
Abstract
BACKGROUND:
Autonomic disturbances are a common phenomenon in patients’ post-stroke, characterized by hypo function of the para-sympathetic and/or overactive sympathetic system. The impact of autonomic disturbances on physical therapy tasks during the rehabilitation period has not yet been assessed.
OBJECTIVE:
To describe the response of the cardiac autonomic nervous system during different tasks, among patients and age-matched healthy controls.
METHODS:
Nineteen patients in the subacute phase post first-ever ischemic stroke, and 16 controls. The Polar advanced heart rate monitor (RS800CX) was used to record RR intervals at rest, during paced breathing exercise, while performing different types of muscle contractions, and during single and dual task conditions.
RESULTS:
RR intervals and heart-rate variability (HRV) parameters were significantly lower among patients post stroke, both at rest and during most of the activities tested. Among the control group a significant autonomic adaptation was seen in the form of reduced RR intervals and HRV during muscle contraction and a significant increase in these parameters during slow breathing, no significant changes were observed among patients post stroke.
CONCLUSION:
Patients post-stroke experience hyper sympathetic function at rest and less adaptive cardiac autonomic control during different activities, which all may have an impact on rehabilitation outcomes.
Introduction
Stroke rehabilitation focuses mainly on an effort to improve patients’ impaired motor, cognitive an linguistic abilities (Carr & Shepherd, 2003). Despite the frequency of impairments in functioning of the autonomic nervous system (Korpelainen, Sotaniemi, & Myllyla, 1999), especially cardiovascular signs like heart rate and blood pressure dysregulation (Tokgozoglu et al., 1999), this component of the symptom complex manifested post stroke seldom receives a proper consideration in the form of systematic assessment and treatment.
Soon after stroke onset and during the subacute period, an association was found between autonomic and motor impairments and functional disability (Raphaely Beer & Katz-Leurer, 2014). The impact of autonomic nervous system impairments on the rehabilitation process is seldom assessed, despite the inherent role of this system in exercise physiology which is a central component of stroke rehabilitation programs. For example, muscle strength training, using static and dynamic exercises, is employed in stroke rehabilitation in order to prevent muscle atrophy secondary to reduced activity (Eng, 2004). It is well known that for such training to succeed in muscle strengthening, an accurate blood supply regulation is required (Iellamo et al., 1999). Cognitive therapy, another major component of stroke rehabilitation programs aimed to enhance functional cognition. A large body of research has shown the connection between cognitive functioning and the cardiovascular system through autonomic vagal control (Thayer & Lane, 2009).
Diagnostic evaluation of autonomic nervous system functioning is a multi-faceted process, including monitoring cardiovascular responses to position changes, to static muscle contraction – e.g., during forced grip (Ewing, Borsey, Bellavere, & Clarke, 1981), to breathing tests (Ewing et al., 1981) and other tasks being part of the daily routine of stroke rehabilitation programs. The current study aims are to describe the response of the cardiac autonomic nervous system to different daily demands during active rehabilitation of patients with first-ever ischemic stroke. Our assumption was that the response of the cardiac autonomic system to different demands will be less flexible and adaptive compared to the typical response of age matched healthy controls.
Methods
Nineteen patients post first-ever ischemic stroke, 11 with right- and 8 with left-hemisphere stroke, were recruited from the Neurology Department at Sorasky Medical Center Tel Aviv and the Department of Neurological Rehabilitation at the Loewenstein Rehabilitation Center, Raanana, Israel. Sixteen age-matched healthy individuals served as the control group. Inclusion criteria were: age range between 40–80 years, negative neurological medical history prior to the stroke event, negative history of cardiac disease, stable clinical and metabolic state at the time of testing, and lack of major hearing or vision impairment, dementia or major depression. All the participants provided a written informed consent. The study was approved by the Institutional Review Board for experiments involving human subjects (Helsinki Committee) of the Sorasky and the Loewenstein hospitals.
Tools
Heart rate was monitored by the Polar Advanced Heart Rate Monitor (RS800CX) validated for this purpose (Gamelin, Berthoin, & Bosquet, 2006). An elastic electrode transmitter belt (Polar sensor) was placed on the lower chest. The electrodes detect the voltage differential on the skin during every heart beat and send a continuous wireless signal to the Polar RS800CX receiver unit which is then transferred via Polar-specific software (Polar® ProTrainer 5 software) to a computer. The data were then exported as a text file to the HRV analysis software (Kubios heart rate variability software version 2.0; Biosignal Analysis and Medical Imaging Group, Department of Physics, University of Kuopio, Kuopio, Finland) for analysis. The standard deviation of normal R– R intervals (SDNN) and the root-mean-square difference of successive normal R– R intervals (RMSSD) were used as parameters of the total variance and the vagal control within the time domain respectively (Allen, Chambers, & Towers, 2007). The Montreal Cognitive Assessment Scale (MoCA) was used as a screening test for cognitive function including sub-tests that assessed executive functions and psychomotor speed (Nasreddine et al., 2005). The Barthel index was used to assess patients basic daily functional ability (Mahoney, 1965).
Protocol
The test was conducted in a sitting position with the polar belt attached to the patient. And after a ten-minute rest period, the MoCA evaluation was given. The sequence of testing conditions, taken from the daily rehabilitation repertoire, included static and dynamic muscle contraction, single and dual task conditions, and paced breathing exercise. Testing was performed in the following order: Static muscle contraction (grip test): The participants were requested to sustain a handgrip at 1/3 of maximum voluntary contraction pressure for 2 minutes using the dynamometer scale in front of them. Paced breathing: The participants were asked to breathe at a rate of 6 breaths per minute for two minutes. Single cognitive task (serial three subtraction task): The participants were asked to sequentially subtract “3” starting from a three-digit number for one minute, the number of subtractions and number of errors were recorded. Active motor task: While sitting in a chair, the participants were asked to cycle at a comfortable pace for two continuous minutes. Dual task: The participants were asked to perform the serial three subtraction task while cycling at a comfortable pace. The cycling was performed for two minutes and the serial three subtraction task was added during the second minute.
Between each pair of tests, a three-minute rest period was given.
Statistical analysis
Statistical analyses were performed with SPSS software (Version 20.0 for Windows; SPSS Inc., Chicago, USA). Statistical significance was set at p < 0.05. The Kolmogorov-Smirnov test was performed for all outcome measures. As the data distribution fulfilled the assumption of normality, parametric statistics were used. Baseline differences were assessed by t-test. The differences between rest and each testing condition (delta) were computed and the differences between groups in each delta were assessed by t-tests.
Results
Participants were between 42 and 76 years of age, with no significant difference in age range between groups. The mean MoCA score of the patients group was significantly lower compared to that of age-matched healthy control subjects (Table 1).
Descriptive characteristics by groups
Descriptive characteristics by groups
Group mean and range [min-max] values. P-value based on chi square test and independent t-test; MoCA = The Montreal Cognitive Assessment Scale.
At rest, mean RR and SDNN values were significantly lower among patients post- stroke compared to age-matched healthy subjects (mean difference of 119 ms and 15 ms, respectively) (Table 2). The RMSSD value was lower among patients post-stroke, but the difference did not reach significance (5.8 ms, p = 0.08).
HRV parameters at rest in stroke patients and age-matched controls
Group mean (±SD) values in milliseconds. P-value based on independent t-test. Mean RR = Mean of the time interval in seconds between two nearby R waves on the ECG. SDNN = Standard deviation of the RR intervals. RMSSD = Root mean square of differences between adjacent RR intervals.
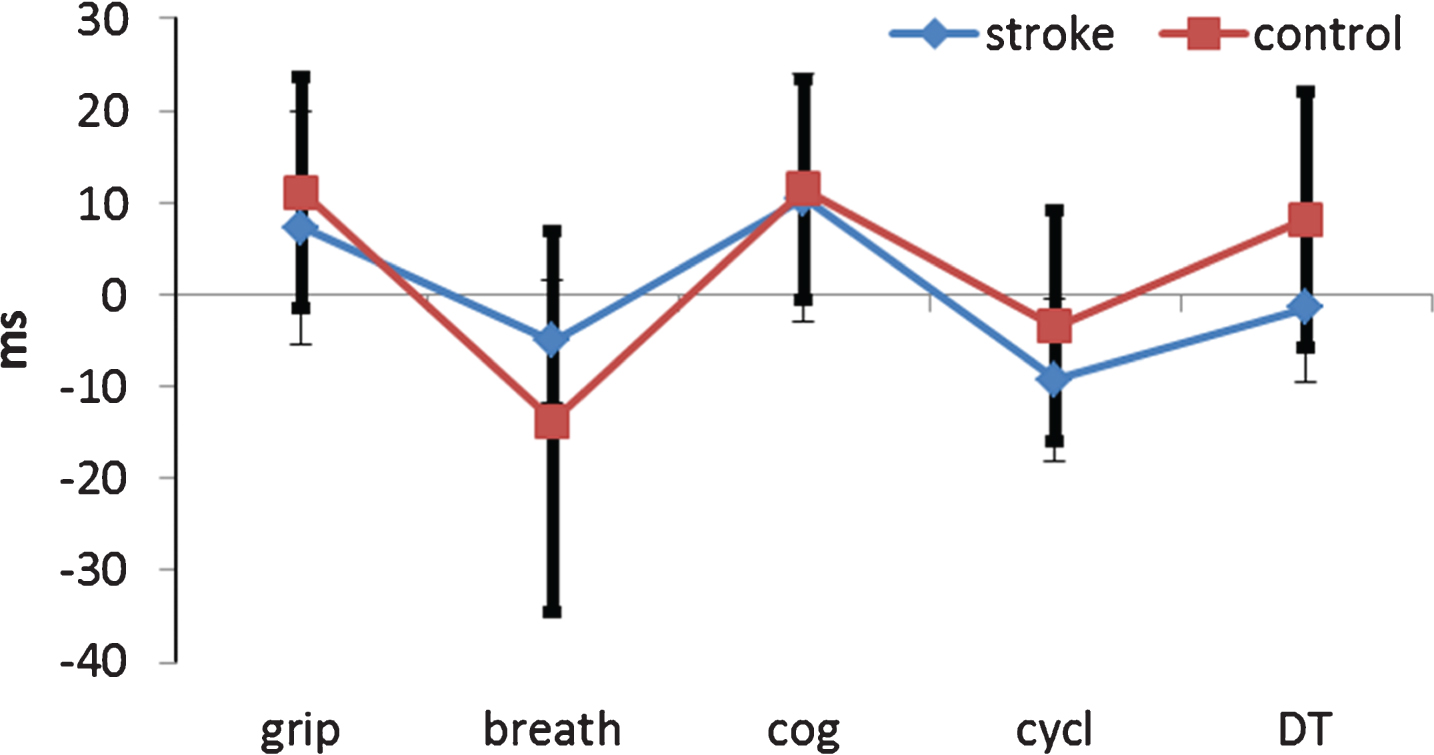
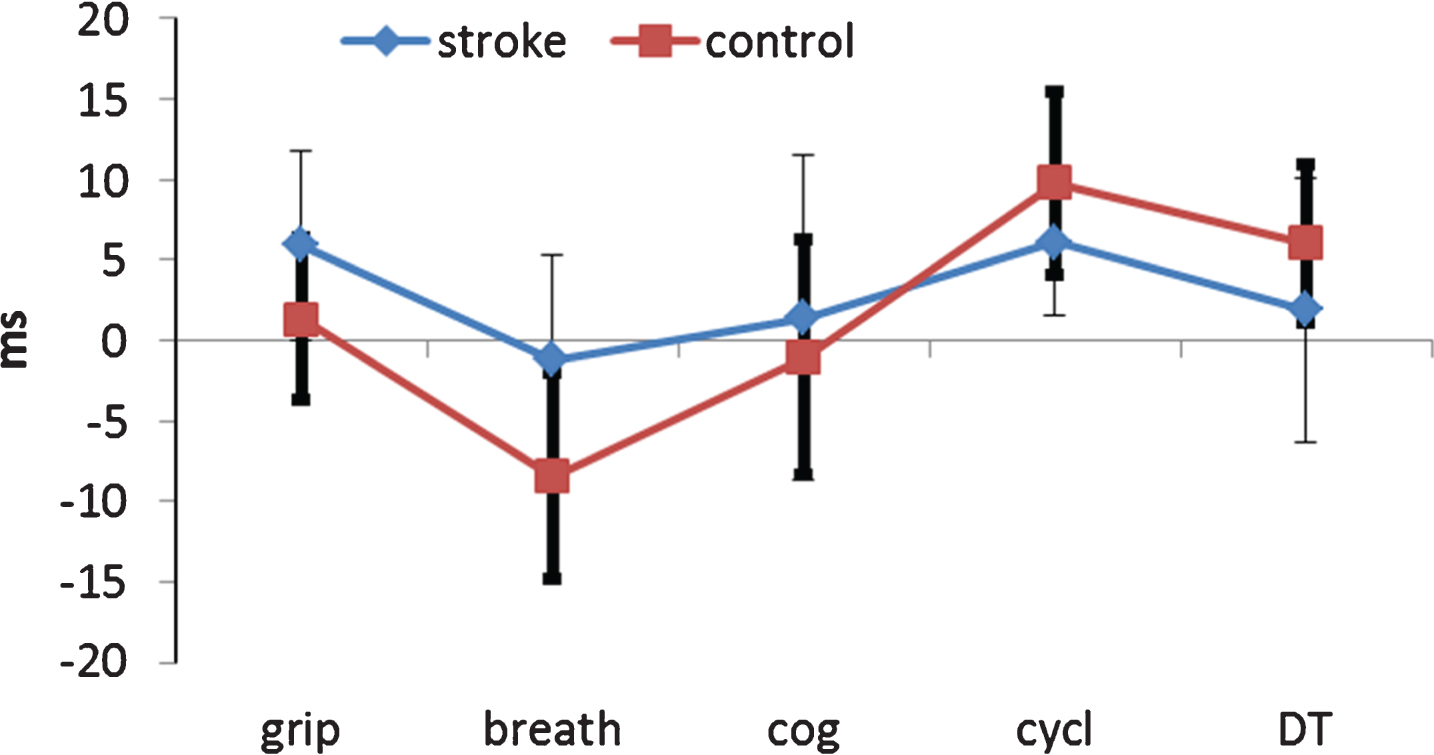
Figures 1–3 present the differences in RR, SDNN and RMSSD values between rest and each testing condition, reflecting the response of the autonomic cardiac nervous system to each task. The zero line represents no response and the error bars represent a 95% confidence interval around the mean difference. Differences from rest value in the RR interval are shown in Fig. 1. As can be seen, the control subjects exhibited significant responses in each testing condition, except for paced breathing, reflected in the form of reduced RR interval. In contrast, the, patients’ post-stroke exhibited a significant change from baseline only during paced breathing. Assessment of the difference between the two groups in delta values (the magnitude of change in a given testing condition relative to rest) using t-test, revealed significant differences during the cycling task. While the healthy controls reduced their RR by a mean of 179 ms, the average reduction among the patients post-stroke was by only 40 ms. Figure 2 presents the SDNN change from baseline. Although a trend towards a larger effect was noted among the control group, no significant differences from baseline values and no significant differences between groups was noted. Figure 3 presents the RMSSD change from baseline. While the controls exhibited a significant response in the breathing exercise, in cycling, and in the dual task conditions, patients post-stroke showed no significant response (change from baseline) in any of these conditions. Assessing differences in delta values between groups by t-test revealed no significant differences.

Delta mean RR values of patients and healthy control groups, in each testing condition relative to rest. Conditions: grip, breathing, serial-3, cycling, and serial-3 while cycling (see methods section). Mean RR = Mean time interval between two nearby R waves on the ECG.
Delta SDNN values of patients and healthy control groups, in each testing condition relative to rest. Conditions: grip, breathing, serial-3, cycling, and serial-3 while cycling (see methods section). SDNN = Standard deviation of the RR intervals.
Delta RMSSD values of patients and healthy control groups, in each testing condition relative to rest. Conditions: grip, breathing, serial-3, cycling, and serial-3 while cycling (see methods section). RMSSD = Root mean square of differences between adjacent RR intervals.
The main findings of the current study are (a) the significant reduction in RR and SDNN parameters of autonomic nervous system functioning among patients post stroke compared to age-matched healthy controls, and (b) the lack of adaptive autonomic cardiac response among post-stroke patients (unlike healthy controls), when passing from rest to different testing conditions representing activities that are common in the daily rehabilitation practice.
The significant decrease in RR and SDNN (with marginal decrease in RMSSD) parameters of autonomic nervous system functioning at rest, among patients post stroke compared to age-matched healthy controls, points to a state of sympathetic hyperactivity in the subacute phase post stroke onset. This finding is in accord with previous research (De Raedt, De Vos, & De Keyser, 2014; Thayer, Hansen, Saus-Rose, & Johnsen, 2009). It means that in a stroke patient at this phase of the disease (the subacute phase, where usually rehabilitation is conducted), the cardiac autonomic nervous system maintains at rest a level of activity which generally is preserved to more physically or emotionally active conditions (de Bruyne et al., 1999; Lucini, Norbiato, Clerici, & Pagani, 2002).
An examination of the behavior of the healthy control subjects in the different testing conditions, reveals the extent to which various motor and cognitive tasks, simulating or sampling daily routines of the rehabilitation process, recruit the sympathetic nervous system, thus pointing to the inherent role of the autonomic nervous system in such rehabilitation routines. The behavior exhibited by the healthy control group in reaction to the different tasks is in line with previous empirical evidence (Hansen, Johnsen, Sollers III, Stenvik, & Thayer, 2004; Shields, 2009; Thayer et al., 2009; Weippert, Behrens, Rieger, Stoll, & Kreuzfeld, 2013).
The behavior exhibited by the patients post-stroke was in sharp contrast to the pattern of response exhibited by the control group. The patients failed to show the normal increment in sympathetic activity in response to any of the testing conditions, primarily due to their hyper sympathetic state at rest. Two earlier studies that tested patients’ response to exercise at the acute and sub-acute phases post-stroke support our findings. Raimundo et al. (2013) found that patients’ HR and time domain HRV values do not return to baseline for up to 30 minutes post exercise, and Katz-Leurer et al. (2007) did not find any adaptation of HR values after 8 weeks of aerobic exercise. The current study and these earlier studies point to a significant physiological disturbance in the capacity of the autonomic nervous system to respond adequately to demands imposed by routine rehabilitation practices exercised during the subacute phase post stroke (Katz-Leurer & Shochina, 2007; Katz-Leurer, Zohar, Boum, & Keren, 2014; Raimundo et al., 2013), such that only higher demands recruit the expected sympathetic response (Raphaely Beer, Bornstein, Soroker, & Katz-Leurer, 2016). A recently published literature review concluded that associations exist between competence of the cardiac autonomic control and motor performance among patients post stroke: patients with more severe autonomic impairment exhibit lower motor performance (Raphaely Beer & Katz-Leurer, 2014). Whether this association post stroke reflects comorbidity or causality remains to be defined. However, an emphasis on the use of physical therapy measures aimed to improve the functioning of autonomic cardiac control, is indicated by the above findings.
Limitations
To reduce the impact of possible confounding factors we chose to include in the study patients with first-ever stroke without a history of cardiac problems, which narrows the study’s external validity with respect to the entire stroke population. Given the relationship between ischemic heart disease and stroke, this criterion resulted in a significant reduction in the number of subjects for enrollment. However, the significant group effects shown in the current study, despite the small number of patients, strengthens our basic claim for a stroke-related disturbance in cardiac autonomic system functioning, affecting the capacity of patients post stroke to cope with routine demands to the rehabilitation process.
Conclusion
Patients post stroke experience sympathetic overflow. This is reflected in the inability of the system to reach equilibrium with the para sympathetic sub-system at rest and when performing various tasks. In clinical practice this situation may seriously affect stroke patients’ capacity to cope adequately with routine demands of the rehabilitation program. Further research is needed in order to assess the optimal ways to rehabilitate the impaired autonomic cardiac control.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This work was performed in partial fulfillment of the requirements for a Ph.D. degree of Noa Raphaely Beer, Sackler Faculty of Medicine, Tel Aviv University, Israel.