
Abstract
BACKGROUND:
The person-centered perspective of residential care facility (RCF) residents with dementia with regard to their intimate and sexual lives is largely neglected in research.
OBJECTIVE:
We aim to provide methodological considerations and reflections on a performed qualitative study. Recommendations and a guide to study design are provided to inform and encourage future research on the inclusion of people with dementia as participants.
METHODS:
Methodological recommendations and reflections are described in chronological order of the procedure. Fragments of interviews are included for further illustration and clarification.
RESULTS:
Considering preparation, close involvement of clinical practice, and extensive deliberation regarding study design tended to be important. Considering procedure, investment in contacts with clinical practice and authorized representatives; an introduction meeting; person-centered inclusion and consent; profound skills in interviewing participants with dementia; and flexibility in data collection were proven of importance. Considering data analysis and study quality, including field notes and aiming at a balance between study quality and practicability to enhance study ‘rigor’ were found important.
CONCLUSION:
Including the person-centered perspective in research on intimacy and sexuality of RCF residents with dementia, is challenging and takes a flexible and creative approach. It is, however, worthwhile to close the gap in literature.
Introduction
Simultaneously with the aging population, the prevalence of dementia has increased. Worldwide estimations predict that in 2040, 80.1 million people will suffer from dementia (Ferri et al., 2005). Today 256,000 people in The Netherlands suffer from dementia, and this figure is expected to rise up to half a million in 2050 (Alzheimer Nederland, 2014). In 2013, a total of 80,555 people with dementia lived in psychogeriatric care units within Residential Care Facilities (RCF) in The Netherlands (Centrum Indicatiestelling Zorg, 2014).
In this psychogeriatric RCF care in The Netherlands, a paradigm shift is taking place (Actiz, 2012a). While medically-oriented views dominated care in the past, a more person-centered view is now expanding. Consequently, contributing to the Quality of Life (QoL) of residents with dementia and their (possible) partners has become a key objective for RCFs, in addition to ensuring safety and providing physical care (Actiz, 2012b; Elias & Ryan, 2011). However, it is not clear whether the QoL oriented care also includes the domain of intimacy and sexuality. Instead, professional caregivers may tend to regard these topics mostly as a purely private matter. Moreover, concerns and complex dilemmas concerning responsibility, consent capacity, and the willing balance between safety and security, and QoL are frequently reported and recognized by Dutch professional caregivers (Hoogeveen & van Waarde, 2016).
Despite increased research into the person-centered perspective in health care, little has been done on the theme of intimacy and sexuality (Roelofs, Luijkx, & Embregts, 2015). Person-centeredness can be defined as focusing on the perspective of the resident in research so results can contribute directly to policies and services (Murphy, Jordan, Hunter, Cooney, & Casey, 2014). The absence of this person-centered perspective seems remarkable, especially since this theme is so deeply personal. In previously published papers, this person-centered approach has been stressed as one of the major aspects in this field of research (Bentrott & Margrett, 2011; Murphy et al., 2014; Tarzia, Bauer, Fetherstonhaugh, & Nay, 2013). Therefore, both in content and in study design, the person or participant should be the starting point of all considerations.
This is why we composed a qualitative study to explore the experiences and needs of RCF residents with dementia regarding their love, intimate, and sexual lives. In this paper, we aim to provide insights into the methodology of this study and reflect on its design, procedures, and outcomes. We will also provide a guide to study design based on ideas arising from these methodological considerations. With these insights and guide, we hope to inform and encourage future research on how to include the person-centered perspective for people with dementia.
First, the (theoretical) background is detailed; this was the basis for this study and had significant influence on the design of the data collection. Second, methodological considerations and reflections are described. In this chapter, the methodology of the study is presented, reflections and considerations on the design and execution of the study are described, and both are illustrated using examples from research practice. Third, arising from the considerations, experiences, and reflections, recommendations, and a guide for future studies is composed. We end with a short conclusion.
Background
The World Health Organization defines sexuality as follows:
“Sexuality is a central aspect of being human throughout life encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction. Sexuality is experienced and expressed in thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles and relationships. While sexuality can include all of these dimensions, not all of them are always experienced or expressed. Sexuality is influenced by the interaction of biological, psychological, social, economic, political, cultural, legal, historical, religious and spiritual factors.” (World Health Organization, 2006).
So, despite negative myths and prejudices, intimacy and sexuality remain important for people in old age (throughout life) and is defined as a far broader concept than sexual intercourse alone (Hajjar & Kamel, 2004; World Health Organization, 2006). Although expression, intensity, and frequency of sexual activity can change across the lifespan (Tsatali, Tsolaki, Christodoulou, & Papaliagkas, 2010), Lindau et al. (2007) found that 26% of community dwelling adults between 75 and 85 years of age reported being sexually active (Lindau et al., 2007). Even more fulfillment in intimacy and sexuality was reported by sexually active elderly people compared to younger people, despite the variation in the intensity of the sexual activity (Saga Health, 2011). That older people have a more open mind on the concept of sexuality was suggested to be a factor in this difference between young and old, as they do not solely focus on intercourse, and they tend to include intimate behavior, such as hugging and kissing in their concept of sexuality (Benbow & Beeston, 2012).
Unfortunately, old age is often accompanied by poor health and illness. Dementia is one of the illnesses with an onset that occurs mostly late in life. Although associated with different somatic conditions, dementia always includes memory loss, and eventually a decline of all cognitive and physical functions (American Psychiatric Association, 2000). In addition to dealing with physical and cognitive impairments, suffering from a chronic and deadly disease can cause a decline in QoL itself (Lawton, 1999; Tsatali et al., 2010). Dementia-specific impairments sometimes induce a necessary move into an RCF. This move impacts the lives of people with dementia even more and can be a reason for further decline in QoL (Gonzalez-Salvador et al., 2000). Among many reasons, lack of privacy was found to be a cause for this decline (Gonzalez-Salvador et al., 2000). In that perspective, it is conceivable that intimacy and sexuality cannot be experienced in the same way people were used to when living (together) in their own home (Hajjar & Kamel, 2004). In addition to the privacy barrier, Hajjar and Kamel (2004) suggest other physical and environmental barriers to sexual expression in RCFs, based on a literature review mainly of proxy studies.
Despite these barriers (Hajjar & Kamel, 2004), intimate and sexual behavior is observed in RCF residents with dementia (Archibald, 1998; de Medeiros, Saunders, Doyle, Mosby, & Van Haitsma, 2012; Doll, 2013; Ehrenfeld, Bronner, Tabak, Alpert, & Bergman, 1999; Mayers, 1994; Tzeng, Lin, Shyr, & Wen, 2009; Zeiss, Davies, & Tinklenber, 1996). The interpretation of these reported behaviors varied greatly between the various studies. Perceived models of care, views on intimacy and sexuality, aim of the study, and perhaps the researcher’s individual point of view seem to be factors in these differences. There is, for example, research that focuses on sexual problem behavior and inhibitions (Tsatali et al., 2010), research that includes the responses to intimate and sexual behavior of other residents (Tzeng et al., 2009) and theoretical perspectives and ethical considerations (Bartlett, 2010; Bentrott & Margrett, 2011; Everett, 2007; Kamel & Hajjar, 2004; Mahieu & Gastmans, 2012). In addition to this small body of literature, there is some attention given to the attitudes, perspectives, and education of care staff in research (Benbow & Beeston, 2012; Di Napoli, Breland, & Allen, 2013; Hajjar & Kamel, 2004; Holmes, Reingold, & Teresi, 1997; Tsatali et al., 2010; Ward, Vass, Aggarwal, Garfield, & Cybyk, 2005). Interest in this domain is justified, as nursing home residents with dementia are extensively dependent on their professional caregivers in the specialized psychogeriatric RCF care units. Attitudes and perspectives of said professional caregivers can influence if and in what way residents can express sexuality (Benbow & Beeston, 2012; Hajjar & Kamel, 2004).
Methodological considerations and reflections
Current study
The described study was part of a larger research project, in which we aimed at exploring the experiences and needs of RCF residents with dementia and their spouses, concerning intimacy and sexuality. It was conducted in 2015-2016. Only the study section, which focused solely on RCF residents with dementia, is described below. Dutch RCF residents with dementia were included (see Table 1). These people live in specialized units that contain about six to ten residents in which (small scale) high intensive, 24-hour care is provided. Participants were recruited from three RCFs located in the south of The Netherlands (North-Brabant). The data collection consisted of eight interviews, which yielded rich data.
Participant characteristics
Participant characteristics
*The resident with dementia was male. **The resident with dementia was female. ***Both the male and female dyad of the couple are residents with dementia.
Various aspects of the study were given extensive consideration. For example, as we expected a very small sample size due to the characteristics of the participants and the topic of research, extensive consideration was given to the recruitment, inclusion, and consent process. This was also done in order to shape all steps of the research process in the most person-centered way. In the next section, these considerations will be described and explained. During the execution of the study, not all considerations and choices turned out as expected, and in some areas, adjustments were made during the process. Experiences and reflections on this process are also described below.
A qualitative research design was chosen; specifically, the study was designed according to the Interpretative Phenomenological Analysis (IPA) (Larkin & Thompson, 2012; Smith & Osborn, 2007). This design and analysis methodology was developed to enable researchers to explore people’s experiences, but it also allows a detailed exploration of the way in which people make sense of their own personal worlds. The methodology has been previously used in health psychology research (Brocki & Wearden, 2006; Larkin & Thompson, 2012).
Additional design details were thought through extensively, because of the population under study and the subject at hand. This was done by consulting with experts in clinical practice and by organizing two group discussions to elaborate on the design details and specific ethical considerations. For example, the content of the information letter (Appendix 2), the introduction meetings (Fig. 1), the topic list and question schedule (Appendix 1), and the consent procedure for residential participants were discussed and developed by the research team together with clinical practitioners. Professional caregivers, a care manager, and a psychologist working in an RCF psychogeriatric care unit attended the group discussion.
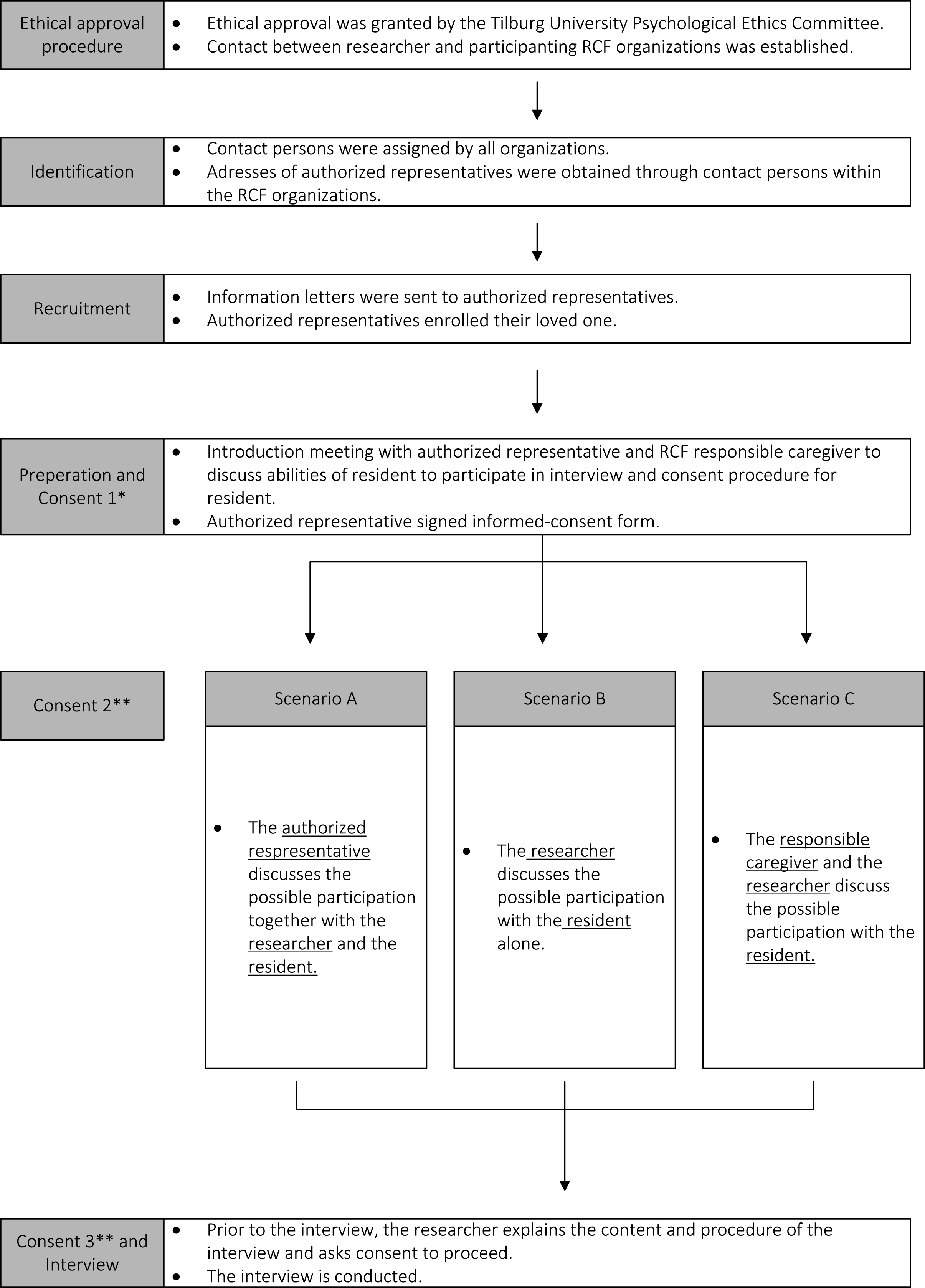
Recruitment, Inclusion and Consent Procedure. *The first consent was obtained from the authorized representative. **Consent was obtained (twice) from the residential participant.
Through the combination of designing the study using the IPA methodology and consulting clinical practitioners, a set of rich data, consisting of both transcriptions of verbal information and field notes of non-verbal information was obtained.
The research proposal was first submitted to the Medical Research Ethical Committee (MREC) in Brabant (Province of The Netherlands), to assess the legal position of this research. In The Netherlands, the Medical Research Involving Human Subjects Act (Central Committee on Research Involving Human Subject, 1998) governs and controls all (medical) research involving human subjects. Although the targeted participants (people with dementia living in RCF psychogeriatric units) are considered legally incapacitated to consent in participation of scientific research in The Netherlands, and the subject of intimacy and sexuality is considered very private and personal, the MREC decided that this Act was not applicable to this research. The research proposal was consequently submitted to another (lower order) ethical committee. Approval was granted by the ethical committee of Tilburg University (reg. nr. EC-2014.27).
Procedure
Recruitment
A stepwise recruitment process was performed (see Fig. 1). First, in the identification phase, a list of potential participants was provided to the researchers by the participating RCF organizations. Close contact between the researcher and the participating organizations, especially the secretary offices, was very helpful in this step of the process.
Second, information letters were sent to authorized representatives of the residents. Due to the considered legal incapacity of the residents suffering from dementia, (informed) consent is needed from an authorized representative before the resident can enroll in scientific research. Partners, children, or other relatives of the resident provided this authorized representation. In some cases, a friend of the resident or legal professional served this role. Through the information letters, the authorized representatives were invited to enroll the person they represent for participation in the study.
Third, in the cases of no response, the researcher (TR) made a follow-up call two weeks after the letter was sent, as was stated in the information letter. In practice, it served as an opportunity for different authorized representatives to discuss their doubts and considerations on enrolling the resident they represented. The actual contact proved beneficial to obtaining sufficient participants for the study, but also in promoting understanding by the researchers of the considerations and dilemmas of the authorized representatives. In hindsight, we assume that authorized representatives were even more precautious in enrolling the person they represent than we had expected. This seems understandable, as it is difficult to decide for another person, especially one who suffers from dementia, to participate in scientific research, particularly on the topic of their intimate and sexual lives.
Inclusion
Introductory meetings were arranged to assess the abilities of the enrolled resident and to decide whether inclusion was possible. The authorized representative, the researcher (TR), and a responsible (professional) caregiver of the RCF were present at these meetings. The responsible caregiver is a member of the unit care staff who is the contact point for resident and the authorized representative. People with dementia who reside in 24-hour psychogeriatric care units are impaired in different cognitive and physical areas. To include these residents in qualitative research in which the data collection consists of semi-structured interviews, specific cognitive and physical abilities have to be sufficient. However, while some people suffer from great communicative impairments, others suffer from memory or executive impairments but are not impaired in their ability to articulate their experiences. Furthermore, the manifestations of impairments and their severity are very individual, and the variability over short periods of time can be great. For these reasons, no objective operationalization of the (dis) abilities was performed. Instead, the impression and view of the authorized representative and the responsible caregiver guided the inclusion process. Some guidelines were followed before the inclusion: residents suffering from moderate to severe communication impairments and residents with severe attention, concentration, and frequently occurring behavioral difficulties were not included.
In this study, no exclusion was performed based on the information obtained in the information meetings. The authorized representatives tended to estimate the abilities of the person they represent sufficiently to decide whether an interview on intimacy and sexuality was possible. However, the inclusion criteria could have been of influence on the results of the study, as only a small portion of the total residential population was able to participate.
Consent
Also during the introduction meeting, written informed consent from the authorized representative was obtained and the procedure for informing and obtaining written informed consent from the resident was discussed. To facilitate the involvement of the resident in the ‘ritual’ of informed consent (Dewing, 2002), the consent procedure was adapted to the individual resident. A two-step procedure in consent (consent 2 and 3 in Fig. 1) was performed. The first step consisted of one of the three consent scenarios (scenarios A, B, C; see Fig. 1) and took place two weeks prior to the interview. The choice between one of these scenarios was made during the introduction meeting, but in all scenarios the presence and participation of the resident was most important. Although most respondents (conceivably) could not remember the information for a period of two weeks, a conventional procedure was chosen, where information of the study is provided in advance of the study to all possible participants (Dewing, 2002; Murphy et al., 2014). The second consent step was performed just before the interview started. Again, the content and procedure information was provided to the residential participant and consent to proceed with the interview was requested. During the study, all possible participants consented on both occasions and decided to participate.
Population
A (convenience) small sample size was obtained (see Table 1), which is both consistent with our expectations and the IPA design requirements (Larkin & Thompson, 2012; Smith & Osborn, 2007). Eight interviews were performed (see Table 1). To obtain a diverse group of people for this study, within the population, no exclusion was performed based on age, sex, marital status, sexual orientation, level of cognitive abilities, or ethnic background. This resulted in a sample of individuals with dementia who were single, or widowed; one couple of two residents with dementia who lived together in the RCF; three couples of whom one is a resident with dementia and the other partner is community dwelling. All participants were heterosexual. The participants did not receive financial compensation for participation.
The interview
Design
To gather data, a flexible approach to the semi-structured form of interviewing was employed. A semi-structured conversational style has been recommended when inquiring about information on sensitive topics (Barriball & While, 1994) from people with dementia (Tarzia et al., 2013), which it is also consistent with the IPA research method (Larkin & Thompson, 2012; Smith & Osborn, 2007). In this way, a balance was established between the information derived from participants on the one hand, and guidance that could be given to the conversation on the other.
Different researchers (Murphy et al., 2014; Smith & Osborn, 2007; Tarzia et al., 2013) provided composition suggestions for the interview schedule. For instance, the topics of the questions were sequenced from least sensitive questions first, progressing to the most sensitive questions last (e.g. introduction; friendship/companionship; love; romance; intimacy; eroticism; sexuality). This was done to make participants more comfortable speaking with the interviewer during the interview and to become more experienced with this study. Participants seemed to feel comfortable speaking about their current experiences in intimacy and sexuality after discussing their love and life history and experiences of their current life in general.
During the course of the data collection, the question schedule was altered due to experiences during interviews. Some questions did not result in relevant information at all, such as questions on romance that followed those about love. Participants tended to not understand the difference between both constructs and the interviewer found it too complex to clarify this difference during the interviews. For individual interviews, the possible exclusion of overly sensitive or difficult topics was discussed during the introduction meeting (see Fig. 1). For example, in the introduction meeting of the couple who both suffer from dementia, it was made clear that this couple never had children. It was discussed whether this was a difficult or painful topic for the couple, which would be better avoided.
Also during the interviews, some adjustments were made to the question schedule and topic list in order to enable participants to express their experiences and opinions in their own way as much as possible. These adjustments were both in terms of content and language. For example, although discussing their intimate life was not a problem, the couple of whom both of the dyad suffered from dementia did not want to discuss their current sexual lives:
“That is something we do not talk about” (couple FG)
Interviewing participants with dementia
The impairments and their variety between participants made the interviewing more challenging, than interviewing people without dementia. Various aspects tended to be important in preparation and execution of the actual interview.
First, a location where people can feel safe and comfortable is very important for interviewing (Smith & Osborn, 2007), especially when the conversation includes sensitive topics such as intimacy and sexuality (Tarzia et al., 2013) and the participant is suffering from dementia (Dewing, 2002). Interviews were held in a comfortable location within the nursing home, mostly in the bedroom of the resident. A “do not disturb” sign on the door provided prevention from interruption and the professional caregiver on duty was also informed that the interview was taking place. Interviewing the residents in their own bedroom was beneficial for another reason. In these bedrooms, residents can keep small personal furniture and belongings, such as pictures or photo albums. These could be used during the interview by both the interviewer and the resident to clarify the context of a story. For example, in one case, a male resident showed a photo album of his 50-year anniversary to the interviewer, to explain his family structure and the fact that his wife died some time after the anniversary.
Second, in this study, an experienced psychologist in dementia care (researcher TR) executed the interviews and her skills in communicating with people with dementia proved to be of importance for the quality of the data. For example, as RCF residents with dementia are not always coherent in their orientation, it is important to recognize their current or changing perceptions in time or place. In this way, a direct estimation can be made of the importance of the information provided by the resident for the current situation, and an intervention can be performed during the interview to restore the perspective in the ‘here and now’ (e.g. waiting, provide information on time and place, asking clarifying questions). For example, in one of the couple interviews, a female resident with dementia temporarily experienced her world as if she and her husband were still in their working life:
“You work as a teacher, right?” (couple CD)
The researcher (TR) could intervene by reminding her how old she is, as her husband just provided that information. Furthermore, despite the exclusion of residents with moderate to severe communicative impairments, some participants were affected in their communicative abilities. This sometimes resulted in vague answers or answers that were difficult to understand. Based on the experience of the researcher, different strategies could be used to clarify the answers or stories participants shared. For example, when discussing the theme of love in one case, the researcher showed a picture of a deceased spouse she found on the bedside of a participant. This helped the participant to put their love story forward as she could confirm that she was talking about her husband. In addition, some participants needed more guidance through the interview. For example, one female participant tended to forget that she was in an interview situation during the interview. The researcher had to remind her of that fact several times. It was, however, important to do this as neutrally as possible, to avoid confrontation of the participant with her disability and possibly feeling distressed or sad about that fact:
Couple FG (F is the female spouse with dementia, I is the interviewer)
F: “Who are you, if I may ask?”
I: “I am TR and I came to interview you both”
F: “Does X (the couples authorized representative) know this?”
I: “Yes, he knows, he gave me permission to contact you.”
F: “Right, what do you want to know?”
This ritual was repeated several times during the interview, but because the resident showed no actual signs of distress, the interview continued. Finally, RCF residents with dementia can be distressed by an interview in general, as questions are asked. This can be ascribed to difficulties in understanding the interview situation, especially as the researcher was unfamiliar to the participants, and to general suspiciousness resulting from the dementia process (American Psychiatric Association, 2000). Recognizing and being responsive to signals of distress, such as physical restlessness, looking anxious or insecure, repeating the same questions in a distressed way, were very important during the interviews. The length of the interview depended solely on the attention and concentration abilities of the participant (s). These were between 20 minutes and one hour. If participants wished to leave, or showed in any other way that they felt uncomfortable with proceeding, the researcher would have stopped the interview immediately. This only occurred once, as a female participant became (physically) restless after 20 minutes of interviewing. In these 20 minutes, she did provide valuable information on the topics and despite the short duration of the interview, the transcript was included in the analysis. In general, during the completion of the interview and ‘handing over’ of the participant to the professional caregiver on duty it was very important to avoid distress as well.
The interviews were audio-recorded using a digital recording device; because of the scaring effect a video camera can have, especially on residents with dementia, we decided not to collect video-material. Before the interview started, the digital recording device was explained to the participants. Notes of non-verbal reactions (field notes) were made during and after the interview by the researcher and were included in the transcription.
In conclusion, the location of the interview, observational contact, communication skills of the interviewer/researcher, and the choice of recording device proved to be important to the course of the interviews and the information obtained therefrom.
Data analysis
Understanding the content and complexity of the personal world of the participant was the main goal of the described study. An ‘interpretative relationship’ with the obtained information was engaged by the interviewer (Smith & Osborn, 2007). The complete transcription, including notes and observations, were considered data for analysis. This method of analysis was chosen in order to reveal the richness of the data and to overcome possible ambiguity of the verbal reactions. The analysis procedure was further constructed in accordance with the IPA guidelines (Larkin & Thompson, 2012; Smith & Osborn, 2007).
Despite the inclusion of the observations and notes, ambiguity was still experienced in the process of analysis. As one researcher performed the interviews (TR), the critical peer reviewer (KL) sometimes missed information regarding the context and course of the interview. This complicated the analysis process in some cases, as the first researcher was the only one present in the interviews and analysis. Thorough discussion among the authors was needed to clarify these ambiguities and reach consensus on the codes and themes constructed. For example, in interviews with couples where one of the dyad members was resident in the RCF, the healthy spouse sometimes provided more information and offered clarification on something the participant with dementia said. This was, however, done in a way in which the healthy spouse bent over to the interviewer and ‘whispered’ the information to the interviewer, to prevent the participant with dementia being confronted with the fact that they were being corrected. We did, however, feel that conducting the interview with more than one interviewer would have had great disadvantages with respect to the course of the interviews, which would have been consequential to the information obtained. Most of the important aspects in interviewing participants with dementia (described before) depended exclusively on the nature of contact between the interviewer and participant.
Through the analysis, it became manifest that participants tended to discuss the topics of intimacy and especially, sexuality in a figuratively and sometimes ‘covered’ way. Proverbs, sayings, and even song lyrics were used by the participants to describe their experiences and personal worlds. It was, however, not possible most of the time, to ask the participant for clarification during the interview. For example, the male participant of the couple who both live in the RCF described their sexual historyas:
“Yes, we grew up together” (Couple FG).
And the single male participant described his former sexual life as:
“Just some fooling around” (Participant A2).
Even more implicit, was a well-known Dutch folk song that the female individual participant sang during the interview:
“Good were those days, in which we were young and together” (literal translation, Participant A1).
In addition, the interviews were held in Dutch. As research reports are written in English, translation was conducted during the writing process of results section of the research paper. Supplementary to the valid considerations this type of translation usually has in qualitative research, due to the figurative and ‘covered’ statements of the residents, this was even more challenging, and required extensive consideration. Some proverbs or sayings given by the interviewees were specifically Dutch, and when translated into English, the underlying feeling or meaning that Dutch speakers would ascribe to the statement is no longer apparent. Extensive explanation of the context and the underlying feeling or meaning in the research reports is then necessary, but challenging, especially when considering the complexity of language and practical issues, such as limitations in allowed length of research reports.
Study quality
There has been debate on how to achieve a sufficient level of quality in qualitative research in general. While the quality of quantitative research derives from reliability, validity, generalizability, and objectivity (Gibson, Timlin, Curran, & Wattis, 2004), achieving quality in qualitative research is more complex. Devers (1999) composed equivalent criteria to enhance ‘rigor’ in qualitative research (Devers, 1999). To meet these criteria and enhance ‘rigor’ and thus the quality of the described study, different techniques were performed (Boeije, 2012; Devers, 1999; Mays & Pope, 2000).
First, in order to enhance the ‘external validity’ (Devers, 1999), a clear and extensive description of the data collection and analysis was reported during and after the study. For this study specifically, due to the important role of the researcher, this does not enable exact replicability. However, transferability was enabled (Devers, 1999).
Second, ‘reflexivity’ (Devers, 1999) was used to ensure attention to this aforementioned important role of the researcher. Personal characteristics of the researcher and description of the researcher-participant relationship were considered and included in research reports to enhance ‘objectivity/confirmability’ (Boeije, 2012; Devers, 1999). The researcher and interviewer was a 29-year-old woman. In addition to research work, she worked as a psychologist in one of the RCFs in which the study took place. However, this researcher was not clinically responsible or involved in the selected units where the recruitment for the study took place. This researcher was responsible for the recruitment process and conducted all the interviews.
Third, two critical peer reviewers (KL, PE) played the part of ‘devil’s advocate’ (Devers, 1999) in the complete research process. They asked critical questions on research methods, design, analysis, and interpretation of the data. Consequently, this enhanced the ‘dependability/reliability’ in this study. In addition, a peer reviewer performed the co-coding process (KL).
However, one commonly used technique for enhancing study quality was not possible to engage with, due to the characteristics of the participants. No member checks (e.g. receiving feedback from research participants on transcripts or abstracts of interviews) were performed in this study, as we expected that participants, due to memory impairments (American Psychiatric Association, 2000), were not able to provide the researchers with a reliable answer.
Limitations, guides and recommendations for study design
Limitations, guides and recommendations for future study design deriving from the above-described methodological considerations and reflections are presented in chronological order of study design (see also Appendix 3).
Preparation
During the design of the study, professionals from clinical practice were closely involved. This proved to be very beneficial in terms of the methodological and ethical considerations; the practical execution of the study and the support base for the study in practice. It also complements recommendations from prior studies (Dewing, 2002; Tarzia et al., 2013). Combining the views of experienced researchers, with those of experienced professionals from practice in the preparation phase is there for strongly recommended for future research, especially when the population under study is vulnerable.
Furthermore, putting extensive thought in every step of the process, and reporting these steps beforehand, proved to also be, beneficial. However, this should not compromise the flexibility in the execution of the study. Flexibility, such as adjusting the interview schedule, proved to be very important, especially considering the variety in participants’ characteristics.
Although, both the topic list and the question schedule were exclusively composed for this study (see Appendix 1), they were not pre-tested because of the small sample size and effort to recruit these participants in the first place. In addition, pre-testing of the interview schedule was not expected to be of any added value, due to the variety within participants, and even more so, the variety in impairments and lingual possibilities of the participants. This can be considered as a limitation as it could have influenced the results.
Procedure
The introduction meeting (see Fig. 1) proved to be very important to perform a person-centered recruitment, inclusion and consent procedure, which was stressed to be important before (Bentrott & Margrett, 2011; Murphy et al., 2014; Tarzia et al., 2013). A customized inclusion process in which personal characteristics could be taken into account, helped the researcher to estimate whether the possible participant was able to participate, without the need to quantify cognitive functions and possibly cause further distress in the participant. In addition, quantification of cognitive functions, using a cognitive screening for example, was expected not to predict the actual possibilities of the resident to participate in an interview. Furthermore, the introduction meeting enabled customization of the consent process that contributed to obtaining informed consent comfortably from both the authorized representative and the residents with dementia (see Fig. 1).
The authorized representatives and responsible caregivers were intensively involved in the recruitment and inclusion process. These people are closely involved in the life and care of the residential participant on a daily basis. Their views and opinions were considered of great value in the decision process. However, participating residents were not involved during the first steps of recruitment and consent (see Fig. 1), and exclusion from the study was still possible after the introduction meeting. This can be considered as a limitation regarding the person-centeredness of the recruitment and inclusion process. However, with this approach we prevented a situation in which the resident would agree with enrolment, but the authorized representative disagree, resulting in the resident not participating, which could lead to confusion or distress in the resident.
On interviewing people with dementia, suggestions were made in prior research (Devers, 1999; Murphy et al., 2014; Tarzia et al., 2013), which proved to be beneficial (e.g. sequencing the interview guide; a comfortable location to interview; profound skills of the interviewer). We however experienced that especially the skills of the interviewer were very important to the process and outcome of the results. To interview people with dementia, who live in an RCF, profound knowledge on dementia and skills to guide a conversation, observe and take action on vague or non-verbal signals of distress and flexibility proved upmost important. In addition, the interviewer had to combine these actions, with the data collection, which can be seen as the primary task and can be a great limitation. However, the direct contact and individual contact between interviewer and participant proved to be very beneficial to the outcome and a strength of this described study.
Data analysis and study quality
Although no video material was collected, which can be considered a limitation; field notes on a range of non-verbal outings were included in the analysis. This proved to be of great value during the data analysis, as only one researcher was present during the interviews and the non-verbal information was at least as important to provide context to the content of the interviews, as the transcriptions of verbal information. The impairment of the participants sometimes impeded providing further verbal explanation and so non-verbal information was very important. Also information from the introduction meetings was important to provide context.
Enhancing ‘rigor’ in qualitative research when residents with dementia are participants proved to be challenging. Balance between study quality and practicability tended to be necessary when dealing with these participants and this research topic. Although different techniques (Devers, 1999) to enhance ‘rigor’ were performed (see study quality), several proposed techniques were not possible, due to (memory) impairments in participants, such as performing member checks or performing triangulation (Devers, 1999).
Conclusion
The person-centered perspective was rarely represented in research on intimacy and sexuality in RCF residents with dementia (Roelofs et al., 2015). Through the described study, we aimed at including this perspective as much as possible. To achieve this, the person-centered perspective served as a base for methodological choices and design details. This necessitated a flexible, creative, out-of-the-box approach through the course of the study. Although various dilemmas, challenges, and difficulties were faced, the value of the rich and personal data that were obtained, confirmed the idea of the starting point of the study: it was worthwhile.
Different recommendations and guides for future studies are provided. We hope this will be informative and will encourage researchers to include the person-centered perspective in future research and care policy for this important theme. However, the goal to include the person-centered perspective is not exclusively reached by the choices and approaches described, but can be seen as a first step in this direction.
Conflict of interest
None to report.
Footnotes
Appendix 1
Question Schedule
| Topic | Questions |
| Introduction | Welcome |
| Do you have any questions in advance? | |
| friendship/companionship | Can you tell me what friendship or companionship means to you? |
| Do you experience friendship in any way, lately? | |
| If so? In what way? | |
| What does that mean to you? | |
| love | Can you tell me what love means to you? |
| Have you been experiencing love lately? | |
| In what way? | |
| What does that mean to you? | |
| romance | Can you tell me what romance means to you? |
| Have you been experiencing romance lately? | |
| In what way? | |
| What does that mean to you? | |
| intimacy | Can you tell me what intimacy means to you? |
| Have you been experiencing (physical or non-physical) intimacy currently? | |
| Are you experiencing any barriers to experiencing intimacy? | |
| What does that mean to you? | |
| eroticism | Can you tell me what eroticism means to you? |
| Have you been experiencing eroticism lately? | |
| May I ask you in what way you have experienced eroticism lately? | |
| What does that mean to you? Is it important to you? | |
| sexuality | May I ask if you have been experiencing sexual contact lately? |
| Are you experiencing any barriers to experiencing sexual contact? | |
| And in what way? | |
| What does that experience mean to you? | |
| Closing | Do you even discuss any needs in intimacy or sexuality with anyone? |
| (e.g., partner, children, responsible caregiver, psychologist, doctor) | |
| What do you think of the way the unit/caregivers handle issues in this area? | |
| Do you have any more needs in your experience in these areas? | |
| Is there, for example a proper place to experience intimacy the way you prefer? | |
| Do you still have any questions or comments? | |
| Thank for participation |
Appendix 2: Information Letter
Dear Sir/Madam,
We send you this letter, because we want to kindly ask you to participate in a study.
The study is titled: “Intimacy and Sexuality in the Nursing home.”
We are researchers of Tilburg University.
Tineke Roelofs will conduct the study within (Name of the RCF organization).
She works as a researcher, and also as a psychologist and is experienced in talking about private matters with people with dementia.
You decide for yourself if you want to cooperate. Before you decide, it is important to know more about the study. We therefor ask you to (calmly) read this letter.
The study concerns the importance of intimacy and sexuality in people’s lives.
And in this study, especially on the importance for people with dementia who live in a nursing home, and their partners.
The researcher really wants to know from the people with dementia themselves, how they experience intimacy and sexuality in their current life, and if they have any further needs and wishes in this area.
Intimacy and sexuality are important aspects of life. When people get older, suffer from dementia, or move to a nursing home, this can be of great influence on their experience of intimacy andsexuality.
This is, however, never studied before.
Through the information derived from the study, we hope to inform practice on experiences, needs and opinions of people with dementia themselves.
Participation in the study will not lead to actual changes in your current situation. However, in the long-term, we can use the results to improve the quality of care and to adapt the care process to the experiences of people with dementia.
The researcher will conduct interviews with people with dementia, and if possible, with their partners. You largely decide the content of the interview yourself.
Your experiences and opinions are most important.
The researcher will, by any means, ask you about the importance of intimacy and sexuality in your life. She will also ask you questions about the possibilities to experience intimacy and sexuality within your current situation, possible barriers and the way professional caregivers deal with this subject.
The interview will take between 20 minutes to one hour and will be audio taped.
Before we can start the interview, an introduction meeting will take place. In this conversation your partner or authorized representative, your responsible caregiver and the researcher will discuss how the interview can best be conducted.
You decide yourself, if you want to participate in the study.
Participation is voluntary.
If you do not want to participate, you do not have to tell why.
If you want to participate, you also do not have to tell why. You will get a consent form from the researcher, for you to sign.
You can, of course, change your mind at any point and stop, also during or after the interview.
The audiotapes of the interview, are handled confidentially. They will only be used for this study. Your participation and everything you tell the researcher will not be shared with, for example, your responsible caregiver, your doctor or family.
We use data-coding to prevent that the interviews can be traced back to your person.
Only the researcher has access to these codes.
We are obliged to save all the data for 15 years. You will consent with this procedure, if you participate in the study. If you do not want that, you cannot participate.
The interviews will take place between (depended on the organization).
The interview will be planned, when it suits your agenda.
When you have any remaining questions, you can always contact the researcher: Tineke Roelofs (contact details see below)
When all the interviews are conducted, the researchers will write scientific reports about them. Naturally, your name will not be mentioned in these reports.
If you are interested in these (English) reports, it is of course possible to receive a copy.
You will always receive a newsletter in Dutch, to inform you on the results.
Finally, the results from the interviews will be included in a doctoral thesis. Also in this thesis, your name will not be mentioned.
You can discuss the participation with anyone you want, for example your partner, your children or other relatives.
Do you have any remaining questions, after reading this letter? You can always contact the researcher: Tineke Roelofs
You can contact here through (phone number) and (email address).
Tineke Roelofs (affiliations)
Prof. Dr. Katrien Luijkx, (affiliations) and prof. Dr. Petri Embregts (affiliations)
(name of the RCF organization)
Appendix 3
Guide and recommendations for study design
| Preparation | |
| Close involvement of clinical practice in study design, methodological and ethical considerations. | •The design details connect closely to the practice situation, which contributes to the complete procedure of the study. |
| Extensive thought and consideration in design and methodology. | •Putting extensive thought and consideration into every step of the design and methodology contributes to successful and smooth progress of the study. |
| •Reporting these all steps beforehand proved to be of value. This report should not compromise flexibility in the execution of the study procedure. Flexibility is important, especially considering the participants’ characteristics. | |
| Procedure | |
| Investment in direct contacts with clinical practice and authorized representatives. | •Contact on management level, but especially on the level of secretary offices and professional caregivers proved to be convenient. |
| •Where information letters can provide general information on the content and procedure of the study, during direct contact with authorized representatives, remaining questions can be answered and considerations and worries can be discussed. | |
| The introductory meeting; inclusion and consent. | •A customized inclusion process in which personal characteristics could be taken into account helps the researcher to estimate whether the possible participant was able to participate, without the need to quantify cognitive functions. |
| •A customized consent process contributed to obtaining informed consent comfortably and easily from the residents with dementia. | |
| Person-centered inclusion and consent. | •In order to include residents with dementia as much as possible in the study and procedures, and facilitate the authorized representatives to do the same, the information letter was composed in such a way that the most possible participants could understand the information. Also, the two-step informed consent procedure for residential participants was performed for this reason. |
| Interviewing participants with dementia. | •The sequencing of interview questions from least sensitive to most sensitive proved to be effective in building up a rich, informative interview. |
| •The skills of the interviewer proved to be very important. Experience in contact and communication with residents with dementia was necessary. | |
| •A location where the resident can feel comfortable and ‘at home’ tended to be very important for the course and outcome of the interview. A location set in the bedroom of the resident proved to be convenient, as personal belongings of the resident (e.g. pictures) could be used to clarify information during the interview. | |
| •The duration of the interviews should be adapted to the characteristics and impairments of the residential participants. Contact with and good observation of verbal and non-verbal signals is necessary to estimate whether the interview can continue or should be ended. | |
| Data collection. | •The interviews were performed by one researcher, without a camera or extra observer. The interviews were audio-recorded with a small recording device and the researcher made field notes that enriched the data greatly. |
| •A flexible approach to semi-structured interviewing helped to avoid distress in the resident and improved the outcome. | |
| Data analysis and study quality | |
| Field notes. | •The inclusion of field notes in the transcriptions proved to be of great value to interpretation during data analysis. Also the information from the introductory meetings was important to provide context. |
| Enhancing study ‘rigor’. | •Enhancing ‘rigor’ in qualitative research when residents with dementia are participants proved challenging. Balance between study quality and practicability is necessary when dealing with these participants and this research topic. |