
Abstract
PURPOSE:
To determine the effects of a novel dynamic neuromuscular stabilization (DNS) technique on gross motor function, diaphragm movement, and activation of the external oblique (EO) and internal oblique (IO)/transversus abdominal (TrA) muscles in participants with cerebral palsy (CP).
METHOD:
Fifteen participants with CP (7 females) underwent DNS intervention for 30 minutes/day, 3 days a week for 4 weeks. Gross motor function, diaphragm movement, and muscle activation were determined using a gross motor function measure (GMFM-88), ultrasound, and electromyography measurements, respectively, before and after the DNS core stabilization intervention. Paired t-tests were used at p < 0.05.
DESIGN:
A single-arm, pretest-posttest clinical trial.
RESULTS:
GMFM scores for standing, walking, and jumping domains were significantly improved after the intervention (P < 0.05). Diaphragm descending movement (P = 0.0001) and activation of the internal oblique and transversus abdominals were initially undetectable, but remarkably increased after the intervention (P = 0.012).
CONCLUSIONS:
DNS is a promising, effective intervention for facilitating deep core muscle activation of the underactive muscle chain comprising the diaphragm, internal oblique, and transversus abdominals, thereby improving age-appropriate standing, walking, and jumping in participants with spastic diplegic CP.
Introduction
Core instability is a common neuromuscular dysfunction in participants with cerebral palsy (CP) which is often implicated with postural and dynamic locomotor impairments. Neurodevelopmentally, during early postural development, the newborn diaphragm acts as a respiratory muscle (Abel & Damiano, 1996). As the central nervous system (CNS) matures, sagittal stabilization of the cervical and lumbar spine, pelvis, and chest sequentially develops around 4½ months of age, which then progresses to frontal and transverse stabilization (e.g., rolling, turning, creeping, and crawling) (Gandevia & Hodges, 2000). At approximately 6 months of age, the diaphragm fully establishes its dual function as both a respiratory and postural stabilization muscle when abdominal breathing is coordinated with chest breathing, thereby resulting in essential uprighting postural stabilization for sitting, standing, and walking (Cresswell, Daggfeldt, Hodges, & Thorstensson, 2001). However, children with CP demonstrate neurodevelopmental impairments with uprighting postural stabilization and anticipatory trunk postural adjustments under the feed-forward mechanism of control (Frank, Kobesova, & Kolar, 2013). A recent clinical study showed that children with CP had impaired core stability and associated proximal scapular stability, which led to functional limitations in reaching and grasping and impaired motor control during lower extremity movement (Alison, Carol, Marie, & Tim, 2007).
Contemporary core stabilization exercises including neurodevelopmental treatment (NDT) (e.g., bridging, curl-up exercise), abdominal bracing (AB), abdominal drawing-in maneuver (ADIM) (Arokoski, Kankaanpää, & Valta, 2004; Ju & Shin, 2010) and dynamic neuromuscular stabilization (DNS) are primarily utilized to treat adults with core instability. However, there is a dearth of clinical evidence investigating whether core stabilization exercises are beneficial for children with CP. ADIM and AB core stabilization exercises involve conscious, selective activation of the transverse abdominis (TrA) and coactivation of deep and superficial core muscles, respectively, which are not easily conducive to children with CP who have inherent cognitive impairment or attention deficits (Akins, Bassan, Haidar, Huppi, Limperopoulos, Moore, Plessis, Robertson, Soul, Volpe, & Warfield, 2005). Thus, the therapeutic effects of these exercises remain largely unknown and have not been effectively implemented compared to other conventional exercises. DNS has recently gained widespread clinical acceptance because it provides subcortical or reflexive core stabilization via balanced co-activation of the diaphragm, transverse abdominis (TrA)/internal oblique (IO), multifidus, and pelvic floor in coordination with intra-abdominal pressure (IAP) and superficial abdominal muscles (Jelsma, Stark, & Unger, 2013; Liebenson, 2007). Specifically, DNS uses special stimulation zones to connect the discontented core stabilization chain and reestablish the sensorimotor pathways mediating the dynamic neuromuscular core stabilization, thereby resulting in automatic core stabilization. Hence, it is useful for participants with CP who have cognitive and attention deficits. Nevertheless, the therapeutic effects of the DNS technique on core stabilization, balance, and gait function remain unknown in participants with CP. Therefore, the purpose of the present study was to investigate the effects of DNS on diaphragm and abdominal motor control, balance, and gait function in participants with CP. The proposed hypothesis was that the DNS technique would improve diaphragm and abdominal motor control, balance, and gait function in participants with CP.
Methods
Participants
A convenience sample of 16 participants with spastic diplegic CP (7 females; mean age±SD = 14.9±3.4 years) was recruited from a community-based rehabilitation center. All of the participants’ parents provided informed consent forms, and the study protocol was approved by the human ethics and institutional review board (IRB) prior to the experimental study (Yonsei University 1041849-201507-BM-507-01). Inclusion criteria entailed: (1) a diagnosis of spastic diplegic CP, (2) age between 10 and 18 years, (3) a gross motor function classification system (GMFCS) level from I-III, and (4) the ability to follow instructions. The exclusion criteria were severe visual or cognitive impairment, seizure, any previous surgical history within the last 6 months, or medication affecting the experimental procedure.
Clinical tests
Standardized clinical tests included GMFCS, the modified Ashworth spasticity scale (MAS), and the Gross Motor Function Measure (GMFM). GMFCS was used to classify the functional gross motor performance levels of the participants with CP (Beckung, Hagberg, & Himmelmann, 2006). MAS was used to determine the resistance associated with spasticity encountered during passive muscle stretching (Bohannon & Smith, 1987). The GMFM test (GMFM-88) is a standardized clinical assessment designed to evaluate changes in gross motor function in participants with CP (Marshall & Murphy, 2003; Rosenbaum & Russel, 1989). In the present study, only the GMFM subsections C, D, and E were used because all subjects were already able to complete the GMFM subsections A and B. The reliability and validity of GMFCS, MAS, and GMFM are well established (Abel & Damiano, 1996; Beckung, Hagberg, & Himmelmann, 2006; Bohannon & Smith, 1987; Galuppi, Palisano, Rosenbaum, Russell, Walter, & Wood, 1997; Marshall & Murphy, 2003).
Real-time ultrasound imaging measurement for diaphragm movement
A real-time ultrasound with a 3.5-MHz curved transducer was used to determine the intervention-related changes in diaphragm movement. The transducer was first applied in the middle of the midclavicular and anterior axillary lines in the subcostal area and was manipulated to the medial, cranial, and dorsal directions to determine the clearest diaphragm image at the end of the expiration (baseline) and inspiration phases. Once the clearest diaphragm images were obtained for both phases, the images were stored for further analysis of the dimension of the diaphragm movement (Blanc, Boussuges, & Gole, 2009). The diaphragm movement was operationally defined as a displacement in the diaphragm apex between the both expiration (baseline) and inspiration phases (Fig. 1). For the consistent measurements of the diaphragm, the identical anatomical landmarks were applied at the pretest and posttest.
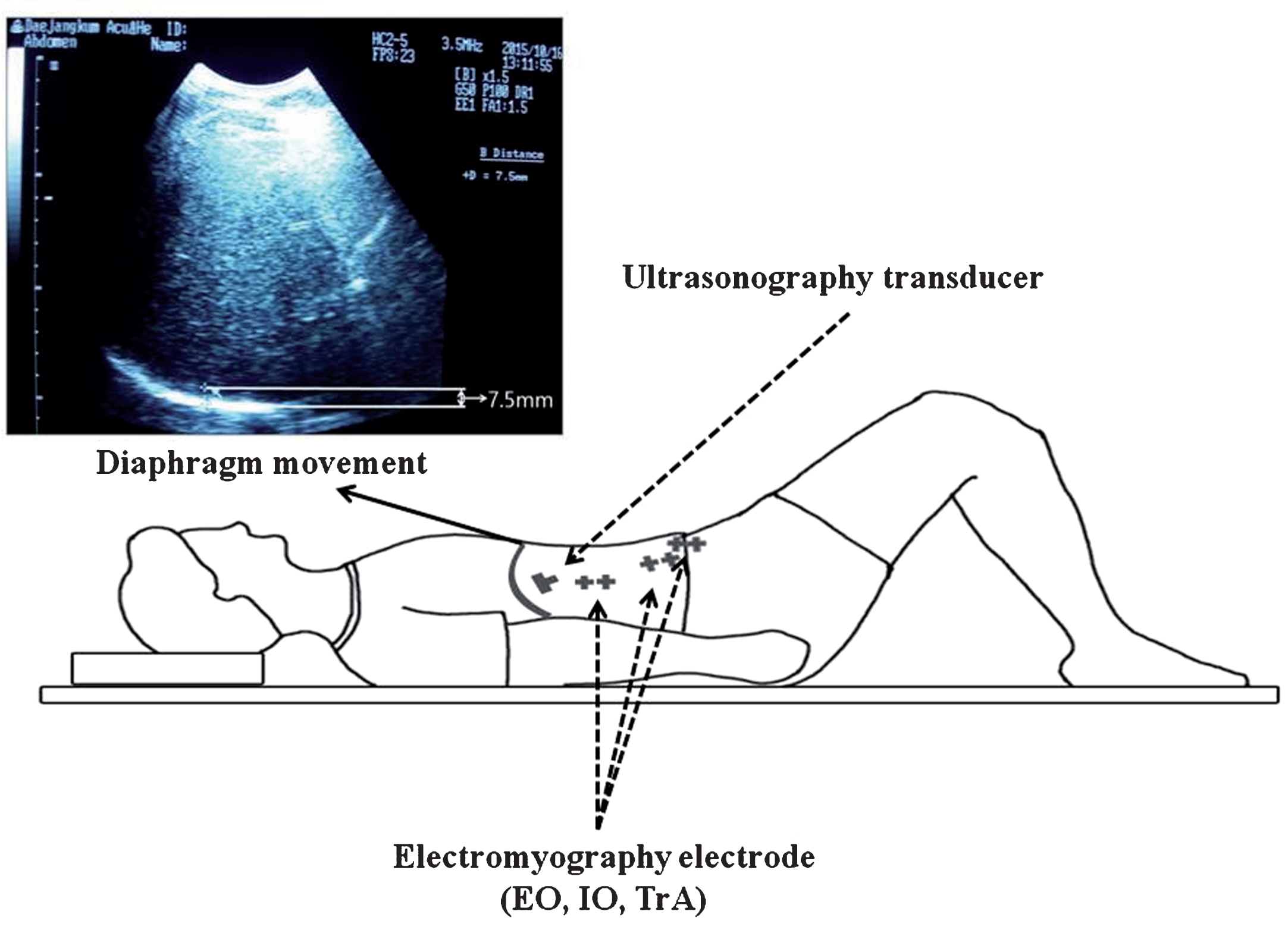
Experimental setup for ultrasound imaging of diaphragm movement and EMG recording of TrA/IO and EO.
EMG was used to determine abdominal core muscle activity including EO and IO/TrA muscles. Prior to the EMG recording, the skin was prepared by cleansing with alcohol. A bipolar electrode with a 1-cm inter-electrode space was placed on the right EO and IO/TrA muscles. Specifically, the TrA/IO electrode was located approximately 2 cm medially and inferiorly from the anterior superior iliac spine (ASIS) (Cram, Kasman, & Holtz, 1998; Marshall & Murphy, 2003). The participant was positioned in a hook-lying position with hip 70° flexion and then asked to lift his or her head approximately 5 cm off the floor. The EMG data collection was acquired at a sampling rate of 1024 Hz and processed with the 60 Hz notch filter, and the band-pass was filtered between 20 and 450 Hz. The EMG data analysis was rectified by root mean square (RMS) and normalized with a reference voluntary contraction (RVC). EMG data were collected 5 consecutive times and repeated if a motion artifact was noted. A 1-minute rest interval was provided to minimize any potential fatigue (Fig. 1).
Intervention
The DNS core stabilization exercise was provided 30 minutes/day, 3 times a week, for 4 weeks. The participant was asked to lie supine with 90° flexion of the hip and knee and was comfortably supported with a pad or the therapist’s leg. All participants practiced the following standardized DNS steps (Rosenbaum & Russel, 2000). First, the therapist identified the chest zone (between the 5th and 6th intercostal spaces, the intersection between the mammillary line and the horizontal xiphoid process) and applied a small amount of pressure with the thumb and index or middle finger (about 20 mmHg), with the stimulation vector aimed toward the contralateral ASISs. Second, while maintaining this alignment, the participant was asked to inhale, descending his or her diaphragm, and co-activate the TrA/IO and pelvic floor. Ultrasound imaging was used to ensure proper descending movement of the diaphragm and TrA/IO muscle activation in coordination with minimal activation of the EO muscles. Third, once proper respiratory function was controlled, the participant was asked to maintain the core stabilization and practiced unilateral and bilateral hip flexion and extension movements for sagittal core stabilization. As the participant’s sagittal core stabilization function improved, he or she progressed to more advanced transverse plane core movements and later with a theraband or manual resistance while stimulating selective zones to facilitate correct neurodevelopment of core stabilization skills.
Statistical analysis
Descriptive statistics include means and standard deviations. The target sample size of 15 participants was determined based on a power of 83% and an α of 0.05 to detect large differences in effect size. Paired t-test was used to determine any statistical significance in the gross motor function measure, diaphragm movement, and EMG amplitudes of the TrA/IO and EO contraction between the pretest and posttest. The level of statistical significance was set at α= 0.05. For statistical analysis of the data, SPSS (IBM Corp., Armonk, NY, USA), version 20.0 for Windows, was used.
Results
Demographic and clinical characteristics of the participants are shown in Table 1. All participants successfully completed the pretest, intervention, and posttest except one participant who withdrew from the study due to another health reason (Fig. 2).
Clinical and demographic characteristics of the participants
Clinical and demographic characteristics of the participants
aGMFCS: Gross Motor Function Classification System; bMAS: The Modified Ashworth Spasticity scale.
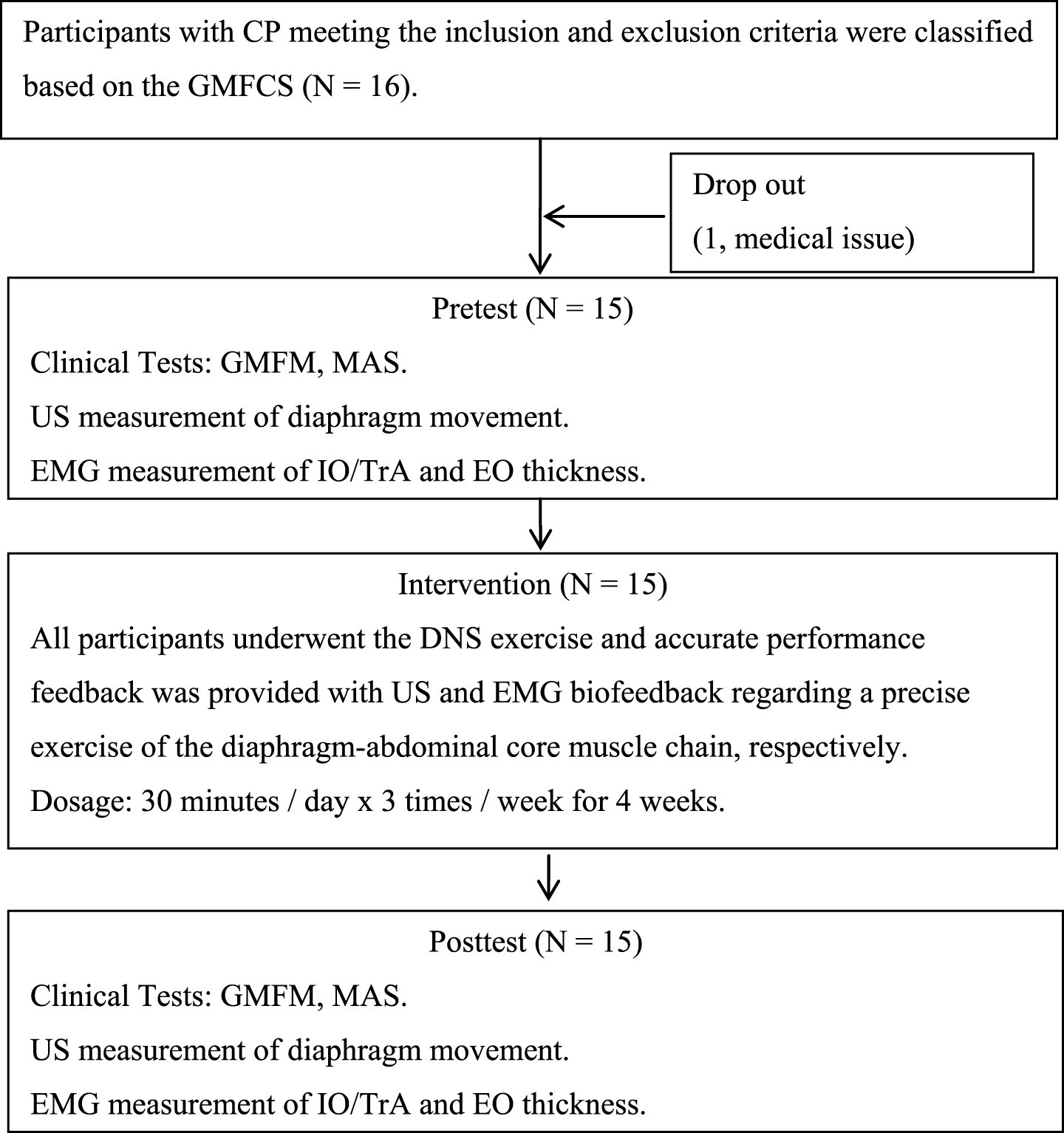
Clinical trial flow chart for experimental procedures.
Paired t-test showed that GMFM subsection scores C, D, and E significantly increased as a result of the DNS intervention, suggesting that the DNS core stabilization training was effective (P < 0.05) (Table 2).
The GMFM C, D, and E subsection scores before and after the intervention (N = 15)
The GMFM C, D, and E subsection scores before and after the intervention (N = 15)
aPaired t-test was significant at p < 0.05.
Diaphragm movement was significantly increased after 4 weeks of the DNS intervention (9.30±3.31 mm) (P < 0.01) compared to no apparent diaphragm movement at the pretest (Table 3).
Ultrasound diaphragm movement (mm) before and after the intervention (N = 15)
Ultrasound diaphragm movement (mm) before and after the intervention (N = 15)
aPaired t-test was significant at p < 0.05.
TrA/IO EMG activation significantly increased after the DNS intervention (P = 0.004). However, EO activation remained unchanged after the intervention (P = 0.148) (Table 4).
EMG amplitudes (% RVC) in abdominal muscles before and after the intervention (N = 15)
EMG amplitudes (% RVC) in abdominal muscles before and after the intervention (N = 15)
aPaired t-test was significant at p < 0.05. bEO: External obliques. cIO: Internal obliques. dTrA: Transverse abdominis.
The present investigation highlights the therapeutic efficacy of DNS exercise on core muscle activation, balance, and gait function. As anticipated, the DNS technique improved diaphragm movement, movement of the transversus abdominal and internal oblique abdominals, standing balance, and gait function in participants with CP, as evidenced using ultrasound and EMG measurements. Most importantly, these neuromechanical improvements were clinically associated with functional ambulation and independent motor performance in normal daily activities. To the best of our knowledge, this is the first clinical trial presenting the effects of a 4-week DNS intervention in participants with CP, which virtually makes it difficult to compare our data with any previous data.
EMG analysis data demonstrated that deep core stabilization muscle activation of the IO/TrA muscles was significantly improved by approximately 37% after the DNS exercise intervention, but the EO muscles did not show any change. Before the intervention, all participants were unable to activate the IO/TrA or diaphragm muscles. This finding corroborates a recent clinical study (Yoon & You, 2016) that compared the core stabilization effects of NDT and DNS exercises on TrA/IO EMG amplitude, ultrasound TrA muscle thickness values, and associated changes in core stability between healthy participants and stroke patients. EMG analysis demonstrated greater activation of the deep core TrA/IO muscles during DNS than during NDT in both healthy participants and stroke patients. The results suggest that DNS was more effective than NDT for reflex-mediated core stabilization. Perhaps, during the DNS core stabilization exercise, when inhaling, the diaphragm descends and reflexively stimulates the other deep core chain muscles (the TrA/IO-pelvic floor-multifidus) eccentrically because the chest zone is stimulated by the therapist. This eccentrically-activated muscle in turn becomes concentrically activated and produces sufficient IAP, resulting in the core stabilization and associated postural stability that precede any dynamic arm swing or leg movement during locomotion (Hodges & Richardson, 1997). In contrast, during the NDT core stabilization exercise, core stabilization is facilitated by realigning the abnormal movement and positioning of the pelvic girdle, which helps normalize the proprioceptive inputs of the lumbopelvic region. This facilitates the selective concentric activation of the deep TrA/IO core muscles (Yoon & You, 2016). Similarly, Ryu (2015) compared 3 different techniques (the NDT, the NDT plus cervical and lumbar core stabilization exercise, the NDT plus cervical stabilization exercise) in 45 participants with CP and found that the NDT plus cervical and lumbar core stabilization exercise was the most effective at improving standing balance and proprioception in the cervical reposition test (Ryu, 2015). Unger et al (Jelsma, Stark, & Unger, 2013). examined therapeutic effects of a selective abdominal muscle-targeted exercise program using whole body vibration (WBV) on posture and gait in participants with spastic CP. The core exercise program was designed to activate and strengthen the underactive or weak abdominal musculature and, as a result, cortically or consciously increased cutaneous awareness of core muscles using vibration. Therapeutic vibration showed increased gait, posture, resting abdominal muscle thickness, and functional abdominal strength in 27 participants with CP when assessed with the 1-Minute Walk Test, 2-dimensional posturography, ultrasound imaging, and sit-ups, respectively (Jelsma, Stark, & Unger, 2013). However, the important roles of the diaphragm and TrA/IO muscles were not determined (Jelsma, Stark, & Unger, 2013). In the present study, ultrasound imaging analysis of the diaphragm revealed that all participants were initially unable to utilize the diaphragm for both breathing and core or postural stabilization prior the intervention. After the DNS exercise, all participants demonstrated dual respiratory and increased descending diaphragm movement (9.30±3.31 mm) during the inspiration phase, and this range is comparable to the normal adult range (10.80 ± 6.65 mm) (Lee, 2013). Perhaps DNS was beneficial for selective facilitation of the diaphragm-TrA/IO-multifidus core chain, supporting the underpinning theory of involuntary or subcortical motor control to activate the inhibited or weak deep core muscle chain. Recently, Varnado (2015) reported that diaphragm and ribcage movement facilitation and trunk strengthening were beneficial for speech outcomes (sound pressure level and maximum phonation duration) in participants with spastic CP (Varnado, 2015).
Gross motor function measurement data demonstrated that DNS exercise helped improve kneeling, standing, and walking, as evidenced in the GMFM scores. This finding was consistent with Sterba’s results that demonstrated the positive effects of core strengthening exercise using horseback riding therapy (HBRT) on gait function in participants with CP. The previous study employed 16 weeks of a therapist-directed hippotherapy program and demonstrated improvements in walking function that lasted for 16 weeks post-HBRT as evident in the ‘E’ section of the GMFM (Sterba, 2007).
Together with previous findings, our data suggest that the DNS intervention is a promising technique to effectively activate TrA/IO and diaphragm muscles and improve associated postural and ambulatory function in participants with CP. It is possible that DNS emphasizes a subconscious feedforward mechanism that involves a relatively short-loop latency of anticipatory postural adjustment (APA) (Frank, Kobesova, & Kolar, 2013), thereby enhancing dynamic postural control during static standing and dynamic locomotion tasks (Barden & Kane, 2012). Furthermore, the DNS technique stimulated the underactive core muscles reflexively and neurodevelopmentally without requiring cortical attention. This is important because it indicates that DNS can be effective in pediatric patients with CP who exhibit cognitive and attention deficits. DNS exercise improved lumbopelvic core stabilization by synchronously and reflexively activating the underactive deepest diaphragm-TrA/IO core muscle chain while inhibiting the overactive superficial abdominal muscles (EO, rectus abdominals, and erector spinae) to generate IAP, thereby improving postural stability and gait, as reflected in the GMFM score. In fact, the DNS exercise is designed to activate diaphragm, TrA/IO, multifidus, pelvic floor muscles in coordination with superficial abdominal muscle (EO, rectus abdominals) and erector spinae because all patients initially utilize primarily overactive superficial muscles (EO, rectus abdominals, SCM, UT, and erector spinae). The relative changes in EMG activation were far greater as a function of the DNS, suggesting that this change in deep core muscle activation was facilitated by reflex-mediated stimulation of the chest zones during DNS (Blanc, Boussuges, & Gole, 2009; Liebenson, 2007). This reflex-mediated stimulation might have increased proprioceptive kinesthetic awareness, which evokes core stabilization via the monosynaptic reflexive activation system (Beckung, Hagberg, & Himmelmann, 2006). However, this theoretical assumption warrants further investigation.
A couple of study limitations should be considered in future research. One limitation is that a careful interpretation should be made when generalizing our findings to other types of hemiplegic and quadriplegic CP. The other limitation is that although the ultrasound imaging and EMG measurements provide accurate information of the selective diaphragm and abdominal muscle control, the advanced motion MRI imaging can be used to ascertain a more comprehensive mechanisms of the deepest core muscle chain (diaphragm – TrA – pelvic floor – multifidus) during DNS (Jelsma, Stark, & Unger, 2013).
Conclusion
The present research examined the effects of the novel DNS core stabilization exercise on diaphragm and abdominal motor control, balance and gait function in children with CP. The DNS core stabilization exercise was effective for activating the underutilized or underactive deep TrA/IO core muscles and diaphragm movement as well as associated balance and gait performance in the GMFM measure. This study provided an important clinical evidence for the application of the DNS core stabilization exercise in CP when designing effective core stabilization intervention to improve balance and gait function.
Conflict of interest
None to report.
Footnotes
Acknowledgments
Both Min Soo Son and Do Hee Jung have equally contributed to the manuscript preparation as first coauthors. All authors contributed to the conceptual framework of the study, experimental design, data collection, analysis, and manuscript preparation. This study was in part supported by the “Brain Korea 21 PLUS Project (Grant No. 2016-51-0009),” the Korean Research Foundation for Department of Physical Therapy in the Graduate School of Yonsei University.