
Abstract
BACKGROUND:
Proprioception deficits are common post-stroke and may lead to impaired standing balance and restricted mobility.
OBJECTIVES:
To compare 1) mobility, balance, balance confidence (BC), independence in basic and instrumental activities of daily living (BADL and IADL) of individuals with and without mild proprioception deficits at the chronic stage post-stroke. In addition, 2) correlations between mobility, balance and BC to BADL and IADL will be assessed.
METHODS:
Sixty-four participants [mean(SD) age - 59.9(9.3), 61% men, 26.1(18.3) months post-stroke] underwent the Thumb Localization Test (TLT) to assess proprioception; 45 participants had intact proprioception and 19 participants had mild proprioception deficits. The Timed Up and Go Test (TUG) and the Functional Reach Test (FRT) assessed mobility and balance (respectively). Activities-specific Balance Confidence (ABC) scale rated BC. BADL and IADL was also assessed.
RESULTS:
Significant differences in mobility, balance and BC, BADL, IADL were found between participants with and without mild proprioception deficits. Correlations between mobility, balance, and BC to BADL and IADL, were significant (p < 0.05) for all 64 participants, but not within groups.
CONCLUSIONS:
Mild proprioception deficits seem to be a confounding factor for explaining daily living at the chronic stage post-stroke. Proprioception screening is recommended for clinical practice and future research.
Introduction
A large percentage of individuals following stroke experience proprioception deficits in addition to the motor deficits on the contralateral side to the brain damage (Carey, 1995; Connell, Lincoln & Radford, 2008; Dukelow et al., 2010; Smith, Akhtar & Garraway, 1983). Proprioception is the perception of the position of body parts in space, the perception of motion, and the perception of force generated by the body (Berthoz, 2000; Niessen, Veeger & Janssen, 2009; Ogard, 2011; Proske & Gandevia, 2012). Proprioception information derives from muscle spindles, Golgi tendon organs, joint and cutaneous receptors (Haerer, 1997; Lephart, Riemann & Fu, 2000; Riemann & Lephart, 2002a; Riemann & Lephart, 2002b). Therefore proprioception deficits and not only muscle weakness may lead to impaired standing balance (Nian, Cheung, Sullivan, Kent & Gu, 1999), difficultly in regaining the ability to walk independently (Reding & Potes, 1988) and predict overall poor functional outcome post-stroke (Berthoz, 2000; Gottlieb et al., 1997; Prescott, Garraway & Akhtar, 1982; Reding, 1990; Reding & Potes, 1988; Smith et al., 1983; Stern, McDowell, Miller & Robinson, 1973; Wade, Wood & Langton-Hewer, 1985).
Balance, which is the ability to maintain the body mass above the base of support, is known to be impaired following stroke (Nian et al., 1999). Since intact balance requires the complex integration of vestibular, proprioceptive and visual inputs (Means, 2013), proprioception deficits may lead to balance impairments. Reding and Potes (1988) reported significant differences in regaining the ability to walk and achieving independence in BADL of individuals with combined motor and proprioception deficits compared to individuals with motor deficits post-stroke.
However, balance is not the only factor, which affects mobility and daily function (Hellström, Nilsson & Fugl-Meyer, 2001). Balance confidence (BC) is also an important predictor of activity and participation post-stroke (Schmid et al., 2012) and a predictor of satisfaction with community reintegration in older adults with chronic stroke (Pang, Eng & Miller, 2007). BC at discharge from stroke rehabilitation predicted perceived physical function, mobility, and recovery 12 months later (Torkia, Best, Miller & Eng, 2016). BC (sometimes referred to as balance self-efficacy), is an individual’s judgment of his or her balance ability (Bandura, 1997). According to Bandura’s Social Cognitive Theory, a person’s perceived level of ability predicts their behavior more than their actual physical ability (Bandura, 1977). In other words, an individual’s confidence in performing tasks without losing balance or becoming unsteady may be more, or as important as their actual ability to maintain balance.
Whereas factors such as balance, motor and physical functioning, and perceived health status (Hellström et al., 2001; Hellstrom, Lindmark, Wahlberg & Fugl-Meyer, 2003; Pang et al., 2007; Salbach et al., 2006; Schmid et al., 2012; Torkia et al., 2016) are known to correlate with BC, it is unknown if these correlations exist in participants with proprioception deficits. As intact proprioception is critical for movement control, balance and daily functioning, (Berthoz, 2000; Smith et al., 1983) it is important to understand if mobility, balance and BC of individuals with mild proprioception deficits correlates with their daily function at the chronic stage post-stroke.
Therefore, this study aims to compare 1) mobility, balance and BC, independence in basic and instrumental activities of daily living (BADL and IADL) of individuals with and without mild proprioception deficits at the chronic stage post-stroke. In addition, 2) correlations between mobility, balance and BC to BADL and IADL will be assessed. This will allow for a better understanding of the underlying factors which can explain independence in daily living and the role of proprioception at the chronic stage.
Methods
A secondary analysis of data obtained from a cross-sectional study with a convenience sample of individuals with chronic stroke.
Population
Adults with chronic stroke who lived in the community were invited to participate in the study. Inclusion criteria were 1. sustained a stroke at least 6 months prior to the study, 2. able to walk at least 10-meters (with or without assistance), to increase the like-hood of independence in daily function, 3. without a significant cognitive deficit (score >21/30 points on The Mini Mental State Examination, (Folstein, Folstein & McHugh, 1975) a valid and reliable screening test for cognition post-stroke). Participants with other neurological conditions were excluded from the study.
Procedure
This study was approved by the Research Ethics Committee in the rehabilitation center and the University Ethics committee. Participants were recruited using discharge lists from a large rehabilitation center. They were contacted and screened by phone and if found eligible, were invited to the rehabilitation center for the assessment session. After signing the informed consent form, the participants underwent the clinical assessments. They received reimbursement for their travel expenses.
Tools
Proprioception was assessed using the Thumb Localization Test (TLT), (Berthoz, 2000; Prescott et al., 1982) which is a quick and easy clinical test for proprioception (Hillier, Immink & Thewlis, 2015). The participant’s affected arm is moved by the examiner to four different locations in space and the participant is requested to grasp their affected thumb with their less-affected hand while their eyes are closed. The scoring for each location is based on the estimated distance that the participant misses their affected thumb in space and discriminates between ‘precisely grasps the thumb’ (0-no deficits), ‘just misses to grasp the thumb and immediately corrects’ (1-mild deficits), ‘is able to find the arm and uses the arm to find the thumb’ (2-moderate deficits), or ‘cannot locate his/her thumb’ (3-severe proprioception deficit). The TLT scoring is according to the worst performance of the four trials. Proprioception deficits assessed by the TLT have been reported to be significant moderately correlated to the Finger Shift Test, (Ziegler, 1975) a common test to assess proprioception (r = 0.53— 0.71, p < 0.01) assessed on week 0, 2, 4 and 6 weeks following admission to rehabilitation (Rand, Gottlieb & Weiss, 2001). Despite this, the validity and reliability of the TLT, similar to other tests for proprioception have not been well established (Hillier et al., 2015).
Mobility was tested using the Timed Up and Go Test (TUG) (Podsiadlo & Richardson, 1991), which assesses the ability to perform sequential motor tasks relative to walking and turning by measuring the time required to get up from an armchair, walk 3 m and return to the chair. Balance was assessed using The Functional Reach Test (FRT) (Duncan, Weiner, Chandler & Studenski, 1990), which measures the distance between the length of the arm and a maximal forward reach in the standing position, while maintaining a fixed base of support. The FRT was developed as a dynamic measure of balance and is used to measure the ability to stand and lean forward without losing balance. The mean difference in centimeters between standing and leaning forward following three trials was calculated.
The TUG and FRT are clinically-meaningful relevant tests, quick to administer, which are frequently used in the clinical setting and patient’s homes (Benaim, Perennous, Villy, Rousseaux & Pelissier, 1999; Ng & Hui-Chan, 2005).
BC was assessed using the Activities-specific Balance Confidence (ABC) scale (Powell & Myers, 1995), which is a 16-item self-report measure of balance self-efficacy in maintaining static and dynamic balance control during functional tasks. Participants indicate their level of self-efficacy (0% – 100%) in performing the activity without losing their balance or becoming unsteady. The validity and reliability of the ABC scale after stroke has been established (Botner, Miller & Eng, 2005; Myers, Fletcher, Myers & Sherk, 1998).
Independence in BADL was assessed via an interview (Masedo, Hanley, Jensen, Ehde & Cardenas, 2005) using The Functional Independence Measure (FIM) (Granger, 1998). Each of the 18 activities (eating, dressing, grooming) are rated from 1–7, total scores ranging from 18–126 points, higher scores indicating more independence in BADL. Independence in IADL was assessed using the IADL questionnaire (Lawton & Brody, 1969; Lawton, Moss, Fulcomer & Kleban, 1982). Scores range from 0 (totally dependent) to 23 (total independent) in IADL by rating eight IADL domains such as shopping, use of transportation and cooking. Demographic and stroke information was also collected.
Statistical analyses
Descriptive statistics [mean (standard deviation) (SD) and median (inter quartile) (IQR)] were used to describe participants in terms of stroke, demographic information, mobility, balance, BC and daily-living. Normality Testing using Shapiro Wilks Test revealed that the dependent variables (TUG, FRT, ABC) were not normally distributed (p < 0.05) and since groups were uneven in size, non-parametric statistics were used. Differences between groups (with/without mild proprioception deficits) were assessed using Mann-Whitney U Test for continuous variables and Chi square for dichotomous variables. Spearman correlations assessed associations between mobility, balance and BC to BADL and IADL for all participants and within each group separately. Correlations ranging from 0.25 to 0.49 were considered fair, and values of 0.5 to 0.75 were considered moderate to good relationships (Portney & Watkins, 2000). Statistical significance was set at p < 0.05, and all analyses were conducted using SPSS for Windows version 23.0 (SPSS Inc, Chicago, IL).
Results
This paper includes a secondary analysis of 102 participants with chronic stroke, 64 of them are included in this analysis and are the focus of this paper. Thirty-four of the 102 participants did not undergo mobility and balance testing. Of the remaining 68 participants, according to the TLT; 45 participants had intact proprioception (scored 0), 19 participants had mild proprioception deficits (scored 1) and four participants had moderate proprioception deficits (scored 2). The four participants with moderate proprioception deficits were therefore excluded from this study.
The demographic and stroke information appears in Table 1. No significant differences were found for age, education, time since stroke and cognition between groups (with and without mild proprioception deficits). However, the mobility, balance, BC, independence in BADL and IADL was significantly higher for the participants with intact proprioception compared to the participants with mild proprioception deficits (Table 2).
Demographic and Stroke characteristics of all participants and participants divided into groups
Demographic and Stroke characteristics of all participants and participants divided into groups
MMSE – Mini Mental State Examination.
Mobility, balance, balance confidence and daily living of all participants and participants from both groups
TUG – Timed Up and Go Test; FRT – Functional Reach Test, ABC – Activities-specific Balance Confidence Scale; FIM – Functional Independence Measure; IADLq – Instrumental Activities of Daily Living questionnaire.
Significant weak-moderate correlations were found between mobility, balance and BC to BADL and IADL when assessed for all 64 participants (Table 3). However, when these correlations were assessed separately for each group, different associations were found (Table 3, Fig. 1). For the participants with intact proprioception; mobility, balance, and BC were significant moderately correlated to BADL but only balance was significantly correlated to BADL for participants with mild proprioception deficits. Mobility and BC were significant moderately correlated to IADL for the 45 participants with intact proprioception, but only mobility was significantly correlated to IADL for the 19 participants with mild proprioception deficits (Table 3). Balance (FRT) (r = 0.50, p < 0.001) and mobility (TUG) (r = – 0.53, p < 0.001) were significant moderately correlated to BC (ABC) for participants with intact proprioception, but these variables were not significantly correlated to BC for participants with mild proprioception deficits.
Correlation (Spearman) Matrix between mobility, balance and balance confidence to independence in daily living for all participants (N = 64), participants with intact proprioception (N = 45) and participants with mild proprioception deficits (N = 19)
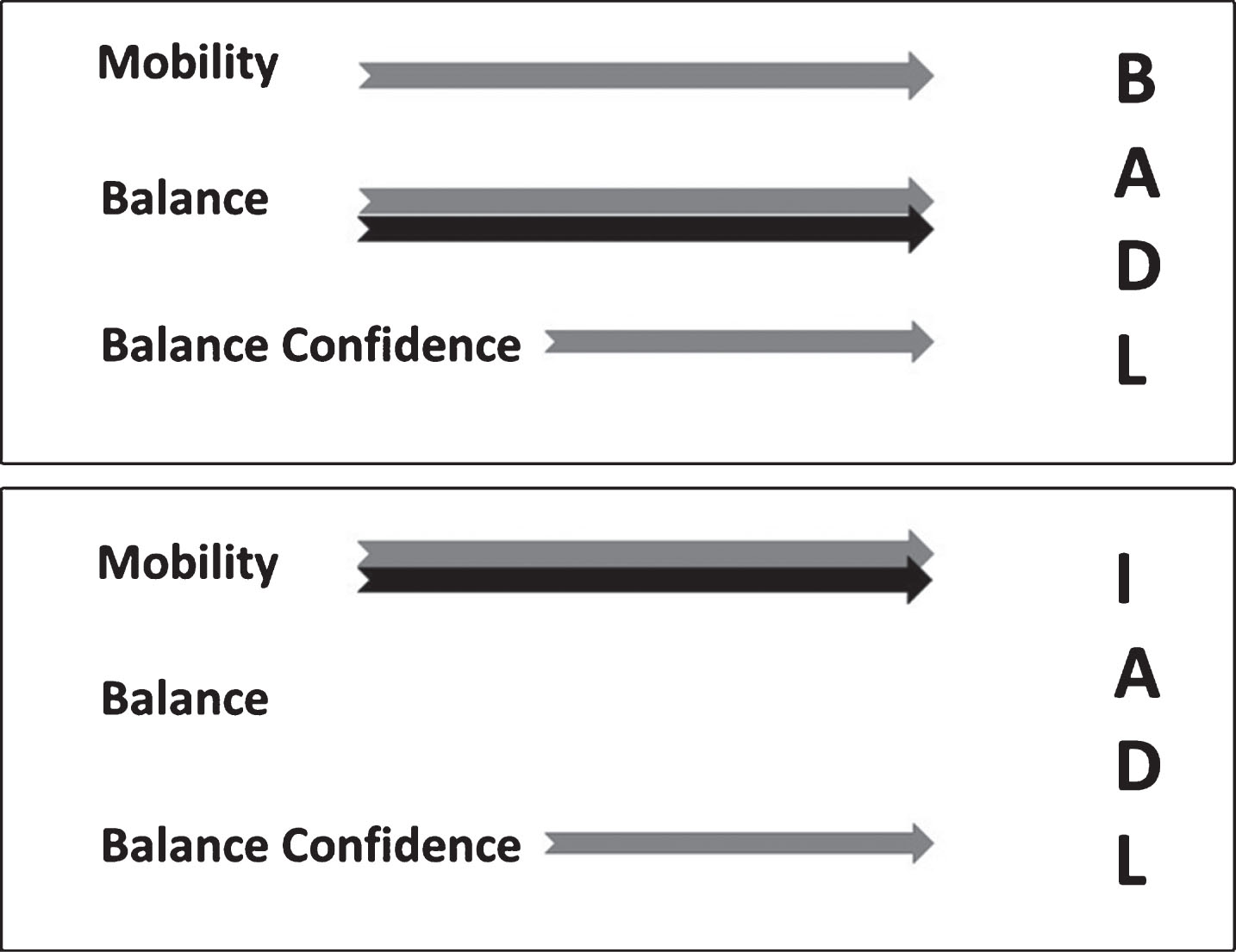
Arrows indicate significant correlations between mobility, balance and balance confidence to BADL (upper) and IADL (lower) for the participants with intact proprioception (grey) and participants with mild proprioception deficits (black).
The assessment and treatment of limitations in mobility, impaired balance and low BC have been the focus of many studies following stroke (e.g. Hellström et al., 2001; Hellstrom et al., 2003; Nian et al., 1999; Salbach et al., 2006; Torkia et al., 2016). However, these variables have not previously been investigated in relation to proprioception deficits in general and specifically at the chronic stage post-stroke. Since many individuals with chronic stroke are still dependent in IADL such as use of transportation, cooking or shopping, it is important to understand the underlying impairments that correlate with their daily living (Hartman-Maeir, Soroker, Ring, Avni & Katz, 2007).
This study compared two groups of participants with chronic stroke who differed in their ability to grasp their affected thumb with their eyes closed. Whereas 45 participants were able to grasp their thumb precisely, 19 participants just missed grasping their thumb but were able to correct quickly, demonstrating the presence of mild proprioception deficits. Interesting, despite no difference in time since stroke, age, education or cognitive status, these groups significantly differed in their mobility and balance, which are known to correlate with proprioception deficits.
The mobility of our 64 participants [TUG - 23.0 (18.6) secs] is similar to the reported mobility of individuals with chronic stroke who ambulate (Dean, Richards & Malouin, 2000; Ng & Hui-Chan, 2005). Significant differences were found between participants with and without mild proprioception deficits and when compared to published studies (Dean et al., 2000; Ng & Hui-Chan, 2005) the mobility of our participants with mild proprioception deficits is lower [32.6 (22.3) secs] and the mobility of our participants with intact proprioception is higher [18.9 (15.4) secs], indicating that proprioception deficits are a confounding factor.
The ability to maintain standing balance of our participants is similar to FRT scores reported for the participants with chronic stroke (Erel, Uygur, Engin Simsek & Yakut, 2011) [randomized to experimental and control groups 16.57 (10.01) and 22.50 (13.53) cm, respectively], despite the fact that our participants were older. Our participants with mild proprioception deficits leaned and reached a shorter distance compared to the participants with intact proprioception. This is possibly a direct result of the lack of proprioception, which is crucial for efficient balance and motor control (Means, 2013), which possibly also lead to poor BC.
BC is known to be compromised in individuals with stroke (Salbach et al., 2006), is therefore the focus of many interventions (Tang et al., 2015). This study revealed significant differences in BC between participants with and without mild proprioception deficits. The mean(SD) ABC scores of our 64 participants [59.4(23.5) out of 100% ] is similar to the mean(SD) ABC scores reported for a cohort of 89 community-dwelling individuals with stroke (Salbach et al., 2006) [59(21) out of 100% ].) However, our participants with mild proprioception deficits experienced significantly lower BC [44.4(22.8)] compared to the participants with intact proprioception [65.9(20.9)]. BC (ABC) has been reported to be significant moderately correlated to balance (assessed using the Berg Balance Scale) (r = 0.44) and mobility (TUG) (r = – 0.43) during the first year post-stroke (Salbach et al., 2006). Whereas, similar correlations with BC were revealed for all our 64 participants [balance (FRT) r = 0.50, p < 0.001; mobility (TUG) r = – 0.46, p < 0.001], when assessed separately for each group, they were no longer significant for the participants with mild proprioception deficits. BC is often low in participants with impaired balance (Yiu, Miller, Eng & Liu, 2012) and therefore, our participants with mild proprioception deficits might experience low BC as well as impaired balance. However, this was not supported by the non-significant correlations between balance and BC in this group. Hence, proprioception deficits may play an additional role in negatively affecting BC. Further research with a larger group of participants with mild proprioception deficits should be conducted. This implies that the focus of treatment for participants with proprioception deficits should be different, perhaps focusing on improving proprioception prior to improving balance and BC. Consequently, screening tests for proprioception deficits should be conducted to guide the intervention. The Thumb localization Test, which is a quick and easy test to administer, can be used.
As expected at the chronic stage, all participants were overall independent in BADL, yet, participants with intact proprioception were significantly more independent than participants with mild deficits. This has previously been demonstrated at the subacute stage (Gottlieb et al., 1997; Rand et al., 2001; Reding & Potes, 1988). Independence in IADL of all participants ranged from very dependent to more independent in complex daily activities such as shopping and cleaning but still, participants with intact proprioception were significantly more independent compared to the participants with mild proprioception deficits.
Mobility, balance and BC, which are known to correlate and contribute to independence in daily living (Kim & Park, 2014) were assessed in this study. Significant correlations were, in fact found between mobility, balance and BC with BADL and IADL for all participants but not when assessed separately for each group. For participants with mild proprioception deficits, only the ability to maintain balance was significantly correlated with independence in BADL. Whereas mobility and BC of participants with intact proprioception were significantly correlated to independence IADL, only mobility was significantly correlated to IADL for the participants with mild proprioception deficits. BC of participants with proprioception deficits seems not to play a role in explaining independence in daily living, possibly due to the substantial overarching effect of proprioception deficits on daily living.
The main limitation of this study is the fact that only one test (TLT), which has limited validity and reliability, was used to characterize proprioception deficits and divide the population into two groups. Nevertheless, this test significantly differentiated between groups in terms of mobility, balance, BC. The TLT is similar to other clinical tests for proprioception, with limited validity and reliability (Hillier et al., 2015). Adding another sensory tests could have possibly improved the accuracy of proprioception assessment in this study. This study is a secondary analysis and the groups were uneven in size, which is another study limitation, therefore findings should be interpreted cautiously and future research should recruit participants separately to create equal size groups. Only participants with mild proprioception deficits were included, in the future, studies should include participants with moderate and severe proprioception deficits as well.
To conclude, participants with chronic stroke who have mild proprioception deficits are not only more impaired in terms of mobility, balance and balance confidence, but are also less independent in BADL and IADL than participants with intact proprioception. Mild proprioception deficits seem to be a confounding factor for explaining independence in daily living at the chronic stage post-stroke. Screening for proprioception is important and therefore recommended for clinical practice and future research.
Conflict of interest
None to report.