
Abstract
OBJECTIVE:
The purpose of this study was to evaluate the effect of treadmill training with body weight support on gait kinematics parameters in patients with PD using DBS.
DESIGN:
Twelve patients completed the protocols (age: 60.9±10.6 years; disease duration: 20±7 years; and time since DBS surgery: 20±4 months). The same set of patients underwent two trainings protocols and four gait analyses (before and after each training). They received eight weeks of treadmill training without body weight support (16 sessions) in conjunction with physiotherapy program followed by six weeks of wash out period, followed by eight weeks of body-weight-supported treadmill training in conjunction with a same physiotherapy program. The Gait Kinematic Analysis involved eight infrared cameras that detected 19 reflective spherical markers attached in limb lower of patients. Statistical analysis used the Wilcoxon test (p≤0.05).
RESULTS:
Both the training no showed significant differences in linear variables. As the angular variables, only training with support showed significant increase of ranges of motion: pelvis tilt, obliquity and rotation amplitude; hip adduction-abduction and rotation amplitude; percentage of peak flexion in swing phase; foot progression amplitude.
CONCLUSION:
The body weight supported treadmill training may promote increase of mobility of lower limbs during gait and it could be a targeted intervention for PD patients treated with DBS.
Introduction
Gait disturbance is one of the hallmark features of Parkinson’s disease (PD), which significantly disrupts the individual’s ability to maintain mobility, independence, and overall health related to quality of life (Peppe et al., 2007).
Impairments in Parkinson gait usually include difficulty in walking and stopping, reducing stride length and speed, and increasing double limb support time (Fisher et al., 2008). Moreover, studies observed decreased range of motion (ROM) of the hip, knee, ankle, trunk and upper limbs (Sofuwa et al., 2005; Svehlik et al., 2009; Roiz et al., 2010).
With the advance of the disease, there is decreased efficacy of medication treatment and increase of gait impaired (Braak et al., 2003). At this stage, subthalamic nucleus deep brain stimulation (DBS) has been indicated and studies show that after surgery occurs increase in gait velocity and stride length (Johnsen et al., 2009; Potter-Nerger et al., 2013), as well as lower limbs articulations ROM (Ferrarin et al., 2005; Lubik et al., 2006; Stolze et al., 2001). Then, it is essential that this new condition of mobility’s improvement after subthalamic nucleus DBS could be associated with specific motor rehabilitation to maintain and improve the acquired functional gains (Botzel et al., 2010; Vercruysse et al., 2014), once the surgery does not stop the degenerative effects of the disease.
The use of treadmill training has long been a therapy most notable to the gait of patients with PD and leading the patients greater improvements in gait parameters, when compared to those without treadmill gait therapy (Miyai et al., 2000; Miyai et al., 2002), because it is more specific for gait improvement. The treadmill training promotes continuous sensory stimulation; external sensory cues; activation of central pattern gait generator circuits, visual feedback and motor learning (Bello et al., 2012), more than non-specific rehabilitation protocols.
The gait treadmill training in DP has been studied with body weight support (BWS) (Fisher et al., 2008; Miyai et al., 2000) or without support (Pohl et al., 2003). Compared to unsupported, the training with BWS provides more safety and facilitates the movement of the lower limbs, as well as lower cardiorespiratory demand (Miyai et al., 2000; Miyai et al., 2002). The characteristics described above are associated with the greater ROM of the lower limbs joints, acquired after the DBS implantation in PD patients. The association of all these factors could be helpful to maintain the clinical gait improvement acquired after surgery.
There are very few studies that have analyzed the gait patterns in PD patients using DBS after such rehabilitation programs (Johnsen et al., 2009; Ferrarin et al., 2005; McNeely et al., 2011; Sofuwa et al., 2005) and which do not address treadmill therapy with body weight support (Johnsen et al., 2009; Sofuwa et al., 2005). Moreover, assessments performed do not use kinematics, that have accuracy and specificity to evaluate the series of complex movements of the locomotion cycle (Potter-Nerger et al., 2013). Only one study observed the effect of Lokomat system training with kinematic assessment, but did not compare with the unsupported (Nardo et al., 2014).
The purpose of this study was to evaluate the effect of treadmill training with body weight support on gait kinematics parameters in patients with PD using DBS.
Methods
Study design
This study is a cross over clinical trial and was registered on http://www.ensaiosclinicos.gov.br (Número do UTN: U1111-1130-6667). The study was approved by ethics committee of Clinical Hospital, School of Medicine, University of São Paulo under number 0105/10, and all the participants have signed statements of informed consent.
Participants
The participants were recruited from the Departament of Neurology of Hospital das Clínicas (Medical School University São Paulo, Brazil). Patients underwent bilateral subthalamic nucleus deep brain stimulation (DBS) between January, 2008 and December, 2011, were eligible for inclusion after postsurgical monitoring. Although a non-probabilistic or convenience sample, a sample calculation was performed through a study by Nardo et al. (2014), which evaluated kinematic parameters of individuals with deep brain stimulation after gait training. The formula used based on Miot (2011) is below and the result was 9.
N - sample size; Zα/2 - critical value for the desired degree of confidence, 1.96 (95%); Δ - population standard deviation of the variable; E - standard error, 5%; N - population size (finite).
The inclusion criteria were: adults (over the age of 18) diagnosed with PD, who has implanted bilateral DBS at least 12 months prior to assessment postoperative monitoring, classified between levels 2 and 3 on the Hoehn–Yahr modified scale; a Mini Mental State Examination (MMSE) score ≥25 (5); stability of medications dose; patients with the DBS parameters: without adequate response to treatment with medication or who have complications related to prolonged use of levodopa; with the possibility of to do local or general anestesia; intellectually able to understand and sign the consent form and normal hematology, coagulation and metabolic exams. Also, the patient had to show an ability to walk at least 10 meters without assistance; no history of treadmill training in the previous six months; no concomitant physiotherapy interventions during research period and the absence of other existing neurological disorders, orthopedic surgery and visual and auditory deficits.
Patients were excluded if they were not able to perform the evaluations or discontinuity of treatment. Other exclusion criteria were: patients with anatomical abnormalities that preclude access to the implant electrodes (cranial or intracranial tumors, cysts); patients with uncontrolled infection or other uncontrolled pre-existing medical conditions (eg., decompensated diabetes, hypertension, symptomatic heart disease); history primary or secondary myocardial ischemia, congestive heart failure, cardiac arrhythmia; concurrent treatment with other experimental drugs; pregnant or breastfeeding and sociological, geographical or psychological conditions, that make impossible the post-operative medical care.
From 33 patients who matched inclusion criteria, only 17 were able to participate. Among these patients, five were excluded (2 changed DBS devices and 3 for excessive absence).
Interventions
The same set of patients underwent two trainings protocols and four gait analysis. Initially, the patients underwent the first gait kinematic analysis. There after received eight weeks of treadmill training without body weight support (TT) in conjunction with physiotherapy program, followed by the second gait kinematic analysis. So, the patients were referred to six weeks of wash out period. Thereafter, they underwent the third gait kinematic analysis and then completed eight week of body-weight-supported treadmill training (BWSTT) also concurrently with the same physiotherapy program, followed by the fourth gait analysis. The interventions was performed in Laboratory for the Study of Movement, Department of Orthopedics and Traumatology, School of Medicine, University of São Paulo, São Paulo, Brazil.
Both types of interventions were developed in 90 minutes (treadmill training, 30 minutes and physiotherapy program, 60 minutes), twice a week (total of 16 sessions) and were conducted individually and applied by two trained physiotherapists. The physiotherapy program was the same to the two interventions and was performed before of treadmill training.
During wash out period, the patients were instructed to not participate in any type of physical therapy, just to continue their daily living activities. Each week, the patients received calls from researchers and were asked about their physical condition. They remained well and did not participate in any therapy.
Physiotherapy program
The physiotherapy program included: flexibility, muscular resistance and balance exercises.
The part of flexibility was performed by two sets of 20 seconds of trunk, upper and lower limb stretching (Cakit et al., 2007). The stretching exercises were four recommended by the Parkinson Society Canadian: Rotation of trunk; trunk lateral tilt; gastrocnemius stretching; shoulder flexion.
The stage of muscular resistance was performed for lower limbs (quadriceps, hamstrings, gastrocnemius), upper limbs and scapular girdle (biceps, triceps, rhomboids, trapezius) and trunk (flexors and extensors) (Gobbi et al., 2009). For each exercise, three sets of 15 repetitions will be performed. The exercises were: training for biceps brachial and hip adductors; training for rhomboid and hip abductors; training for hamstrings, gluteus maximus and médium; mini-squatting; Step down; Sit to stand; training for dorsiflexors.
The balance was performed through exercises to stimulate hip, knee, ankle and trunk strategies (Ashburn et al., 2007). The patient performed two sets of 3 balance exercise (bipodal, tandem and unipodal stance; 1 minute each). The evolution criteria: open eyes and after closed in stable support; open eyes and after closed in unstable support. The progression will be performed when the patient will execut the exercise for 1 minute without difficulty. The orientation in all exercises will be to keep the orthoticism and of body alignment.
Treadmill training
Both trainings had duration of 30 minutes and speed initiated at 0.5 km/h, that increased by increments of 0.5 km/h as tolerated by each patient. At the end of each training the values of effort in metabolic equivalents (METs), distance and speeds were recorded for each individual. The maximum speed reached was 5 km/h, since patients were encouraged to maintain the usual speed from day to day. During the training, patients were carefully monitored for fatigue. When the patient complained of fatigue or any symptom related to overexertion (e.g., shortness of breath or large variation of effort METs) walking speed was gradually reduced to a comfortable pace (by decreases of 0.5 km/h).
The difference inter trainings, was that the BWSTT required the use of a body belt with straps to allow body suspension. At the beginning, BWSTT was administered with 30% of body weight support, at the sixth session, was reduced to 20% and at the 11th to 10%.
Outcomes measures
The outcomes were gait kinematics parameters: spatiotemporal (gait velocity, cadence, stride length, step length, and single stance time) and angular, which included pelvis (obliquity and rotation and maximal pelvic tilt), hip (flexion/extension, abduction/adduction, and rotation) and knee (flexion and extension) amplitude, swing phase percentage of occurrence of the maximal amplitude of knee flexion, the amplitude (maximal) of dorsal flexion and foot progression in stance. All the variables were examined in dominants and non-dominants members.
Gait kinematic analysis
The gait kinematic analysis was performed by the same experienced examiner in four times. He was blinded, did not participate of intervention and recruitment.
Kinematic analysis is a reliable and commonly used assessment method to quantify lower limb movements (Ferrarin et al., 2005). The analysis involves eight infrared cameras SMARTD BTS system (Milan, Italy) at 100 Hz with fourth order Butterworth filter (cut-off frequency 8 Hz). This captured the movements of the reflective markers that were placed on specific anatomical points of the patient’s skin, based on Vicon® Plug in Gait model (Ferrarin et al., 2005).
All of the cameras will be connected to a computer dedicated to treatment of the video signal, which has different functions: timing circuit/control; coordinate generating circuit and interface circuit of the cameras. Once stored in the video memory, the data will be transferred to a second general purpose computer. Vicon-Nexus® software will be used to process and reconstruct 3D images of the markers through a biomechanical model and a number of mathematical algorithms.
Static calibration of the system will first be performed to determine the laboratory reference coordinates (X, Y and Z). Subsequently, dynamic calibration will be carried out scanning the volume of interest with a metal rod in the shape of a “T” containing five markers. All of the participants will wear shorts to enable the placement and reading of the markers. Their skin will be cleaned with cotton and 70% alcohol to improve the fixation of the markers. 19 retro-reflective double-sided spherical markers (14 mm diameter) will be fixed (3M®) to specific anatomical points, which will serve as a reference for the motion analysis capture system. The markers will be placed in the following locations: side of thigh; lateral face of patella; lateral femoral epicondyle; side of shin; lateral malleolus; foot’s middle third between the 2nd and 3rd metatarsals and the calcaneus.
This set of markers is based on the Helen Hays model that will be used to estimate the position of the articular centers, as well as to calculate the three-dimensional kinematics of the joints of the pelvis, hip, knee and ankle (Davis et al., 1991; Kadaba et al., 1990).
The walk on a track measuring 1.5 m×4.0 m was selected for the analysis. Patients received instructions to walk barefoot 10 times on a track measuring 1.5 m×4.0 m at a self-selected speed.
After the capture of the coordinates of the markers, they were named and saved in C3D format. In order to reconstruct the three-dimensional biomechanical model, the coordinates of the markers fixed to pelvis, thigh, leg and foot were imported and processed in Vicon Nexus® software. During processing, each analysis 6 gait cycle were extracted and an average was made.
Statistical analysis
The data were stored and analyzed in the SPSS (v 20.0) and they were described by medians, means, and standard deviation. The Shapiro-Wilk test was used to determine whether the continuous variables presented a normal distribution.
The paired Student’s T-tests and Wilcoxon signed-rank tests were used for the comparison of angular and spatiotemporal gait parameters. The following comparisions were made: (1) pre versus post TT evaluation; (2) pre versus post BWST evaluation. Comparisons between evaluation pre-treadmill training without body weight support and evaluation pre-treadmill training with body weight support were performed for all variables in order to ensure that the wash out was effective. Lastly, no significant differences were found for any variables. Statistical significance was set at p≤0.05.
The calculation of Effect Size (ES) was performed by Cohen’s formula (average post-test (–) average pre-test/standard deviation pre-test).
Results
The main characteristics of the enrolled patients have been resumed in Table 1. Twelve of them finished the protocol: six males and six females (age: 60.9±10.6 years; MMSE: 27.2±1.2; disease duration: 20±7 years; and time since DBS surgery: 20±4 months). According to the Hoehn and Yahr Classification, one patient was classified as 3, seven as 2.5 and three as 2.
Patients’ clinical characteristics
Patients’ clinical characteristics
SD, Standard Deviation; M, Male; F, Female; H&Y, Hoehn and Yahr stage; DBS, Deep brain stimulation.
The Fig. 1 shows the enrollment and retention of study participants.
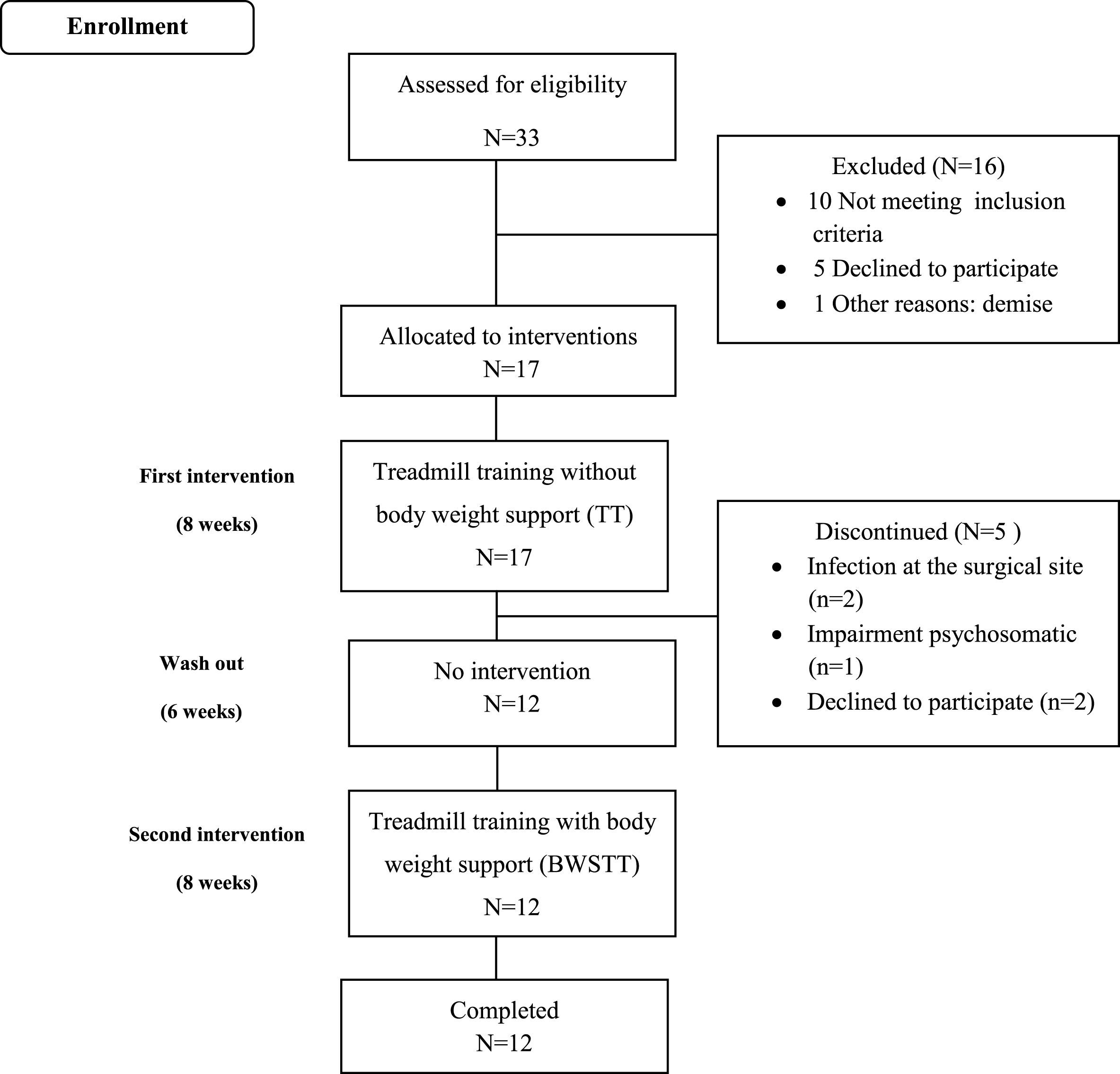
Enrollment and retention of study participants.
No significant differences were found to spatiotemporal gait parameters after both trainings: TT and BWSTT (Table 2).
Spatiotemporal gait parameters before and after the treadmill training without and with body weight support in Parkinson’s disease patients using Deep Brain Stimulation
Spatiotemporal gait parameters before and after the treadmill training without and with body weight support in Parkinson’s disease patients using Deep Brain Stimulation
Wilcoxon Test.; Mean (Standard Deviation); TT, Treadmill training without body weight support; DL, Dominant limb; NDL, Non-Dominant limb; ES, Effects Size.
Although no significant differences were found from pre and post-intervention for TT, expressive improvements were observed for the next variables in response to the BWSTT intervention: pelvis’ range of motion (obliquity, rotation and tilt); hip’s range of amplitude (abduction-adduction and rotation); % knee maximal flexion on Swing phase; and foot progression range of motion (Tables 3 and 4).
Pevis and Hip Angulars gait parameters before and after the treadmill training without and with body weight support in Parkinson’s disease patients using Deep Brain Stimulation
Pevis and Hip Angulars gait parameters before and after the treadmill training without and with body weight support in Parkinson’s disease patients using Deep Brain Stimulation
Test. Wilcoxon *p < 0.05; Mean (Standard Deviation); TT, Treadmill training without body weight support; DL, Dominant limb; NDL, Non-Dominant limb; Max, Maximum; Ext., Extension; Addu., Adduction; ES, Effects Size.
Knee, Ankle and Foot Angulars gait parameters before and after the treadmill training without and with body weight support in Parkinson’s disease patients using Deep Brain Stimulation
Test. Wilcoxon *p < 0.05; Mean (Standard Deviation); TT, Treadmill training without body weight support; DL, Dominant limb; NDL, Non-Dominant limb; Max, Maximum; Ext., Extension; Addu., Adduction; ES, Effects Size.
The main finding of this study were that after eight weeks of gait treadmill training with support, DP patients in use of DBS showed increase ranges of motion of pelvis; hip; knee and foot. On the other, the TT did not show significant differences to gait angular variables and both trainings did not show significant differences to gait spatiotemporal parameters.
Regarding the spatiotemporal variables (velocity, cadence, stride length, step length, and single stance time) there were not significant differences after both trainings. The spatiotemporal parameters are functional and contribute to the early detection of fall risk (Morris et al., 2005), however, they may be less sensitive to change in motor control training, especially this particular sample, when they had already improved gait pattern after DBS implantation.
DP patients who underwent treadmill training without (Bello et al., 2010; Harro et al., 2014; Nadeau et al., 2014) or with BWS (Fisher et al., 2008; Miyai et al., 2000) improved velocity, stride length and step length. However, they were PD patients without DBS and treadmill training comparison was made with other type of therapies. All the studies, but one (Fisher et al., 2008) did not use kinematics evalution, but functional clinical scales.
It is possible that the results of the linear variables are due to the following sample characteristics: “ON DBS” condition and medication. PD patients with bilateral DBS with (Johnsen et al., 2009; McNeely et al., 2011; Chastan et al., 2009) or without (St George et al., 2010) the use of dopaminergic drugs, have better spatial kinematic parameters than the stage “OFF DBS”. DBS promotes improvement in spatiotemporal parameters and in the feet’s spatial position progress, allowing the patients to perform steps much more similar to healthy adults, without PD (St George et al., 2010).
Significant differences were found for angular variables from pre and post-BWST intervention.
The pelvic obliquity (coronal plane) of dominant limb increased from 6.27° to 8.95°, even higher than the value expected from healthy adults (7°) (Saunders et al., 1953) and for individuals without PD paired by age to the current study, which values vary between 6° and 7° (6.7° (Johnsen et al., 2009) and 6.2° (Ferrarin et al., 2005)). The pelvic rotation (transverse plane) of dominant limb increased from 5.62° to 12.28°, also higher than the rotation performed by young adults (10°) (Cakit et al., 2007). However, results on health’s individual without PD show divergent values concerning pelvic rotation, which ranged between 4.2° to 10° (Svehlik et al., 2009; Roiz et al., 2010; Sofuwa et al., 2005; Morris et al., 2005). Morris et al. (1999) reported that the increase of pelvic movement in the coronal and transverse planes in PD is related to the reduced range of motion at lower limb joints. Then, as the rotation occurs at the moment in which the limb progresses in the sway phase, it could be observed that there is an avoidance of pelvis’s drop as well as an adjustment on the step size (Saunders, 1953).
Therefore, if there is an increase in the motion at coronal plane, the pelvis will have to augment its limits of rotation. Hence, this relation may have occurred as a strategy in order to help the limb to perform in sway phase. As it could be observed, the values may have reached higher levels when compared to those presented by the literature, since the use of body weight support has allowed more balance and safety. The pelvic tilt (sagittal plane) of non-dominant limb increased from 4° to 4.9°, higher than the values accomplished by a healthy adult which is 4° (Perry, 2005). The enlargement of pelvic tilt has been associated to the increase of pelvic obliquity (Wolf et al., 2014).
The range of the hip abduction-adduction of dominant limb increased from 8.11° to 11.98°, higher than the values achieved by healthy adults which is 10° (Saunders, 1953). Pelvis’ rotation expansion may have favored the action of hip adductors that replaced the action of hip flexors (PD characteristic) and increased the hip range of motion at coronal plane. This muscular action of adductors to perform hip flexion is accompanied by internal rotation (Perry, 2005), that, also, can explain the augment of the hip movement at the frontal plane, in the non-dominant limb (10.8° to 18.03°).
Another kinematic parameter that has changed after BWST was percentage of gait cycle of maximum knee flexion during swing phase. The percentage of gait cycle increased from 36.85% to 64.20% (non-dominant limb) and 38.59% to 64.27% (dominant limb), approaching the physiological values, which is 71.7% for healthy adults (Perry, 2005). This enlargement represents an evolution because it shows: greater postural control during the swing phase, better preparation of the limb for shock absorption in the heel strike and more stability and support in the stance phase.
Regarding the amplitude of foot progression, the increase was from 2.5° to 6.3°. These initial values may indicate the difficulty concerning heel’s elevation in the pre-swing phases, fact that happens in Parkinson’s disease (Nieuwboer et al., 2007). After training. although they have not reached physiological values, there was meaningful improvement in heel’s elevation that may have raised the mobility of middle tarsus joints and forefoot in the pre-swing phase.
The increase of the pelvis, hip, knee and foot mobility could improve the gait determinant and energy expenditure, even if the spatiotemporal parameters did not change. Probably the BWST was more effective to change the gait angular biomechanic, because the patient can keep the stimulus any longer, with less fatigue. This affirmation is consistent with the findings of 2014 study (Nardo et al., 2014), similar to actual, that assessed nine DP patients with DBS in relation to gait kinematic parameters, after Lokomat robotic gait training (five weeks, 45 minutes daily). The sagittal ankle ROM increased and the improvement is related to the motor control continuous stimulus.
The supported training may have contributed to greater perception of safety, more comfort and easiness to perform the movement of the lower limbs (Lubik et al., 2006; Stolze et al., 2001; Ferrarin et al., 2005). The training without body weight support requires more effort and cardiorespiratory demand (Toole et al., 2005), and probably the main effects of this intervention are physical performance gains and not in the gait angular parameters.
The present study is the first to report the effectiveness of two treadmill training (with and without body weight support) on gait kinematics parameters in patients with PD using DBS. Studies have been conducted with the use of BWST in patients with PD, but most of them without DBS use. Fisher et al. (2008) compared three groups: BWST, physical therapy (range of motion, balance, strength exercise, gait and daily activities training) and therapeutic education (classes about quality of life). BWST group increased hip and ankle range of motion. Although the sample had lower Hoehn & Yahr index and used 10% of body weight support without progression, the result was similar to this present study. The support training can help ankle and hip motion.
Other studies also showed improvement after BWST in PD patients, but used only gait clinical scales. Miyai et al. (2000) compared BWST (20%) with conventional physiotherapy program and the main outcome was the Unified Parkinson’s Disease Rating Scale (UPDRS), speed and number of steps in a 10-meter walk test. Toole et al. (2005) evaluated six weeks’ effects of treadmill training in 23 patients with PD, divided in three groups: two of them did treadmill training with body weight support (25% and 5%) and the third trained unsupported. The three groups improved in the in UPDRS and Berg scale evaluation.
In this study, the BWST may have increased the neurophysiological effects of DBS through dopaminergic and non-dopaminergic pathways and promoted gait improvements. Consistent with this view, Tassoreli et al. (2009) suggested that the effects of a motor rehabilitation program could be associated with the effects of DBS in the neuroplasticity stimulation. DBS increases the motor cortex excitability and can change the neural pattern, normalizing the synchronization between the structures of basal ganglia and this effect could restore the ability of the thalamocortical cells10. The BWST improve postural reflexes (Toole et al., 2005) and could help in normalization of corticomotor excitability mainly in supplementary motor area (Fisher et al., 2008).
The main limitation of this study is sample size. It is a convenience sample (patients on DBS and walkers, coming from a public hospital and mostly low-income), where socio-economic conditions and the place of residence had great impact on the frequency of the patient in the training program. Many of them were not included because they lived in other cities.
However, no patient was excluded due to adverse effect of the training program. The methodological model proposed was “fixed crossover”, where it ensured that there would be not differences between pre - intervention 1 and 3. Although the limitations should be considered, the result is intriguing and opens new perspectives in the area. The use of three-dimensional gait analysis is scarce in studies with PD, but is considered as a method “gold standard” to improve understanding of the biomechanics of the joint movements, providing reproducible and reliable data (Roiz et al., 2010).
The present study did not use high-end robotic technology for gait training, but showed that a simple BWS treadmill system could be useful to promote functional gains in PD patients. So, the expressive clinical application of study is the use of this therapy (safe and cheap) in the rehabilitation of Parkinson patients with DBS. The BWST can contribute to the neurophysiological effects of DBS through dopaminergic and non-dopaminergic pathways and thus promote gait improvement through increased mobility of pelvis; Hip; Knee and foot joints.
This information can guide the therapeutic planning to the rehabilitation Parkinson patients, which may involve a period of training with support and other withou support. The gait training with support would be done first because have lower cardiorespiratory demand and may promote greater mobility and body awareness of upright posture. In addition, the study observe the importance of association of gait training with an exercise program of flexibility, muscular endurance and balance, since the treatment of Parkinson’s disease needs to involve all these goals.
The association of BWS with virtual reality scenarios can be even more efficient in clinical improvement, functional and kinematic. More studies on rehabilitation programs (type, intensity, time) in PD patients in use of DBS are needed. The association of biomechanical evaluation with neuroimaging and brain electrical activity performed during motor activities, can contribute to increase the understanding of the mechanisms involved and how to increase the efficiency of rehabilitation programs.
In conclusion, the body weight supported treadmill training may promote increase of mobility of lower limbs during gait and it could be a targeted intervention for PD patients treated with DBS.
Conflict of interest
All authors report no biomedical financial interests or potential conflicts of interest.