
Abstract
Introduction
both groups (NEMS group: fromStroke-related muscle wasting is one of the factors leading to long-term disability and functional dependency among stroke survivors (Scherbakov & Doehner, 2011; English, McLennan, Thoirs, Coates, & Bernhardt, 2010; Scherbakov, von Haehling, Anker, DirnaqI, & Doehner, 2013; Scherbakov, Sandek, & Doehner, 2015). Studies regarding pathophysiological mechanisms for stroke-related muscle wasting, such as inactivity, denervation, malnutrition, inflammation, and metabolic imbalance, have been published (Scherbakov & Doehner, 2011; English et al., 2010; Scherbakov et al., 2013; Scherbakov et al., 2015). However, the mechanism underlying muscle wasting is unclear, and an effective therapeutic intervention for muscle wasting has not beenfound.
Muscle wasting particularly in the lower leg of stroke patients is often observed in the acute phase (Jørgensen & Jacobsen, 2001; Nozoe et al., 2016). Many studies have been conducted to attempt to prevent leg muscle mass wasting by using several methods (Zou, Wang, Qu, & Wang, 2015; Ryan, Ivey, Prior, Li, & Hafer-Macko, 2011). Neuromuscular electrical stimulation (NMES) is one of the interventions to prevent muscle wasting for patients with several diseases (Yavuzer et al., 2006; Mesci, Ozdemir, Kabayel, & Tokuc, 2009; Gerovasili et al., 2009; Segers et al., 2014; Maffiuletti NA, Roig M, Karatzanos, & Nanas, 2013; Kho et al., 2015). Yavuzer et al. (2006) and Mesci et al. (2009) studied the efficacy of NMES for stroke patients; however, they investigated sub-acute or chronic stroke patients, and the effects on muscle mass were not shown. Other studies have shown the feasibility and efficacy of NMES for patients with critical illness (Gerovasili et al., 2009; Segers et al., 2014; Maffiuletti et al., 2013; Kho et al., 2015; Fischer et al., 2016), chronic obstructive pulmonary disease (COPD) (Maddocks et al., 2016), and heart failure (Gomes Neto et al., 2016). Gerovasili et al. (2009). and another systematic review (Maffiuletti et al., 2013) showed the positive effect of NMES on muscle mass, although the recent study could not show the positive effect on muscle strength or muscle mass in patients with critical illness (Kho et al., 2015; Fischer et al., 2016). Maddocks et al. (2016) also showed positive effects in patients with COPD, but other systematic reviews concluded that NMES has positive effect for patients with heart failure (Gomes Neto et al., 2016). Thus, the researchers were unable obtain certain results in various population, and no study has been conducted in patients with acute stroke.
The purpose of this study was to investigate the efficacy of NMES for preventing quadriceps muscle wasting in patients with moderate or severe acute stroke.
Material and methods
Participants
We enrolled consecutive patients during two phases (from June to October 2014 and from June to October 2015) with acute ischemic and hemorrhage stroke less than 48 h from onset who were admitted to Itami Kousei Neurosurgical Hospital and those who were <85 years old. The definitive diagnosis of stroke was made by an experienced stroke neurologist based on clinical characteristics and neuroimaging. Treatment with recombinant tissue plasminogen activator and endovascular thrombectomy was also allowed. Patients with premorbid modified Rankin Scale (mRS) score≥3, with National Institute of Health Stroke Scale (NIHSS) score <8 upon study enrollment, with other neuromuscular or musculoskeletal disease, cardiopulmonary dysfunction, severe renal dysfunction that influenced physical function, and those who declined to participate in this study (who were uninterested or felt too unwell) were excluded. Patients who were admitted from June to October 2014 and from June to October 2015 were assigned to the control and intervention groups (NMES group), respectively. The study was approved by the Itami Kousei Neurosurgical Hospital Research Ethics Committee. All participants or nominated representative provided informed consent.
Measurement of quadriceps muscle thickness
For all patients, quadriceps muscle thickness was evaluated with ultrasound (US), by measuring the cross-sectional diameter of the quadriceps muscle (rectus femoris–vastus intermedius) on the day the patients provided informed consent (within five days of admission) and 14 days after the first measurement. All measurements were conducted with B-mode US imaging (LOGIQ P5, GE Healthcare Japan, Tokyo, Japan) with an 8-MHz transducer. Measurements were conducted with the subjects in the supine position, with hips and knees extended, and the center of the transducer was positioned on the short axis midway between the anterior superior iliac spine and the midpoint of the proximal end of the patella (Fig. 1) (Ikezoe, Asakawa, Fukumoto, Tsukagoshi, & Ichihashi, 2012). All measurements were performed by the same sonographer. This technique has been shown to have excellent reproducibility (English CK, Thoirs KA, Fisher, McLennan, & Bernhardt, 2012). Excess gel was applied to prevent impression of the skin. The position of the probe was marked to standardize the follow-up measurements.

The position of the electrodes on the quadriceps muscle and measurement point of ultrasound images in quadriceps muscle thickness. The arrow shows the determination of the measurement point.
NEMS was applied to the quadriceps muscles of both lower extremities 5 to 6 days a week from the day of the first measurement for muscle mass in the NMES group. The skin was carefully shaven before the application. Rectangular electrodes (90×50 mm) were positioned on the quadriceps muscles of both legs (Fig. 1) (Segers et al., 2014). The stimulator (ESPURGE, Ito Co., Ltd, Tokyo, Japan) delivered biphasic, symmetric impulses of 50 Hz, 300-μs pulse duration, 12 s on and 6 s off, at intensities able to cause visible contractions and maximal intensity that the subject can tolerate (range, 20 mA–50 mA). The session lasted for 50 to 60 min.
Rehabilitation program
All patients received 40 min–60 min of physiotherapy, which consisted of mobilization, gait exercise combined with orthotic therapy, and conventional rehabilitation approaches to improve the patients’ independence five times per week. Our physiotherapy also included early rehabilitation (starting mobilization within 1 week from admission). The time to first mobilization was determined by the physician to match each patient condition. Daily individualized occupational therapy and speech and language therapy were prescribed to participants on an as-needed basis.
Other measurement procedures
We evaluated patient characteristics, including age, sex, hemiparesis side, Oxfordshire StrokeClassification, comorbidity, time to first mobilization from onset, time to first measurement from onset, serum albumin level, and body mass index (BMI) on admission. The NIHSS was also evaluated on the day of inclusion.
Statistical analysis
All data are presented as mean±standard deviation. The within-patient changes were evaluated with the Wilcoxon signed-rank test. The differences between patients were evaluated with a nonparametric test (Mann-Whitney U test) or chi-square test. A P value of <0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS 20.0J® statistical software (IBM, Chicago, IL, USA).
Results
Study population
Of 193 patients diagnosed with acute stroke who were <85 years old and admitted to the hospital (90 and 103 patients in the control and NMES groups, respectively), 7 and 5 patients were excluded because the premorbid mRS score was≥3; 66 and 77 patients were excluded the NIHSS was <8; 2 and 5 patients were excluded because they declined participation; and 1 and 2 patients were excluded because of other diseases that influenced physical function, respectively. Finally, 28 patients (14 patients in each group) satisfied the inclusion criteria; however, four patients in each group were excluded because of several reasons (Fig. 2). Finally, we analyzed 10 patients in each group.
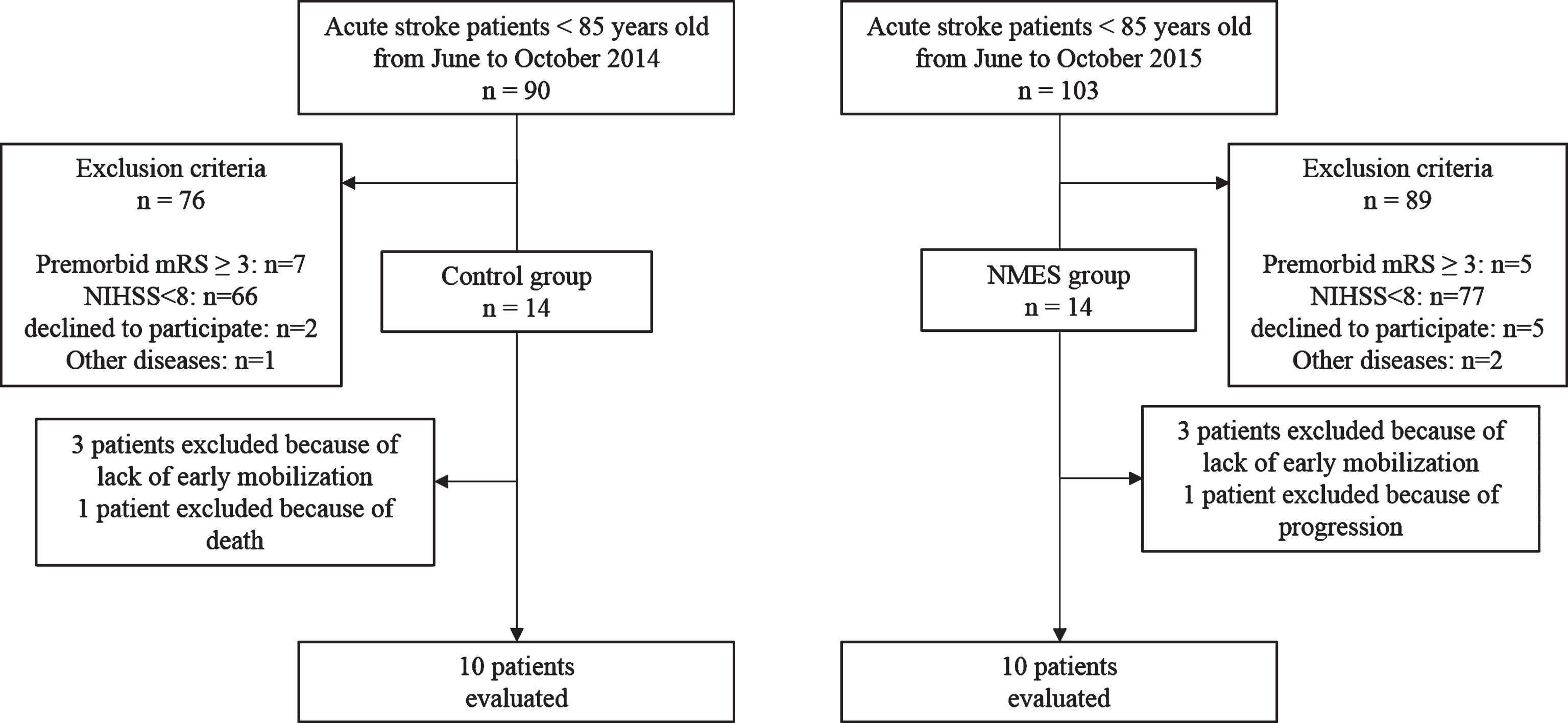
Flow diagram of patient recruitment to the study. NMES, neuromuscular electrical stimulation.
Baseline characteristics of subjects in the control or NMES group are presented in Table 1. No significant differences were found for age, BMI, duration from admission to first mobilization, serum albumin level, and NIHSS score between groups; however, significant differences were found within the time to first measurement from onset. In the control group, two and one patient underwent thrombolysis and craniotomy, respectively, and in the NMES group, two and two patients underwent thrombectomy andcraniotomy, respectively.
Baseline characteristics of subjects in the control or NMES group (mean±SD)
Baseline characteristics of subjects in the control or NMES group (mean±SD)
BMI: body mass index; LACI, lacunar infarct; NIHSS, National Institute of Health Stroke Scale; NMES, neuromuscular electrical stimulation; PACI, partial anterior circulation infarct; POCI, posterior circulation infarct; TACI, total anterior circulation infarct.
The quadriceps muscle thickness on the paretic side decreased in both groups (NEMS group: from 3.06±0.69 cm to 2.71±0.79 cm, P = 0.02; control group: from 3.07±0.60 cm to 2.20±0.68 cm, P = 0.005) (Table 2). The quadriceps muscle thickness on the non-paretic side decreased only in the control group (NEMS group: from 3.20±0.85 cm to 2.97±0.72 cm, P = 0.17; control group: from 3.29±0.59 cm to 2.62±0.92 cm, P = 0.005) (Table 2). The quadriceps muscle thickness on the paretic and non-paretic sides in the NMES group (–12.4% ±12.7%, –5.5% ±15.3%, respectively) significantly decreased to a lesser degree than that in the control group (–29.5% ±12.1%, P = 0.004; and –22.0% ±16.8%, P = 0.04, respectively) (Fig. 3).
Quadriceps muscle thickness in the control or NMES group (mean±SD)
Quadriceps muscle thickness in the control or NMES group (mean±SD)
NMES, neuromuscular electrical stimulation.
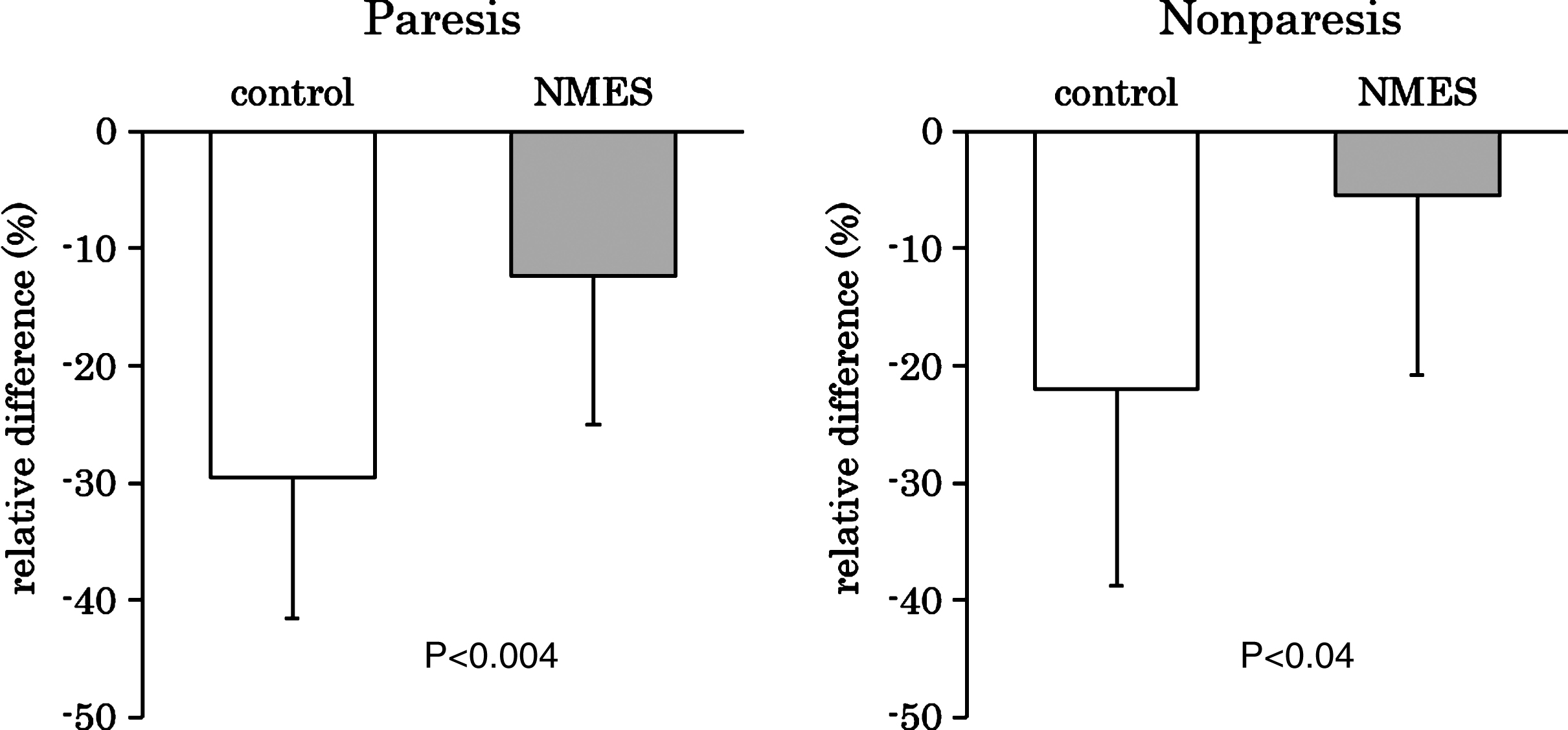
Relative difference (%) in quadriceps muscle thickness of the paretic or nonparetic limb in the control and NMES groups (mean±standard deviation). NMES, neuromuscular electrical stimulation.
This study examines the efficacy of NMES on quadriceps muscle wasting in patients with acute stroke during hospitalization. Our results show that NMES could prevent lower leg muscle wasting in both legs for moderate or severe stroke patients during acute hospitalization.
Several studies have been reported regarding the efficacy of NMES to prevent lower leg muscle wasting during acute hospitalization for patients with several diseases, but the efficacy is controversial (Gerovasili et al., 2009; Segers et al., 2014; Maffiuletti et al., 2013; Kho et al., 2015; Fischer et al., 2016). Gerovasili et al. (2009) showed the positive effects of NMES for preventing muscle wasting in critically ill patients whose cross-sectional diameter of the vastus intermedius in the electrical muscle stimulation group (–12.5%) significantly decreased to a lesser degree compared with that in the control group (–21.5%). However, other studies showed that NMES had no significant effect on muscle layer thickness or muscle volume (Fischer et al., 2016, Poulsen et al., 2011). We speculated that the reason for the difference between each result for these patients is their pathophysiological characteristic. Severe inflammation or catabolic activation can be a common cause for muscle wasting often seen in patients with critical illness (Puthucheary et al., 2013; Witteveen et al., 2014). Controlling the inflammation or catabolic activation of these patients would be difficult for clinicians; hence, they could not show uniform results. Our study population who were admitted because of acute stroke onset also showed inflammation (Whiteley et al., 2012) or catabolic activation (Springer et al., 2014); however, we deliberated why acute stroke patients showed less inflammation or catabolic activation compared with patients with critical illness; thus, quadriceps muscle wasting was prevented in many patients in this study.
The pathophysiological mechanisms for stroke-related muscle wasting have been reported to be inactivity, denervation, malnutrition, inflammation, and metabolic imbalance (Scherbakov & Doehner, 2011; English et al., 2010; Scherbakov et al., 2013; Scherbakov et al., 2015), but these mechanisms are different between both limbs (Springer et al., 2014; van Kuijk et al., 2007). The denervation of stroke patients has also been reported to mainly occur in the paretic limb (van Kuijk et al., 2007), and cerebral infarct severity correlated with catabolic activity only in the contralateral leg, but not in the ipsilateral leg (Springer et al., 2014). The activity level in the paretic limb was lower than that in the non-paretic limb in patients with ischemic stroke (Strømmen, Christensen, & Jensen, 2014). Other effects for muscle activation have also been different between both limbs: decreased descending command from the motor cortex (Feydy et al., 2002), decreased motor unit number (Kouzi et al., 2014), and change in the postural mechanisms as a result of stroke in the quadriceps muscle (Garland, Willems, Ivanova, & Miller, 2003; Garland, Ivanova, & Mochizuki, 2007). Thus, the quadriceps muscle thickness of the non-paretic limb was not decreased in the NMES group only.
We conducted this study as a pilot study, particularly in patients with moderate to severe acute stroke because they often are unable to walk and are dependent. Mild stroke patients often are able to walk in the acute phase, and the decrease in muscle mass has been shown to be less likely to occur in these subjects (Nozoe et al., 2016). The modalities of NMES were also decided as reference with a previous study (Maffiuletti et al., 2013), and particularly in frequency (5 sessions/week) was conducted within the range of feasibility because all subjects also had five sessions of physiotherapy per week. Other modalities of NMES, such as symmetric impulses (50 Hz), pulse duration (300 μs), on-off time, or intensity (20 mA–50 mA), were also decided to avoid discomfort or fatigue for each subject. In fact, our subjects in the NMES group did not drop out for these reasons. Conducting NMES for acute stroke patients may be safe in accordance with these modalities of NMES. We studied quadriceps muscle thickness as an outcome of the efficacy of NMES in acute stroke patients, but we could not measure long-term functional outcome. Long-term functional improvement would also be important for these patients. Moreover, significant differences were found regarding the time to first measurement from onset between both groups. Muscle wasting in patients with acute stroke has been reported to begin 4 h from stroke onset (Carin-Levy et al., 2006); hence, the differences may affect the results. Our study could not control the rehabilitation program particularly on early mobilization; this also may affect the results. Finally, we have also lacked the randomization or blinded assessment in this study due to the lack of enough foundation. In the future, we plan to conduct another randomized controlled study to overcome these limitations and show long-term functional outcomes.
Conclusion
We studied the efficacy of NMES on quadriceps muscle wasting for patients with acute moderate or severe stroke during hospitalization. We conclude that NMES could prevent lower leg muscle wasting of patients with moderate or severe acute stroke.
Conflict of interest
None.
Footnotes
Acknowledgments
This work was supported by JSPS KAKENHI Grant Number 15K16410.