
Abstract
OBJECTIVES:
The purpose of this study was to confirm the intra-rater reliability and absolute reliability of Lissajous Index (LI) in evaluating the symmetry of trunk movement during gait in patients with stroke and to examine the relation between LI and body function in patients with stroke.
METHODS:
Twenty-one healthy subjects (11 males and 10 females, age 63.3±2.0 yrs) and 45 patients with stroke (33 males and 12 females, age 58.7±13.4 yrs) were included in the study. The accelerometer was fixed to a belt at the level of the L3 spinous process. The 10-m walk test was performed twice to record definitive data on trunk acceleration. LI was calculated from trunk accelerations. We confirmed the intra-rater reliability and absolute reliability of LI in patients with stroke and we examined the relation between LI and body function in patients with stroke.
RESULTS:
There was no fixed bias and proportional bias in the LI of patients with stroke. It was found that BBS significantly correlated with LI in stroke patients (p < 0.05, r = –0.413).
CONCLUSIONS:
It was clear that LI during gait was effective at evaluating gait symmetry and balance. LI was indicated to be useful in evaluating gait in patients with stroke.
Introduction
Factors that can cause walking defects among patients after a stroke include motor paralysis, sensory impairment and changes in muscle tone. Therefore, gait in stroke patients quickly becomes asymmetrical. Walking with asymmetric stride-times requires more metabolic power than symmetric walking at comparable stride-times (Ellis et al., 2013). Gait asymmetry is recognized as a key to understanding post-stroke deficits in gait and to improving the rehabilitation process in order to maximize mobility after a stroke (Shull et al., 2014; Meijer, Plotnik, Zwaaftink, van, Lummel, Ainsworth, Martina, & Hausdorff, 2011; Alexander et al., 2009).
Recent studies have reported that, gait analysis using tri-axial accelerometers has many advantages and reliability of measurement. A skin-mounted accelerometer can accurately reflect the acceleration of the joint (Miyazaki et al., 1998). In addition, a tri-axial accelerometer is easy to use because it is lightweight and presents no obstructions. Various gait parameters, as well as the regularity and symmetry of the gait, can be computed from data gathered by an accelerometer of the trunk. The harmonic ratio has been used as an indication of the rhythm and symmetry of the acceleration patterns; frequency analyses of the acceleration signals have been used to quantify the harmonic ratio (Brach et al., 2011).
The Lissajous Index (LI) visually and numerically evaluates the left-right symmetry of a Lissajous Figure (LF); this LF is made from trunk acceleration data (Yamaguchi, Hirata, Doi, Asai, Inoue, Makiura, Ando, Kurosaka, & Miura, 2012). The center of gravity (COG) in the human body exists at the level of the L3-4 spine and the accelerometer at the level of the L3 measures the acceleration of the COG (Moe-Nilssen, 1998). The LF is thus indicative of movements of the virtual COG as it is made from accelerations measured by the accelerometer at the level of L3.Yamaguchi et al. determined that healthy older people have more asymmetry of the left-right trunk movement than healthy younger people (Yamaguchi et al., 2012). Kagawa et al. found that left-right trunk symmetry during walking of patients with hip osteoarthritis improves after total hip replacement (THA) (Kagawa, Chida, Kimura, Maeda, Mabuti, & Doumen, 2009). Hence, the LI has been fined useful for healthy subjects and for patients with hip osteoarthritis, but the LI has not been evaluated or adjusted for patients with stroke.
The purpose of this study was to confirm the intra-rater reliability and absolute reliability of LI in evaluating the symmetry of trunk movement during gait in patients with stroke, to compare the LIs of patients with stroke with those of healthy subjects, and to examine the relation between LI and body function in patients with stroke.
Methods
Subjects
Twenty-one healthy subjects (11 males and 10 females, age 63.3±2.0 yrs) and 45 patients with stroke (33 males and 12 females, age 58.7±13.4 yrs) were included in the study (Table 1). The following patients were excluded: 1) patients who were not able to walk by themselves without canes, 2) patients with illness or injuries other than stroke that impaired their behavior and 3) patients who did not understand the purpose of the experiment. The Brunnstrom recovery stage of legs in the patients with stroke was classified as3 of 7, 4 of 13, 5 of 16 and 6 of 9.
The features of subjects
The features of subjects
Mean±Standard Deviation (SD) or Median (Interquartile range).
This study was reviewed and approved by the Ethics Committees of Akita University Graduate School of Medicine (2015) and Akita Prefectural Center for Rehabilitation and Psychiatric Medicine (2015), and was carried out according to the Declaration of Helsinki. Written consent was obtained from all participants.
Tri-axial accelerometer
The small wireless tri-axial accelerometer (MG-M1110; LSI Medience Corporation, Tokyo) (Yoneyama, Mitoma, & Okuma, 2013a; Yoneyama, Kurihara, Watanabe, & Mitoma, 2013b) had a length of 75 mm, height of 50 mm, width of 20 mm and weight of 120 g. The sampling rate was 100 Hz. The accelerometer was used to measure the vertical (VT), anteroposterior (AP), and mediolateral (ML) acceleration of the trunk during gait. Each aspect of acceleration was indicated by graphs using the analysis software for personal computer (MG-M1110-PCTM; LSI Medience Corporation, Tokyo) (Yoneyama et al., 2013a; Yoneyama et al., 2013b). This software calculated the steps, gait speed and gait coefficient of variation and exported the values of each aspect of acceleration into Microsoft Excel (Excel).
Accelerometry procedures
The accelerometer was fixed to a belt at the level of the L3 spinous process. The 10-m walk test was performed twice to record definitive data on trunk acceleration. A 10-m-long walkway with a 1-m spare walkway area at both the start and end was constructed. All subjects were instructed to walk straight at a self-selected comfortable speed towards a target line on the floor. Eight patients with stroke who would not be able to walk otherwise used an ankle-foot orthosis.
Methods of making a LF (Yamaguchi, 2012)
All acceleration data from the 10-m walk was used, except for the first and final steps. Using Excel, the LF was graphed on a scatter chart with the y-axis representing VT acceleration and the x-axis representing ML acceleration. Figure 1 shows the LF made from actual measured values of trunk acceleration.
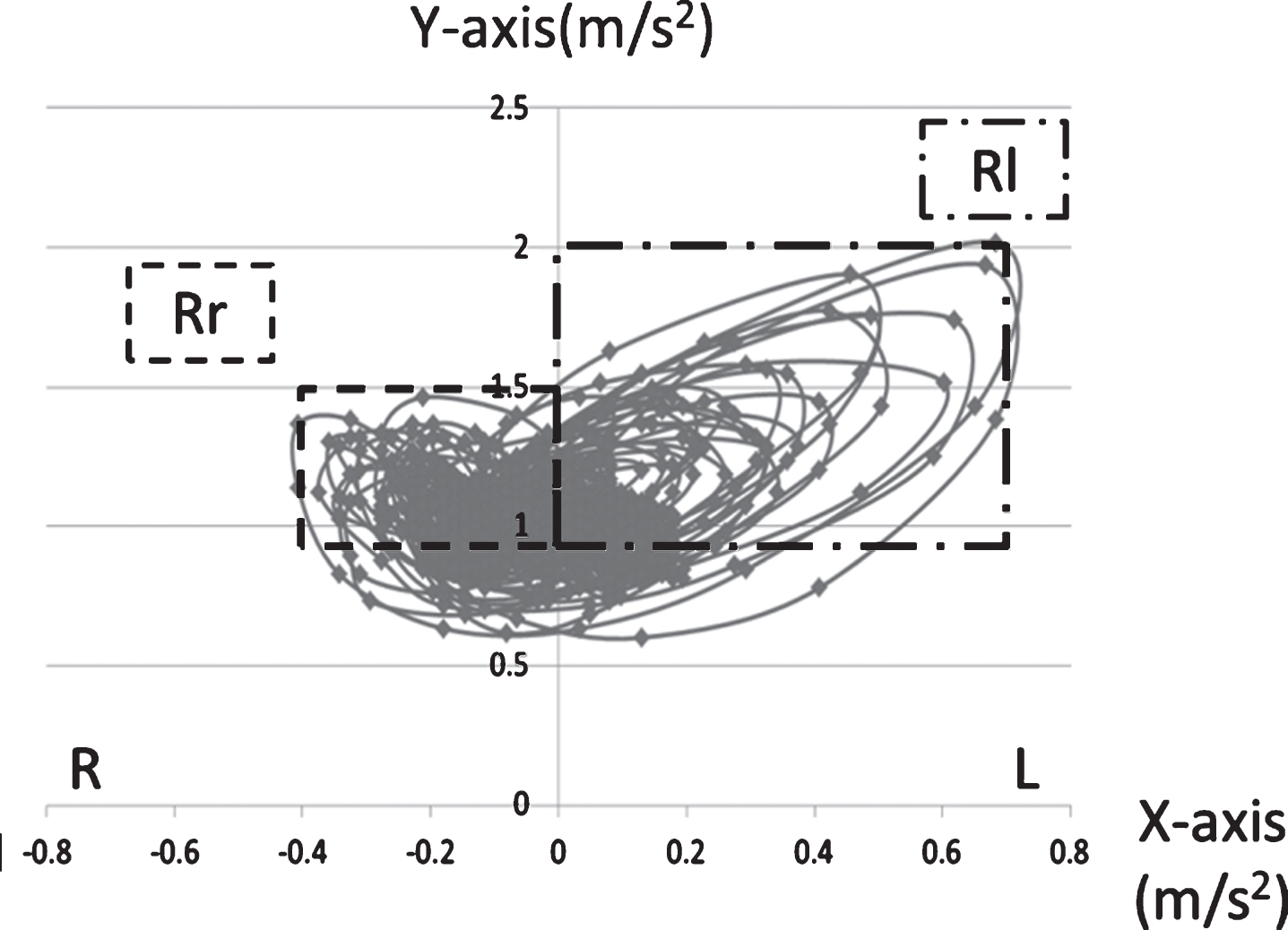
Lissajous Figure.
The quadrangle surrounded by undulating line (Rr) and the quadrangle surrounded by undulating and dotted line (Rl) were the calculated areas (Fig. 1).
The formula for calculating LI is shown below.
A large value of LI indicates asymmetry and small values of LI denotes symmetry on the frontal plane.
Motor function
Recovery was evaluated with the Brunnstrom recovery stage (Br.stage) (Brunnstrom, 1966), disorder of sensation was evaluated with Stroke Impairment Assessment Set (SIAS) (Chino et al., 1997), muscle tone of the paralysis-side leg was evaluated with Modified Ashworth scale (Bohannon & Smith, 1987), muscle strength with isokinetic contraction movement of knee extension, flexion with CYBEX (Medica Corporation, Fukuoka), strength of trunk with Manual Muscle Testing (MMT) (Helen & Montgomery, 2008), standing balance with the Berg Balance Scale (BBS) (Berg, Wood-Dauphinee, William, & Maki, 1992), and the performance of movement with Motor Age Test (MOA) (Johnson et al., 1951). Additionally, the maximum gait speed and comfortable gait speed were evaluated. Isokinetic muscle functions of knee extension and flexion were measured at 60°/s by the ratio of body weight.
Statistical analysis
Intra-rater reliability and absolute reliability of LI in patients with stroke
The Intra-rater reliability between LI of the first time and the second time was examined using an intraclass correlation coefficient (ICC). ICC values >0.75 are considered to have “excellent reliability” and values between 0.4 and 0.75 are considered to have “fair to good reliability (Shrout & Fleise, 1979). To test the absolute reliability of the LI for patients with stroke, we used the Bland-Altman analysis method (Bland & Altman, 1986). There was no fixed bias if the 95% confidence interval (95% CI) included 0. If the t-value was calculated from the actual measurements using a correlation coefficient, a t-value in the degree of freedom ‘n – 2’ suggested that proportional bias did not exist. We also calculated the minimal detectable change of the 95% confidence interval (MDC95) to identify the clinically permissible level.
Comparison of LIs of healthy subjects and patients with stroke
To compare the LIs of healthy subjects with those of patients with stroke, the Mann-Whitney U test was used.
Examination of the relation between LI and body function in patients with stroke
Pearson’s product-moment correlation coefficient or Spearman’s rank correlation coefficient was used to find the body function that have an effect on the LIs of patients with stroke.
PASW Statistics 18 (SPPS Inc, Chicago, IL, USA) was used for statistical analysis (level of significance p < 0.05), but Bland-Altman analysis was excepted. The Bland-Altman analysis was followed the procedures used in previous studies and calculations were entered into Excel (Bland & Altman, 1986).
Results
Intra-rater reliability and absolute reliability of LIs in patients with stroke
The ICC of the LI for patients with stroke was 0.938 (p < 0.05). Figure 2 shows the Bland-Altman plots and Table 2 illustrated the results of the Bland-Altman analysis. In the Bland-Altman analysis, the 95% CI was – 4.77 to 3.11. There was no fixed bias in the LI of patients with stroke because the 95% CI included 0. In this study, we calculated the t-value from the actual measurements using a correlation coefficient. The t-value in the degree of freedom ‘43’ was 2.015. The t-values measured were 0.739, which were less than 2.015, suggesting that proportional bias did not exist. Since there was no systematic error, MDC95 was calculated as 25.7%.
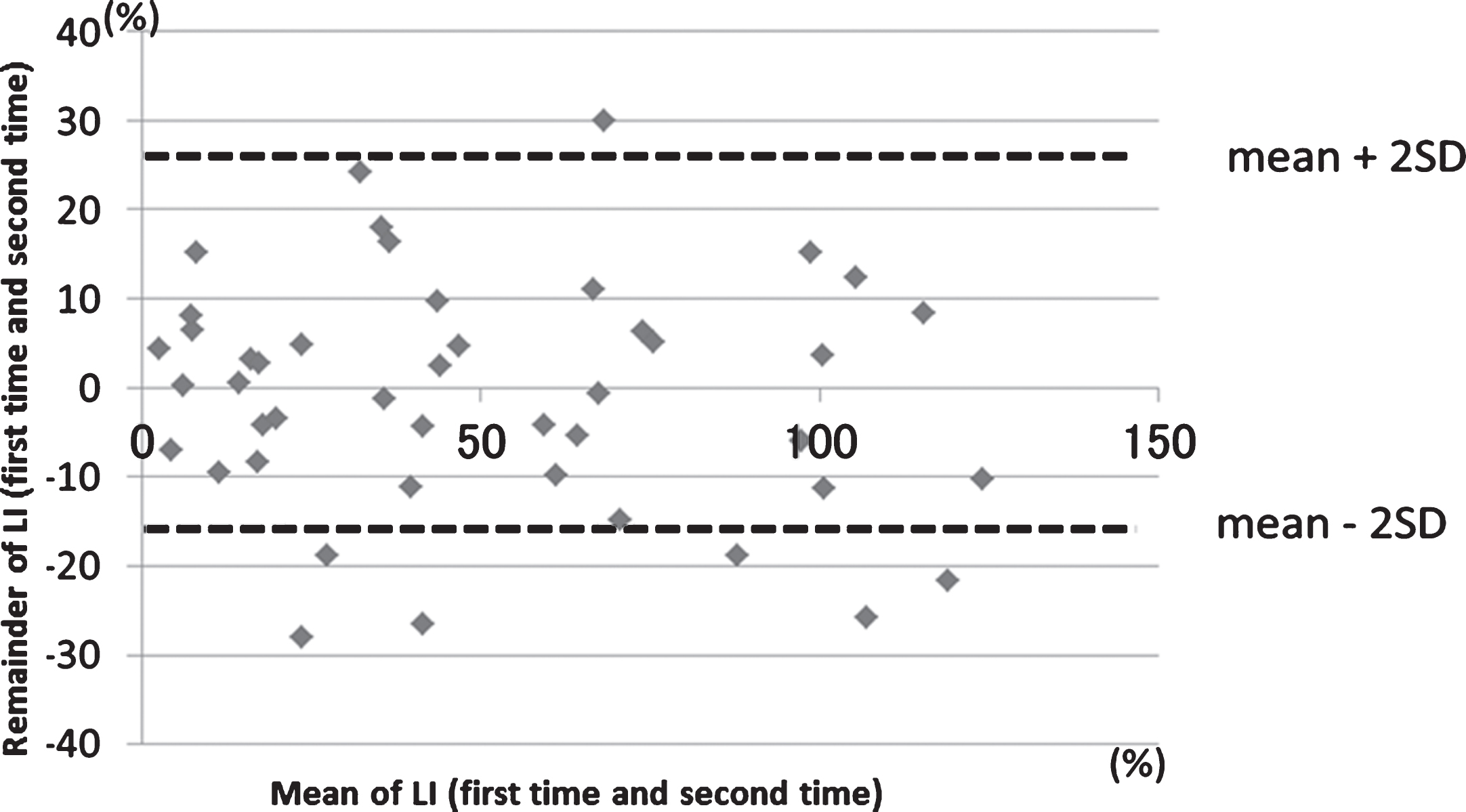
Bland-Altman plot (patients with stroke).
Results of Bland-Altman analysis
Figure 3 shows the actual LF of healthy subjects and patients with stroke. From this figure, it is clear that the LFs of the patients with stroke were larger and more asymmetric than the LFs of the healthy subjects. The means and SDs of LIs in healthy subjects and patients with stroke were 21.1±14.1% and 51.2±37.6%, respectively. The Mann-Whitney U test found that the average LI of the patients with stroke was significantly larger than that of healthy subjects (p < 0.01).
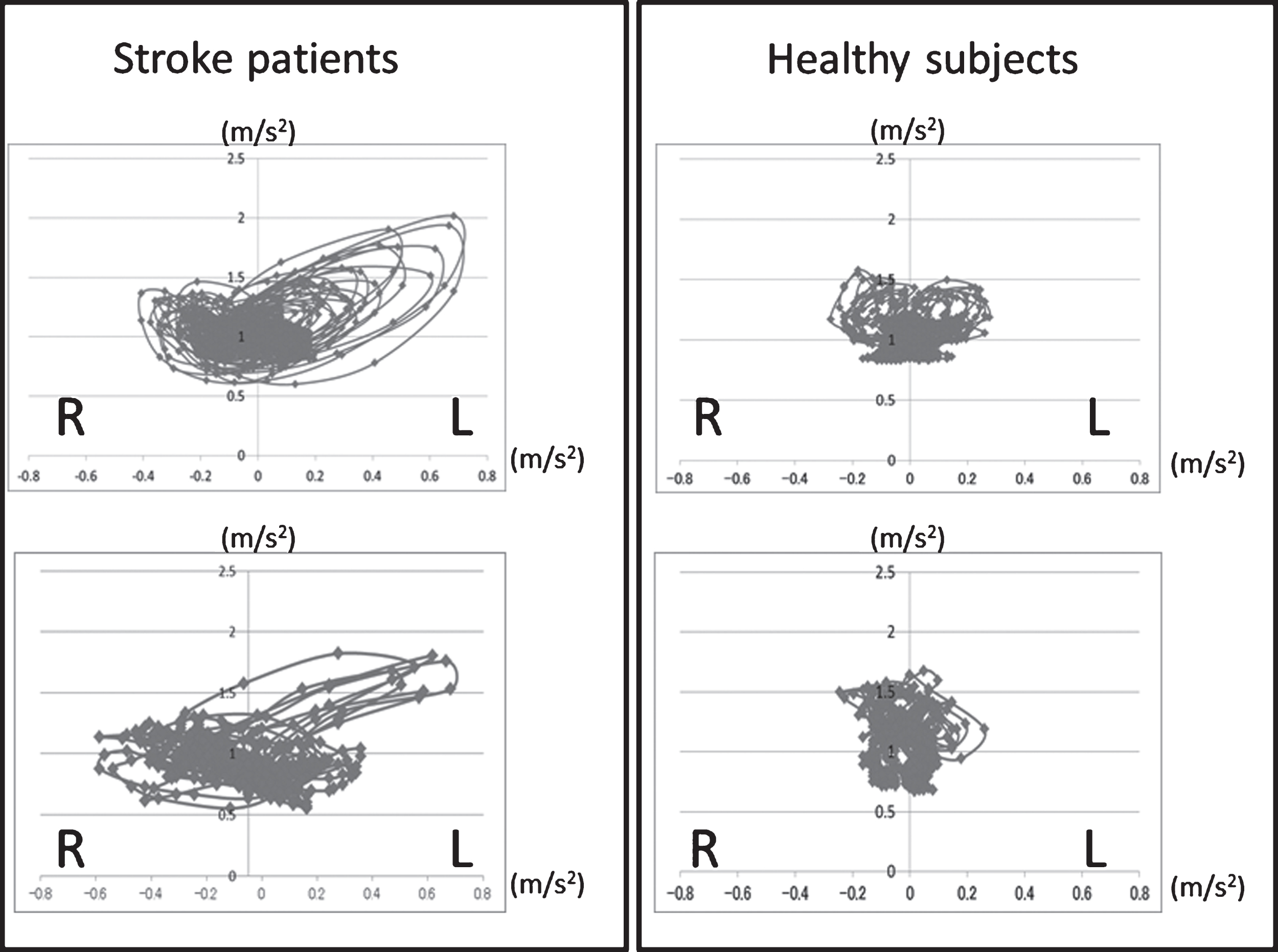
Actual Lissajous Figure.
Possible correlations between various types of body functions and LI were examined to identify what body functions were influenced by LI. It was found that BBS significantly correlated with LI in stroke patients (p < 0.05, r = –0.413) (Table 3).
LI and Motor function
LI and Motor function
*p<0.05. Muscle tone: Modified Ashworth scale, Deep sensation: Stroke Impairment Assessment Set Pearson’s product-moment correlation coefficient or Spearman’s rank correlation coefficient
Studies of left-right symmetry in stroke patients almost always focus on the legs (Meijer et al., 2011; Hollands et al., 2016; Schiemanck et al., 2015; Burnfield et al., 2016). In stroke patients, both leg movement and trunk movement in walking become asymmetrical. However, few studies have examined left-right symmetry of trunk movement in stroke patients (Meijer et al., 2011).
Presently, the symmetry of trunk movement during walking is typically evaluated by the three-dimensional motion analysis system (Henriksen, Lund, Moe-Nilssen, Bliddal, & Danneskiod-Samsoe, 2004; Howell, Osternig, & Chou, 2015). Unfortunately, this system is very expensive and only measures gait in a limited environment (Henriksen et al., 2004; Howell et al., 2015). The number of hospitals having the three-dimensional motion analysis system is also quite limited because the system itself is very large.
Meanwhile, measuring LF and LI using a tri-axial accelerometer is both affordable and feasible. With these tools, LF and LI can be measured in any setting and can evaluate symmetry of trunk movement during walking (Yamaguchi et al., 2012). It is quick and simple to place a tri-axial accelerometer on a patient’s back to measure gait asymmetry (Yamaguchi et al., 2012). Acceleration measured by a tri-axial accelerometer at the level of L3 represents the acceleration of the virtual COG; therefore, LF can provide a visual marker of the symmetry of the virtual COG during gait. And while LF is useful for providing feedback to patients, LI can quantify the LF symmetry, and track changes in COG symmetry over time. Patients with THA are easily able to understand the results of this examination (Kagawa et al., 2009). Therefore, LF and LI are useful in a clinical setting. Surprisingly, the usefulness of LF and LI in patients with stroke has never before been examined. The purpose of present study was to examine the availability of LI included in the evaluation of symmetry for trunk movement during gait in stroke patients.
First, we confirmed the intra-rater reliability and absolute reliability of LI in patients with stroke. Second, we compared the LIs of patients with stroke with those of healthy subjects. Next, we examined the relation between LI and body function in patients with stroke.
Intra-rater reliability and absolute reliability of LI in patients with stroke
Our results showed that LI in stroke patients has a high reliability because the ICC of LI in stroke patients walking 10 m at comfortable speed was 0.938 (>0.75). In addition, Bland-Altman analysis showed the absolute reliability of LI in stroke patients because no fixed bias or proportional bias was found. The constancy of gait declines in patients with stroke, and it has been proposed that maximum gait speed is well suited for the evaluation of gait in stroke patients in terms of reliability (Wade, Wood, Heller, Maggs, & Langton Hewer, 1987). While maximum gait speed has high reproducibility in stroke patients (Wade et al., 1987), LI is able to measure symmetry of stroke patients during walking and is less stressful for the patients, both physically and mentally. LI measured at comfortable gait speed proved to be useful in evaluation of symmetry for trunk movement during gait in stroke patients. Furthermore, since comfortable gait speed is the gait speed of daily life (Kuroki, 1982), LI measured in this context is more relevant to the walking done in daily life.
Comparison of LIs patients with stroke and those of healthy patients
The present study indicated that LI of patients with stroke was significantly larger than that of healthy subjects. The step length and step time of stroke patients show more asymmetry than those of healthy subjects (Iosa et al., 2016; Dobkin et al., 2011); our study showed that acceleration of trunk movement reflects these asymmetries well. LI calculated from trunk acceleration was found to be useful for evaluation of asymmetry of trunk movement during walking.
Relation between LI and body function in patients with stroke
LI of stroke patients was revealed a negatively correlation with BBS (Berg et al., 1992; Berg et al., 1995) for standing balance. Lee et al showed how training of trunk function improves gait parameters, e.g., cadence and stride length (Lee et al., 2016). The present study likewise reflected a correlation between stability of standing balance and symmetry of trunk movement. Kavanagh et al. reported that an accelerometer can detect the complex motion of rotation, not only in the ML direction, but also of the vertebral column (Kavanagh & Menz, 2008). Osaka et al. reported that the trunk acceleration index of the ML direction is lacking in reliability as an index of the regularity and symmetry of walking, and that trunk acceleration in the VT direction reflects the action of the body most accurately (Osaka et al., 2013). LI evaluates the change of acceleration on the frontal plane and includes not only ML acceleration but also VT acceleration (Helen & Montgomery, 2008). For this reason it is possible that LI could become a new method of evaluating symmetry and balance during gait.
There are some limitations in this study. First, the change of LI over time in stroke patients was not investigated. Such investigations are important to pursue before LI can be used in clinical practice. Second, while good intra-rater reliability was shown in this study, inter-rater reliability will also need to be examined.
Conclusion
LI measured by a tri-axial accelerometer at the level of the L3 spinous process in stroke patients showed high intra-rater reliability and absolute reliability. The LI measured at comfortable gait speed in stroke patients was larger than the LI of healthy subjects, and showed a negative correlation with BBS. Thus, it was clear that LI during gait was effective at evaluating gait symmetry and balance. Overall, LF and LI were indicated to be useful in evaluating gait in patients with stroke.
Conflict of interest
With regards to the theme of this manuscript, there are no companies in COI relationship that should be disclosed.