
Abstract
BACKGROUND:
Foot drop is common gait impairment after stroke. Functional electrical stimulation (FES) of the ankle dorsiflexor muscles during the swing phase of gait can help correcting foot drop.
OBJECTIVE:
To evaluate efficacy of additional novel FES system to conventional therapy in facilitating motor recovery in the lower extremities and improving walking ability after stroke.
METHODS:
Sixteen stroke patients were randomly allocated to the FES group (FES therapy plus conventional rehabilitation program) (n = 8), and control group (conventional rehabilitation program) n = 8. FES was delivered for 30 min during gait to induce ankle plantar and dorsiflexion. Main outcome measures: gait speed using 10 Meter Walk Test (10 MWT), Fugl-Meyer Assessment (FMA), Berg Balance Scale (BBS) and modified Barthel Index (MBI).
RESULTS:
Results showed a significant increase in gait speed in FES group (p < 0.001), higher than the minimal detected change. The FES group showed improvement in functional independence in the activities of daily living, motor recovery and gait performance.
CONCLUSIONS:
The findings suggest that novel FES therapy combined with conventional rehabilitation is more effective on walking speed, mobility of the lower extremity, balance disability and activities of daily living compared to a conventional rehabilitation program only.
Introduction
Stroke is the leading cause of death and serious long term disability in adults. Three months after stroke, 20% of individuals remain wheelchair-bound and 70% walk at reduced velocity (Sakuma, Ohata, Izumi, Shiotsuka, Yasui, Ibuki, & Ichihashi, 2014). Correcting the abnormalities of hemiplegic gait is the most important component of rehabilitation for independent and functional activities in daily living, community-dwelling, and social environments (Chung, Kim, Cha, & Hwang, 2014). In up to 20% of stroke patients, a persisting weakness of the contralateral foot is a major cause of gait impairment, usually described as “drop foot.” (Lyons, Sinkjær, Burridge, & Wilcox, 2002). The patients are not able to actively dorsiflexion the foot during the swing phase of gait, which results in undesirable compensatory movement patterns, decreased gait velocity, restricted functional mobility, and increased risk of falls (Cheng, Chen, Wang, & Hong, 2004; Ernst, Grundey, Hewitt, von Lewinski, Kaus, Schmalz, & Liebetanz, 2013; Franceschini, Massucci, Ferrari, Agosti, & Paroli, 2003). Patients compensate inability to lift the foot by walking with increased hip circumduction to propel the leg forward while preventing the toes from catching on the ground during swing phase and initial contact (Olney, & Richards, 1996).
The standard mode of care for foot drop includes an ankle foot orthosis (AFO) that holds the foot in a neutral position. In general, AFOs have been found to support ankle dorsiflexion during the swing phase and improve knee stability in the early stance phase in individuals with drop foot (Fatone, Gard, & Malas, 2009; Mulroy, Eberly, Gronely, Weiss, & Newsam, 2010). However, there are several disadvantages of AFOs such as limited ankle mobility that may contribute to the development of contracture and difficulty with standing from a chair, along with discomfort and unfavorable aesthetics (Given, Dewald, & Rymer, 1995; Janssen, Bussmann, & Stam, 2002; Doğğan, MengüllüoĞĞlu, & Özgirgin, 2011; Teasell, McRae, Foley, & Bhardwaj, 2001). An alternative to the more traditional AFO is the use of functional electrical stimulation (FES). FES applied to the peroneal nerve during the swing phase of ambulation provides active dorsiflexion and can reduce foot drop by facilitating voluntary muscle activity to improve gait quality and symmetry (Liberson, Holmquest, Scot, & Dow, 1961; Hausdorff, & Ring, 2008; Everaert, Thompson, Chong, & Stein, 2009; Ring, Treger, Gruendlinger, & Hausdorff, 2009). Numerous studies of stroke rehabilitation have brought forward strong evidence that FES improves hemiplegic gait parameters, increases gait speed, decreases energy expenditure during walking and improves gait symmetry (Harris, & Eng, 2004; Stein, Everaert, Thompson, Chong, Whittaker, Robertson, & Kuether, 2009; Burridge, Taylor, Hagan, Wood, & Swain, 1997). However, several studies have demonstrated disadvantages of FES including possible skin irritation, difficulty with electrode placement and stimulus discomfort (Stein, et al., 2009; Taylor, Burridge, Dunkerley, Lamb, Wood, Norton, & Swain, 1999; van Swigchem, Vloothuis, den Boer, Weerdesteyn, & Geurts, 2010; Wieler, Stein, Ladouceur, Whittaker, Smith, Naaman, & Aimone, 1999).
In order to reduce the disadvantages of FES, we present in this study a novel FES protocol based on multi-pad electrodes for correcting foot drop (Bijelić, Popović-Bijelić, Jorgovanović, Bojanić, & Popović, 2004; Keller, Lawrence, Kuhn, & Morari, 2006; Popović, & Popović, 2009; O’Dwyer, O’Keeffe, Coote, & Lyons, 2006). Multi-pad electrodes contain individual, relatively small stimulation pads which can be activated individually or as a part of a stimulation pattern. The use of this novel electrode may be a solution for decreasing muscle fatigue as well as stimulus and placement discomfort because it allows for more precise stimulation of affected areas and simple attachment to the lower limb.
The aim of this study is to compare efficacy of additional novel FES system to conventional therapy in comparison to conventional therapy only in facilitating motor recovery in the lower extremities and improving walking ability after stroke.
Methods
Design
We conducted a single-blind (evaluator) randomized controlled trial. The study was approved by the Ethical Committee of the Clinic for Rehabilitation “Dr Miroslav Zotovic”, Faculty of Medicine, University of Belgrade, Serbia. All participants signed informed consent to participate in this study and procedures were performed according to the Declaration of Helsinki. This study was registered at the ClinicalTrials.gov ID NCT02729636.
Settings
The study was performed in a post-acute rehabilitation medicine hospital, Clinic for Rehabilitation “Dr Miroslav Zotovic”, Belgrade, Serbia.
Participants
Seventy participants older than 18 years were recruited for the study from January to June 2016, from the pull of waitlist patients scheduled for inpatients rehabilitation. All inpatients had hemiparesis resulting from a single stroke confirmed by either computed tomography or magnetic resonance imaging. Diagnosis was performed by an expert neurologist physician (R.L.) with 5 years of experience. Each patient involved in the study underwent physical examination performed by a medical doctor and/or physiotherapist with more than 5 years of clinical experience. Inclusion criteria for study participation were: a) Hemiplegia or hemiparesis caused by first-time stroke, b) Independent walking before the stroke, c) Foot dorsiflexion inability during the swing phase of gait, d) Sufficient cognitive and language functions to reliably follow study related instructions and provide feedback, e) Ability to walk at least 10 m with or without the use of aids and walk speed less than 0.4 m/s. Subjects were excluded who have contractures which interfered with ankle dorsiflexion, concomitant lower motor neuron dysfunction or non-stroke-related upper motor neuron dysfunction, uncontrolled seizure disorder, history of cardiac arrhythmias with hemodynamic instability, implanted devices, severely impaired cognition and communication, evidence of deep venous thrombosis or thromboembolism, skin rupture or pregnancy.
The participants were randomized using table of random numbers (SAS software, 9.4, SAS Institute, USA) and then assigned to either the FES group (FES therapy plus conventional rehabilitation program) or control group (conventional rehabilitation program).
To determine the number of participants needed in each group we calculated sample size based on the results from Bogataj et al. based in detection of a minimal clinically important mean difference of 0.13 m/s on a 10 m walk test (10MWT) (Bogataj, Gros, Kljajić, Aćimović, & Maležič, 1995). The estimated desired sample size was seven subjects per group.
Intervention
All study subjects received the conventional stroke rehabilitation program of physiotherapy based on the neurodevelopmental facilitation approach and occupational therapy focused on activities of daily living during the treatment for 60 min a day, 5 days a week, for 4-weeks. The FES group also received electrical stimulation to the tibial nerve in the preswing phase of the gait and to the common peroneal nerve in the swing phase results in ankle plantar flexion and dorsiflexion, respectively. Electrical stimulation was applied using a portable new FES system for correcting foot drop – FESa (Tecnalia R&I, Spain). The system consists of a stimulating unit, demultiplexer, garment with integrated multi-pad electrode, wireless inertial sensors and tablet PC with application. The garment with integrated multi-pad electrode was placed on the skin around the patient’s knee, close to the neck of the fibula in order to stimulate common peroneal and tibial nerves. The inertial sensor was placed on the patient’s paretic foot so as to register the patient’s foot position during calibration and gait cycle. Upon placing the garment in the envisaged position, by means of a tablet application, calibration process started – consisting of short-term stimulation of each electrode pad. The control unit attached on the garment received this trigger signal wirelessly and delivers a single pulse train comprising of pulses of various pulse widths and amplitudes to the demultiplexer which routes it to different independent conductive pads within the multi-pad electrode. The automatic algorithm suggested the electrode pads that should be used for stimulation based on the sensor registered values. Once the parameters for stimulation were determined, the input was sent to the stimulator unit, which was either kept in patient’s pocket or was strapped to the patient’s waist, and the patient started walking. While walking, the system was independent from tablet PC. The stimulation frequency was set to 40 Hz and the pulse width to 400μs. Stimulation began with 20 min sessions per day for the first week of the treatment and progressed to 30–40 min sessions daily for rest of the 4-week treatment.
Outcome measures
Primary outcome: Gait speed
The primary outcome was gait speed as a valid and reliable measure of walking recovery after stroke (Richards, Malouin, Dumas, & Tardif, 1995; Marquis, Moore, Howieson, Sexton, Payami, Kaye, & Camicioli, 2002). Speed was quantified using the 10MWT, which is one of the most frequency used measures to assess gait function in people after stroke (Curfman, Connor, Moy, Heitsch, Panagos, Lee, & Ford, 2014). The walking course was 14 m long in a hallway: After a 2 m warm-up, 10 m were used for the speed measurement and 2 m for slowing to a stop. Patients were instructed to walk at a comfortable speed to use assistive devices (Hornby, Zemon, & Campbell, 2005). According to previous study, gait speed can be stratified into clinically meaningful functional ambulation classes including household ambulation (0.4 m/s), limited community ambulation (0.4 to 0.8 m/s), and full community ambulation (0.8 m/s) (Perry, Garrett, Gronley, & Mulroy, 1995).
Secondary outcomes
We evaluated the following secondary outcome measures: Fugl-Meyer Assessment, Berg balance scale and Barthel index. Fugl-Meyer Assessment (FMA) is a valid measure of post-stroke motor impairment and measures lower extremity reflexes, flexor and extensor synergy patterns, volitional movement and coordination through a series of movement tasks. It is designed to assess motor functioning, balance, sensation and joint functioning in hemiplegic post-stroke patients. The FMA is designed to assess motor functioning of the hip, knee and ankle in the lower extremity with a maximum motor score of 34 for the lower extremity. Better scores suggest better performance (Fugl-Meyer, Jääskö, Leyman, Olsson, & Steglind, 1974; Sanford, Moreland, Swanson, Stratford, & Gowland, 1993). Berg Balance Scale (BBS) is a widely used clinical measurement of static and dynamic balance function and is generally considered to be the gold standard. The scale includes 14 five-level items with a maximum global score of 56 for assessing balance in sitting or standing posture. The score is interpreted as follows: 0–20, wheelchair bound; 21–40, walking with assistance; 41–56, independent. A score of 45 points is the relative risk and an appropriate cut-off for safe independent walking (Maeda, Kato, & Shimada, 2009; Blum, & Korner-Bitensky, 2008). Barthel Index (BI) assesses activities of daily living (ADL), functional mobility and gait. It includes 10 items of ADL and all items are rated based on the amount of assistance required to complete each activity. The scoring method is based on a five-level scale with a maximum total score of 100. A score >60 represents independent living, with lower scares representing assisted or totally dependent living (Uyttenboogaart, Stewart, Vroomen, De Keyser, & Luijckx, 2005; Wade, & Collin, 1988).
All outcome measures were evaluated at the beginning and end of the 4-week training by a medical doctor and/or a physiotherapist, who was blinded to the aims of the study and to which group the subject had been allocated.
Statistical analysis
The data obtained from all the patients having passed inclusion criteria were analyzed by means of SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were presented as mean±standard deviation (SD) for continuous parameters and frequency for categorical parameters. The results of Shapiro-Wilk test showed that continuous parameters were normally distributed. For statistical comparisons of means for continuous parameters between groups, we used the paired t-test for two independent groups. For statistical comparisons between means of continuous parameters recorded before and after therapy in each group, we used the paired sample t-test for two dependent groups. Chi-square tests or Fisher’s exact tests were used for comparing categorical parameters between groups. Statistical testing of hypotheses was performed by two-tailed statistical tests with a significance level of 0.05. The difference between pre- and post-treatment data for both groups was calculated as pre-treatment minus post-treatment. Effect size was calculated using Cohen’s d to evaluate the clinical importance of the measured changes.
To determine the number of participants needed in each group, sample size and power calculations were performed using R Studio software v. 0.98.976 (Boston, MA, USA), SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and G*Power 3.1. The calculations were based on detection of a minimal clinically important mean difference of 0.13 m/s on a 10 m walk test (10MWT), using a two-tailed test, an α level of 0.05 and a desired power of 80% (Bogataj et al., 1995). Effect size was calculated using Cohen’s d to evaluate the clinical importance of the measured changes.
A formula for calculating sample size was:
Results
Seventy patients (n = 70) with post-stroke hemiparesis were screened for eligibility criteria. Sixteen patients fulfilled all eligibility criteria, agreed to participate and were randomized to the FES group (n = 8) or the control group (n = 8). The reasons for ineligibility were non-independent gait (n = 24), medically unstable conditions (uncontrolled hypertension, cardiac arrhythmia with hemodynamic instability, uncontrolled seizure disorder; n = 23) and unwillingness to participate (n = 7). Figure 1 shows a flow diagram of patient recruitment and retention through the study.
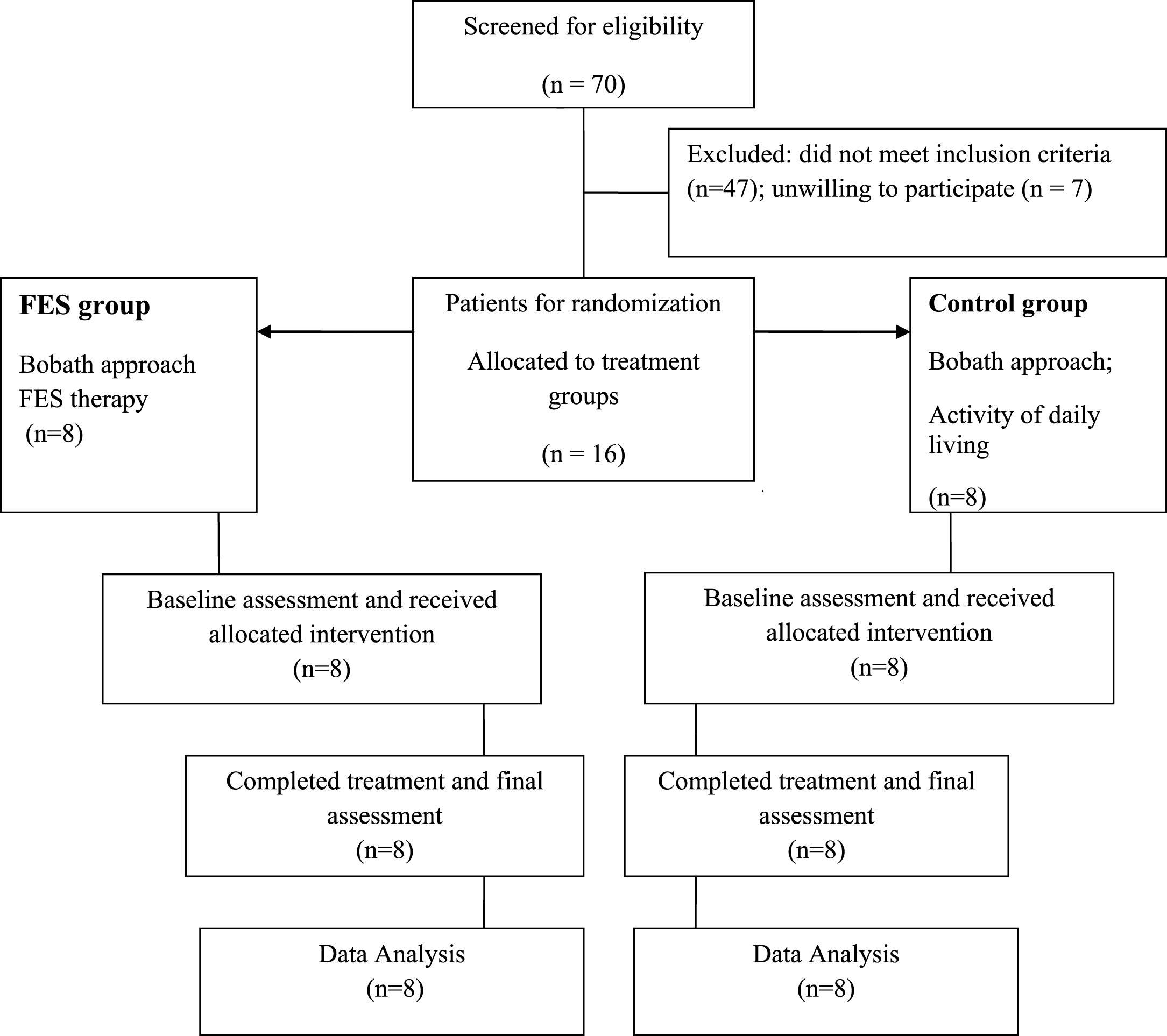
Flow diagram of the study protocol.
Baseline features of both groups were similar for all variables (Table 1). No significant differences were found in the baseline values between subject groups, indicating that they were homogenous in these measurements before treatment.
Baseline demographics for both groups
Comparison of means for outcome measurements between groups at baseline and after 4- week is displayed in Table 2.
Comparison of outcome measurements between groups (mean±SD)
1Fugl-Meyer assessment; 2Berg Balance Scale; 3Barthel Index. Significant difference between groups: *p < 0.05, (95% confidence interval).
With regards to the gait results of stroke patients, a significant increase in mean walking speed between the beginning and end of the trial was in the FES group (p < 0.001). As shown in Fig. 2, mean scores in the FES group increased from 0.25±0.11 to 0.38±0.15 in contrast to the control group 0.23±0.10 to 0.27±0.14.
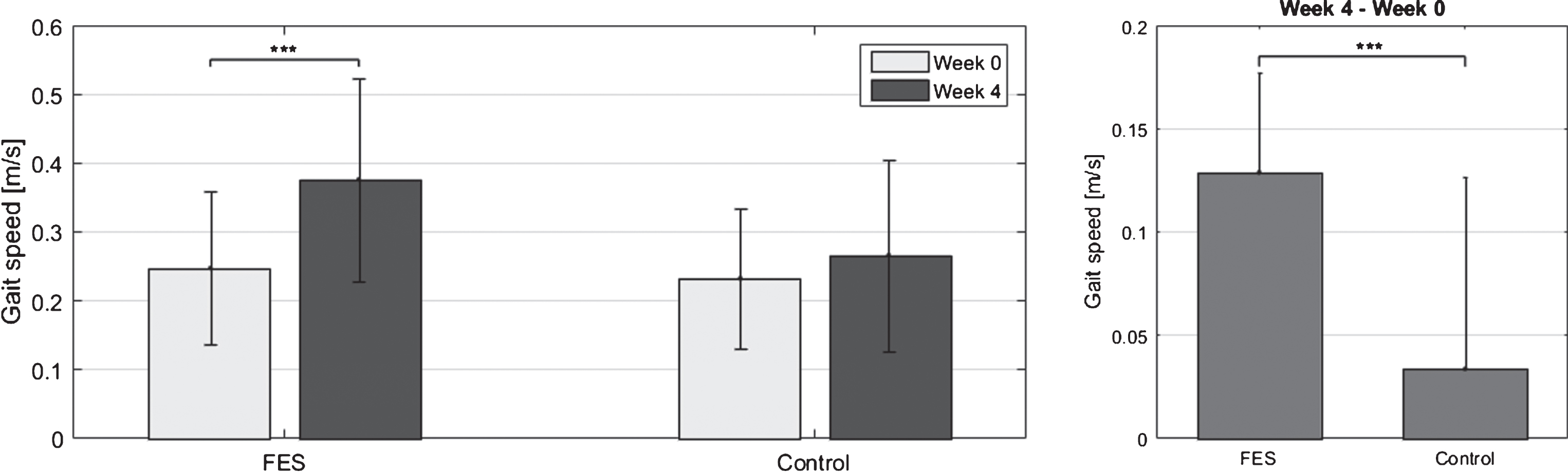
Analysis of gait speed. Left: Gait speed (mean±SD) for FES and Control group before (Week 0) and after (Week 4) treatment. Right: Difference in gait speed (Week 4 – Week 0) for FES and Control group. Horizontal bar with asterisks indicates the statistically significant difference in mean gait speed between the respective conditions. (*, p < 0.05; **, p < 0.01; ***, p < 0.001).
Analysis of functional categories based on walking speed showed that five subjects from the FES group transitioned from household ambulation category (<0.4 m/s) to limited community ambulators (≥0.4 and ≤0.8 m/s). Three subjects did not show improvement and stayed in the household ambulation category. In addition, the household ambulators who successfully transitioned to limited community ambulators demonstrated improvement in secondary outcomes compared with baseline scores and scores after 4-week treatment (Fig. 3.). The initial FMA score in FES group increased from 22.9±2.4 to 25.8±3.2 (p < 0.01), BBS at baseline was 37.4±10.5 and after 4-week 48.1±4.6 (p < 0.01) and BI score increased from 75.0±13.9 to 86.9±7.5 (p < 0.05). In the control group, only two subjects transitioned from home ambulators to limited community ambulators while the remaining subjects showed no improvement. According to followed secondary outcome in the control group only exhibited changes was in BBS score from 36.6±7.4 to 42.0±8.5 (p < 0.05).

Clinical outcomes (Left – Fugl-Meyer Motor Function Assessment, Middle – Berg Balance Scale, Right – Barthel Index) for FES and Control group before (Week 0) and after (Week 4) treatment. Horizontal bar with asterisks indicates the statistically significant difference in mean gait speed between the respective conditions. (*, p < 0.05; **, p < 0.01; ***, p < 0.001).
No adverse events were registered during or after the application of the treatment. No participant dropped out of the study.
This randomized controlled trial examined whether therapy with a novel FES paradigm based on the multi-pad electrode, combined with conventional therapy, was more effective in correcting of foot drop in comparison to conventional therapy only.
Improved walking ability is one of the most frequently stated goals of people with stroke undergoing rehabilitation and among those individuals living with stroke in the community (Bohannon, 1988; Harris, & Eng, 2004). Walking speed is a simple but highly reliable and responsive parameter for gait in stroke survivors (Collen, Wade, & Bradshaw, 1990; Friedman, Richmond, & Baskett, 1988; Wade, Wood, Heller, Maggs, & Langton, 1986). Reliability has been established for test-retest and between-observer measurements (Holden, Gill, Magliozzi, Nathan, & Piehl-Baker, 1984; Wade, & Hewer, 1987). Moreover, gait speed correlates strongly with other parameters, such as balance, use of walking aids, number of falls and ADL function in elderly people (Holden, et al., 1984; Bohannon, 1989; Potter, Evans, & Duncan, 1995). Elderly healthy individuals have a preferred speed of between 1.1 m/s and 1.3 m/s, but can easily change their speed from slow to running. Individuals with stroke tend to be much slower, and are generally more limited in their choice of gait speed (Oberg, Karsznia, & Oberg, 1994). Perry et al. identified three levels based on gait speed over 10 m of walking in stroke survivors: unlimited ambulators (>0.80 m/s), limited ambulators (0.40–0.80 m/s) and household ambulators (<0.40 m/s) (Perry, et al., 1995). Participants in the present study with a mean speed of 0.27 m/s on the 10MWT had severe initial gait speed impairments. Transitioning to a higher class of ambulation was registered for 5 of 8 participants in FES group in comparison to only 2 of 8 in control group. The household ambulators who successfully transitioned to limited community ambulators demonstrated also improvement in FMA score. Sabut et al. found that FES applied to the anterior tibial muscle of the paretic limb increased FMA scores, reduced muscle tone, increased muscle strength and improved the entire gait pattern in stroke patients (Sabut, Sikdar, Kumar, & Mahadevappa, 2011).
The present study’s results of balance score showed better improvement in FES group. It could be favorable for functional independence after stroke regard to the fact that balance disability is positively related to mobility, ADL and falls (Tyson, Hanley, Chillala, Selley, & Tallis, 2007; Di Monaco, Trucco, Di Monaco, Tappero, & Cavanna, 2010). Activities of daily living were also better improved in FES group. The results are consistent with those of Tone, whose report showed that patients treated with FES had a faster gait, better mobility and increased functional ambulation (Lee, Kang, Im, Kim, Kim, Yoon, & Han, 2013).
Numerous studies have shown many advantages of FES therapy after stroke, such as active muscle contraction, improved muscle strength, reduced muscle tone, greater interlimb coordination and improvement of the entire gait pattern, and have further shown that FES is applicable to wide range of subjects (Tong, Ng, & Li, 2006; Embrey, Holtz, Alon, Brandsma, & McCoy, 2010; Robbins, Houghton, Woodbury, & Brown, 2006; Sheffler, Hennessey, Naples, & Chae, 2006; Sabut, Sikdar, Mondal, Kumar, & Mahadevappa, 2010). FES directly assists in the performance of disrupted functions in humans, causes changes in cortical excitability and stimulates cortical reorganization (Bohannon, 1988). During FES, bursts of short pulses of electrical charge generate an electrical field that triggers action potentials in afferent and efferent neural pathways.
However there are limitations which disrupt the use of FES. It is assumed that greater selectivity in the application of FES would result in improved effects because it would allow for longer application of stimulation without the rapid fatigue that normally occurs. The most common problem in the clinical use of FES is finding an adequate position for placing transcutaneous electrodes from one individual to the next, setting stimulation parameters for producing functional and comfortable foot movement while limiting skin irritation and fast muscle fatigue. Rapid fatigue greatly restricts the usefulness of the FES approach to restore meaningful gait over long periods. As a way to overcome these limitations, many research groups have developed various systems using FES for correcting drop foot such as Bioness L300, WalkAide and ODFS ® Pace (Taylor, et al., 1999; Israel, Kotowski, Talbott, Fisher, & Dunning, 2015). Many barriers to compliance have been identified for different foot-drop FES systems including reliability and robust stimulation triggering, the wearing of wires and switches, difficulty with electrode placement, donning and doffing the systems and unreliable detection of gait events.
This study presented a system able to respond to gait cycle events, such as heel strike, heel-off and toes off, but also capable of responding to real-time changes in mean swing/stance time and loading by employing algorithms that adjust the relevant stimulation parameters. FES using a multi-pad electrode allows better selectivity, simple attachment to the lower limb and decreased muscle fatigue because of the size and shape of the electrode. The electrode is based on 16 small stimulation pads where each pad can be activated individually or as a part of a stimulation pattern. Based on previous findings, stimulation via multi-pad electrodes has emerged as step forward in FES technology (Malešević, Malešević, Bijelić, Keller, & Konstantinović, 2014; Azevedo-Coste, Bijelic, Schwirtlich, & Popovic, 2007; Malešević, Maneski, Ilić, Jorgovanović, Bijelić, Keller, & Popović, 2012).
Study limitations
A number of limitations must be kept in mind when interpreting the results of this study. This study was limited in that it examined stroke survivors with a mean walking speed of 0.3 m/s at initial evaluation, so results should not be generalized. We did not consider other factors that could have influenced motor recovery such as type and location of stroke lesion, initial severity, motivation, cognition abilities, and dose-related factors such as the number of movement repetition. Finally, kinematic and EMG analyses should be evaluated.
Conclusion
The present study’s findings suggest that novel FES therapy using a multi-pad electrode combined with conventional rehabilitation is more effective on walking speed, mobility of the lower extremity, balance disability and activities of daily living compared to a conventional rehabilitation program only.
Conflict of interest
None to report.