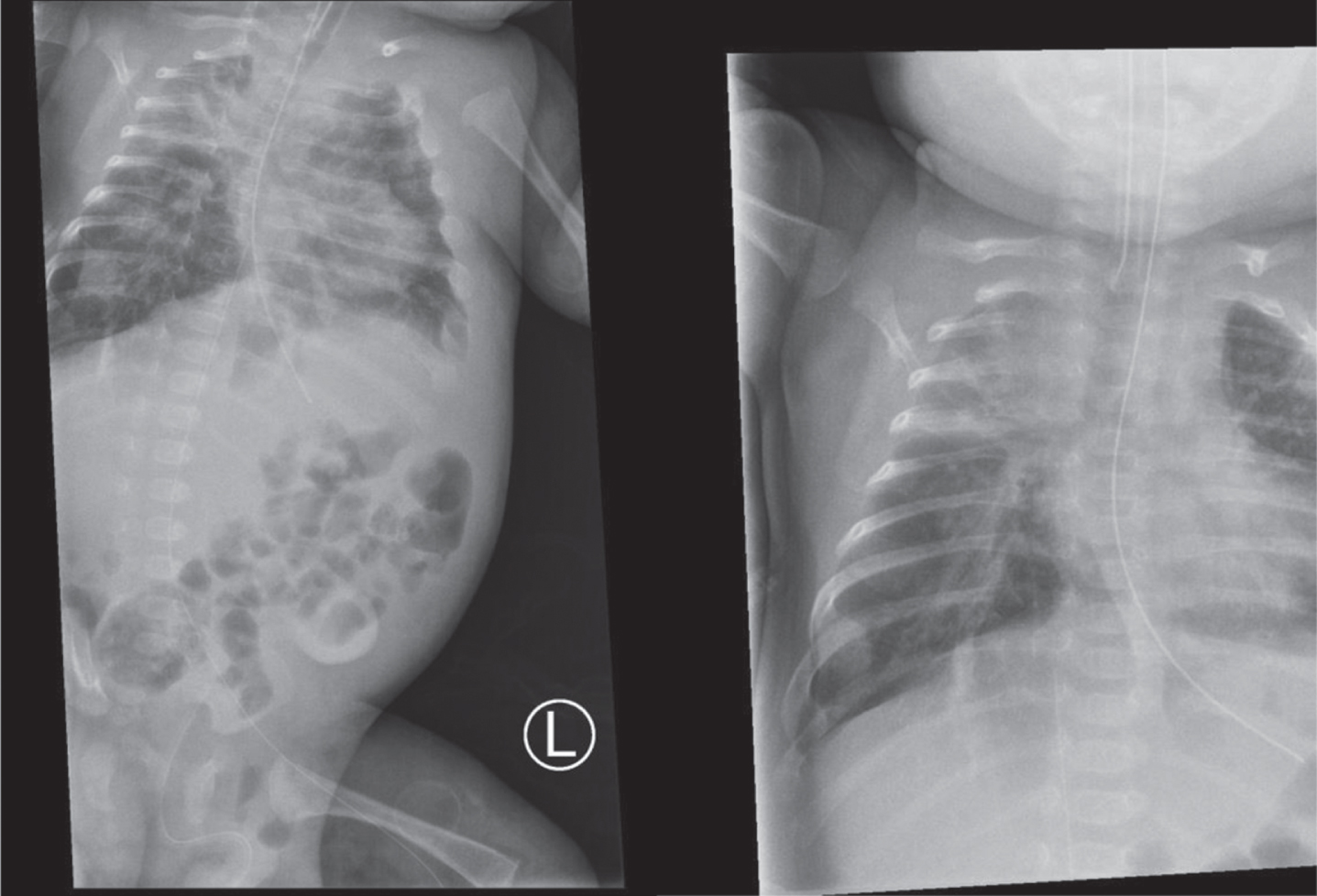
X-ray after placement, evaluting the positioning of the peripherally inserted catheter showing a deep position of the tip (left panel), after which it was repositioned (right panel).
A repeat X-ray showed an unchanged position of the line (Fig. 2). Next, the patient was transferred to the operating theatre. While under general anesthesia, an ultrasound was performed to determine the location of the PICC. As the X-ray suggested, the PICC was in the left popliteal and ileac vein, confirming that the line was placed unintentionally via the left small saphenous vein, instead of the great saphenous vein. Exploration at the popliteal level was thought to provide inadequate exposure with an increased risk of neurological damage, occlusion of the popliteal vein with possible thrombus formation and/or lower leg ischemia [7]. It was subsequently decided to remove the PICC via the great saphenous vein, believing that it would provide easier access with lower risk of complications. Subsequently, a longitudinal incision from the level of the inguinal ligament through the groin fold was made. Beyond the subcutaneous tissue and fat, the common femoral vein was dissected and isolated with vessel loops. Additionally, the great saphenous vein was identified and isolated as well (Fig. 3). Instead of incising the common femoral vein, possibly causing endothelial damage or resulting in a stenosis after closure, a small transverse incision was made in the great saphenous vein just before its entry into the common femoral vein. From here the PICC could be removed from the deep system with a micro forceps. Upon removal, no resistance was detected. The incision of the great saphenous vein was closed with a 7.0 prolene. After removal, a fibrin sheath was observed adhering to the PICC. Long-term follow-up was uneventful.

X-ray of the left lower limb showing the peripherally inserted catheter, which projects over the popliteal and femoral veins.
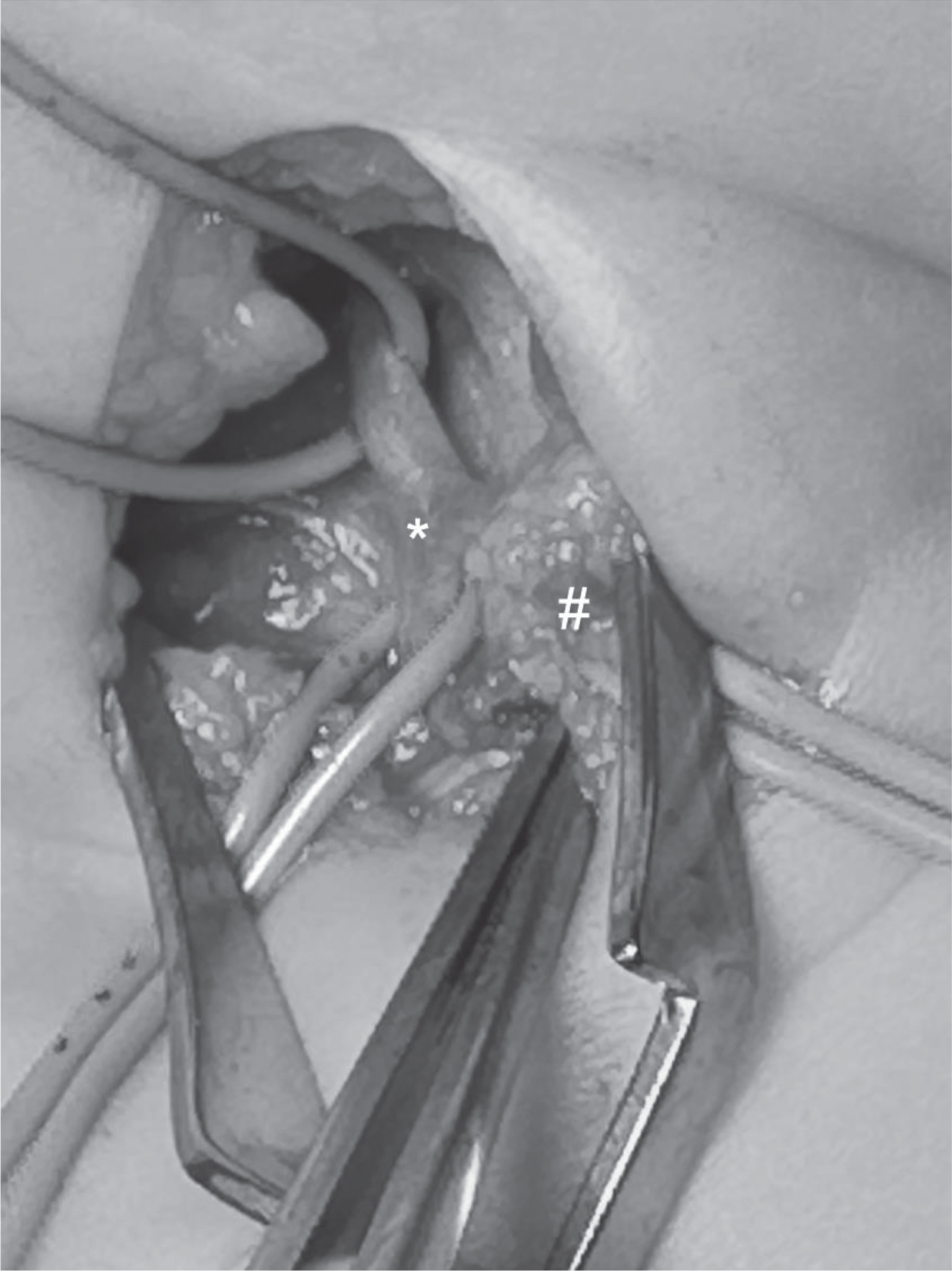
The femoral vein is dissected and isolated proximally and distally with loops (*) and the great saphenous vein showing laterally (with some overlaying fatty tissue; #).
Placement of a PICC is commonly performed at any NICU. Removal usually is uneventful. However, although very infrequent, entrapped or even fractured PICCs have been reported [4, 8]. In case of an embolized catheter, immediate action is required to prevent further complications [9]. To our knowledge, this is the first report that describes surgical removal of a fractured PICC, gaining access to the femoral vein through an incision of the inguinal fold and groin.
The mainstay of PICC patency involves a correct insertion technique according to the manufactures’ instructions by an experienced physician and subsequent proper nursing care for catheter handling, changes of the dressings, infusion policy, and so on [10]. Furthermore, important causes for fracturing have been suggested to be vasospasm, fibrin sheath or thrombus formation, and or adhesions resulting from infection. Even knots have been described to cause resistance to removal [11]. In the present case, a fibrin sheath was seen covering the line. This may have caused adhesion to the vessel wall, or the thickening creating a mechanical obstruction that prevented its passage through the junction of the small saphenous vein into the popliteal vein. However, a real causal relation is difficult to prove.
Removing an entrapped PICC can be achieved with some simple maneuvres. Warming the limb with packs or soaked gauzes is thought to cause dilation of the vein diminishing vasospams. By gradually increasing traction, the line may loosen from the wall and eventually yield. Massaging or repositioning the limb may be sufficient to move a possible fibrin plug beyond a narrow venous segment or release adhesions to the vessel wall [2, 4]. Even with all these measures there is still a possibility that the PICC cannot be extracted and even break under to much tension.
Reported fracture rates range from 1% to 10% [4]. When the catheter embolizes into the vessel an emergent intervention should be undertaken to prevent it from embolizing the heart. There are limited reports on the techniques for removal. Overall, options can be dived into radiologically guided endovascular retrieval and surgery. Two cases have been reported on the removal of a fractured central venous catheter initially placed in the leg. Watkin and Stephenson elobarated on a catheter placed in the right great saphenous vein that embolized to the pulmonary artery. Eventually, a sternotomy was required after unsuccessful cardiac catheterisation [12]. Hsu and collaegues described the succesful endovascular retrieval with a snare of a central catheter initially place in the left femoral vein and, after fracturing, dislodged into the ileac vein and superior vena cava [13]. Endovascular retrievel uses any vein that will allow most adequate access to the catheter such as the femoral or basilic vein [11, 14], or even the umbilical vein if still patent [15]. In addition to the embolization of the catheter to the heart, endovascalur removal itself is not without complications either [16]. In general, the specific surgical procedure will depend on the anatomical location of the catheter [17, 18]. Patient factors, anatomy, experience of the clinicians, availability of equipment, and so on, will likely guide the final choice for the procedure.
Here, we presented a case where a central venous line was unintentionally positioned in the smaller saphenous vein. After fracturing, imaging revealed that it was positioned in the left popliteal and femoral vein. Thereafter, several options had been considered. Since there was no experience with endovascular retrieval in these small calibre vessels, it was decided to perform an operative apporach. However, directly accessing the popliteal vein was thought to entail the risk of damaging the adjecent popliteal nerve and/or popliteal artery [7]. Because the great saphenous vein could be sacrifced if needed, it was chosen to perform an incision of the groin, incise this vein and from there easily retrieve the line from the femoral vein.
Fracturing of a PICC seldomly occurs, but requires swift removal to prevent further harm. To our knowledge, this is the first report of an surgical removal of a PICC dislodged into the femoral vein. Ultimately, each case will require an individual approach directing the most adequate choice of treatment.
Funding
None.
Footnotes
Acknowledgments
None.