
Abstract
BACKGROUND:
During gait training in persons with central nervous system (CNS) movement disorders, virtual reality (VR) can offer added value by providing task-specific gait training in more interactive and motivating environments.
OBJECTIVE:
To summarize current evidence for the effectiveness of VR-enhanced gait training in persons with CNS movement disorders.
METHODS:
PubMed, Web of Science and CENTRAL were systematically searched for studies using VR during walking to improve gait outcomes (spatiotemporal, functional, kinematic and kinetic). Meta-analyses were performed to estimate pooled effects.
RESULTS:
Eighteen studies with in total 337 patients were included (12 studies with people post-stroke, 4 with multiple sclerosis, 1 with Parkinson’s disease, 1 with traumatic brain injury). Spatiotemporal and functional parameters significantly improved in each population after the VR training. Compared to gait training without VR, differences in favor of VR were found for spatiotemporal and functional parameters only in people post-stroke.
CONCLUSION:
VR-enhanced gait training is an effective method to improve spatiotemporal and functional parameters in persons with CNS movement disorders. Current evidence supports that, in comparison to training without VR, for people post-stroke VR-enhanced gait training is more effective to improve gait function. Future research regarding other outcome measures and other CNS movement disorders is necessary.
Introduction
The recovery of functional gait is a key goal in the rehabilitation of persons with central nervous system (CNS) movement disorders, such as stroke, multiple sclerosis (MS) or Parkinson’s disease (PD) (Freivogel, Mehrholz, Husak-Sotomayor, & Schmalohr, 2008; Schwartz & Meiner, 2015). Gait impairments in this population contribute to an increased risk of fall, reduced mobility and poor quality of life (Niedermeier, Ledochowski, Mayr, Saltuari, & Kopp, 2017; Rossano & Terrier, 2016; Shema et al., 2014; Vanbellingen & Kamm, 2016). Therefore, regaining the ability to walk independently is of high priority (Freivogel et al., 2008).
Virtual reality (VR) is a relatively new tool emerging in the field of physical rehabilitation (Dockx et al., 2016; Tieri, Morone, Paolucci, & Iosa, 2018) and can be defined as “an artificial, computer-generated simulation or creation of a real-life environment or situation allowing the user to navigate through and interact with” (Baus & Bouchard, 2014). The use of VR in physical rehabilitation programs can offer several advantages. First, environments and situations that are too dangerous, expensive or impossible in real-life can be simulated with the use of VR. Second, these virtual environments (VEs) are fully controllable by therapists and researchers, giving the opportunity to bring real-life environments or situations, such as doing groceries in a supermarket, into the hospital (Tieri et al., 2018). Third, VEs are artificially made and can therefore easily be changed, creating the possibility to design personalized environments and therapies (Teo et al., 2016; Tieri et al., 2018). Fourth, VR has the potential to increase patients’ motivation by creating more exciting training environments resulting in more repetitions and longer training durations, ultimately improving patients’ treatment compliance (Howard, 2017; Tieri et al., 2018).
An important characteristic of VR is the degree of immersion. The degree of immersion has an impact on the users’ VR experience and affects their sense of presence (i.e. the feeling of being physically present) (Rose, Nam, & Chen, 2018). Based on the degree of immersion, VR systems and devices can be classified into three categories: fully immersive, semi-immersive and non-immersive (Rose et al., 2018). Fully immersive VR systems integrate the user completely into the VE by blocking out perception of the real-world. This can be achieved by using, for example, a head-mounted display (HMD). Semi-immersive and non-immersive VR systems let the user perceive both the real-world and a part of the VE. Large screen monitors, projections or multiple television screens can be classified under semi-immersive. A single television screen is an example of a non-immersive VR system. It is suggested that the exposure to a more immersive VE is able to elicit a stronger feeling of ’being physically present’ allowing the user to react in a more realistic way (Tieri et al., 2018).
Over the last 20 years, the popularity and use of VR in healthcare increased remarkably, and today, VR-based interventions already cover a wide range of areas in the field of rehabilitation (Pourmand, Davis, Lee, Barber, & Sikka, 2017). There is evidence suggesting that VR interventions for motor rehabilitation are beneficial in a number of population groups, such as people post-stroke, people with PD or MS, and for various outcome measures such as upper limb function or ADL function (Dockx et al., 2016; Laver, George, Thomas, Deutsch, & Crotty, 2015; Massetti et al., 2016; Thomson, Pollock, Bugge, & Brady, 2014). However, the efficacy of VR for gait training in persons with CNS movement disorders is still not clear. Although there is evidence that VR for upper limb training is at least as effective as conventional physical therapy, there is only limited evidence about the effectiveness of VR on gait in persons with CNS movement disorders (Laver et al., 2015). In order to establish a clear comprehension about VR and its effect on gait, this review will focus specifically on the effect of using VR while walking on the gait function in persons with CNS movement disorders.
The aim of this systematic review and meta-analysis is to provide an overview of the literature and to estimate pooled effects regarding the effect of VR used while walking on gait outcomes in persons with CNS movement disorders. This systematic review will address two questions: (1) Is VR-enhanced gait training effective to improve gait outcomes in persons with CNS movement disorders? and (2) Does VR-enhanced gait training elicit a greater effect on gait outcomes than training without VR in persons with CNS movement disorders?
Methods
Protocol and registration
The Cochrane Handbook and PRISMA statement were followed for the methodology and reporting of this systematic literature study (Higgins et al., 2011; Liberati et al., 2009). Protocol details were registered prospectively on PROSPERO (registration number: CRD42018083517).
Eligibility criteria
Studies were included if they met following inclusion criteria: Type of participants: Studies involved adults (>18 years old) with CNS movement disorders. No restrictions were made regarding gender, disease duration, or disease severity. Type of intervention: Studies investigated VR-enhanced gait training defined as the use of VR during walking with the aim to improve gait outcomes. The VR had to be an artificial, computer-generated simulation or creation of a real-life environment or situation and could be non–, semi–or fully immersive (Baus & Bouchard, 2014). Included were overground, treadmill and robot-assisted walking with or without body-weight support. Studies with and without control groups were included. However, for studies with a control group, the control group had to consist of the same population as the intervention group and had to receive an identical gait training without a VR component. If not, only data of the intervention group were included. The training had to consist of multiple sessions (>1 session). No further restrictions were made regarding training frequency and duration. Type of outcome: Studies assessed the pre-post and/or pre-follow up effect of VR during walking on spatiotemporal gait parameters (e.g. walking speed, step length, step time) (Hollman, McDade, & Petersen, 2011), functional gait (e.g. Timed Up and Go, 6-Minute Walk Test), lower limb kinematics and kinetics (e.g. range of motion and forces). Type of study design: Non–, quasi–or randomized controlled trials (RCTs), cohort studies or cross-sectional studies. Case studies or reports, narrative or systematic reviews, overview of reviews and protocols were excluded. Studies had to be published in English or Dutch.
Information sources and search
A search strategy was developed and refined in group discussions after preliminary searches. Electronic searches were conducted from inception till 04/10/2017 in PubMed and Web of Science and till 11/01/2018 in Cochrane Central Register of Controlled Trials (CENTRAL). Full electronic searches are provided in supplemental appendices S1, S2 and S3.
Study selection
Identification and selection of studies were conducted in a blinded standardized manner. With the use of Rayyan (Ouzzani, Hammady, Fedorowicz, & Elmagarmid, 2016) – a web application for the rapid exploring and filtering of eligible studies – titles and abstracts were screened to identify relevant studies. If studies were considered relevant, full paper copies were retrieved and eligibility was checked. Screening of the records was done double-blinded. Disagreements between authors (E.D.K., M.G., E.J.) were resolved by consensus. In case consensus could not be reached, an independent review author (E.S.) was consulted.
Data collection process and data items
A data extraction sheet was developed in order to collect data items of interest. One author (E.D.K.) extracted data from all included studies. This sheet was double-checked and completed by two other authors (M.G., E.J.). If the required data were absent or reported insufficiently, authors were contacted individually by email. If no averages were reported for these data, when possible the calculations (e.g. average age, disease duration) were performed by the researchers. From each individual study, following information was extracted: 1) patient characteristics (type of disorder, number, sex, age, disease duration), 2) VR hardware and type of VE, 3) level of immersion (non–, semi–or fully immersive), 4) type of walking (overground, treadmill or robot-assisted), 5) training duration, 6) training frequency and 7) gait outcomes.
Risk of bias assessment
Criteria for assessing the risk of bias in the included studies were based on the Cochrane Collaboration’s tool (Higgins et al., 2011) and the Methods Guide for Comparative Effectiveness Reviews (Viswanathan et al., 2008) (supplemental appendix S4). Following domains were rated “high”, “unclear” or “low”: sampling bias, selection bias (sequence generation, allocation concealment), performance bias, detection bias, attrition bias and reporting bias. Assessing the risk of bias was done double-blinded. Disagreements between authors (E.D.K., M.G., E.J.) were resolved by consensus. In case consensus could not be reached, an independent review author (E.S.) was consulted.
Summary measures and planned methods of analysis
The outcome measures were classified into 4 different categories: spatiotemporal gait parameters, functional gait, lower limb kinematics and kinetics. Results of studies including the same population and same outcome measure, were taken together for quantitative data analysis. The pooled mean differences (MD) and their 95% confidence intervals (CI) were calculated for continuous outcome measures that were reported in at least 2 studies. Meta-analyses were performed using the inverse variance method with the random effects model (Review Manager). A random effect model was chosen because we assumed that the true effect may vary across studies due to differences in study population or gait training.
Inconsistency across studies due to heterogeneity was assessed with the I2 statistic. I2 values greater than 50% were classified as important presence of heterogeneity (Deeks, Higgins, & Altman, 2011). Statistical significance of heterogeneity was based on the Chi-squared test’s p-value. A p-value of 0.10 was used as cut-off to detect statistical significance of the Chi-squared test (Deeks et al., 2011). If for some outcome measures significant important heterogeneity (I2 >50% and Chi2 test’s p-value <0.10) was present, data were not pooled. If outcome measures were reported in a single study, a descriptive analysis was provided.
Results
Study selection
Our total search yielded 1371 relevant articles in PubMed, Web of Science and CENTRAL. Figure 1 illustrates a flow diagram of the entire study selection process. Finally, 18 studies were included of which 14 were RCTs (Calabro, Naro, et al., 2017; Calabro, Russo, et al., 2017; Cho & Lee, 2013, 2014; Jung, Yu, & Kang, 2012; Kang, Kim, Chung, & Hwang, 2012; Kim, Choi, Lee, & Song, 2015; Mirelman et al., 2011; Peruzzi, Cereatti, Della Croce, Zarbo, & Mirelman, 2015; Peruzzi, Zarbo, Cereatti, Della Croce, & Mirelman, 2017; Sessoms et al., 2015; Yang et al., 2011; Yang, Tsai, Chuang, Sung, & Wang, 2008) and 4 clinical trials (Mao, Chen, Li, & Huang, 2015; Peruzzi, Cereatti, Della Croce, & Mirelman, 2016; Walker et al., 2010; Xiao et al., 2017). Of these 18 studies, 14 were used in quantitative synthesis (Calabro, Naro, et al., 2017; Cho, Kim, Lee, & Lee, 2015; Cho & Lee, 2013, 2014; Jung et al., 2012; Kang et al., 2012; Kim et al., 2015; Mao et al., 2015; Mirelman et al., 2011; Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017; Xiao et al., 2017; Yang et al., 2008).
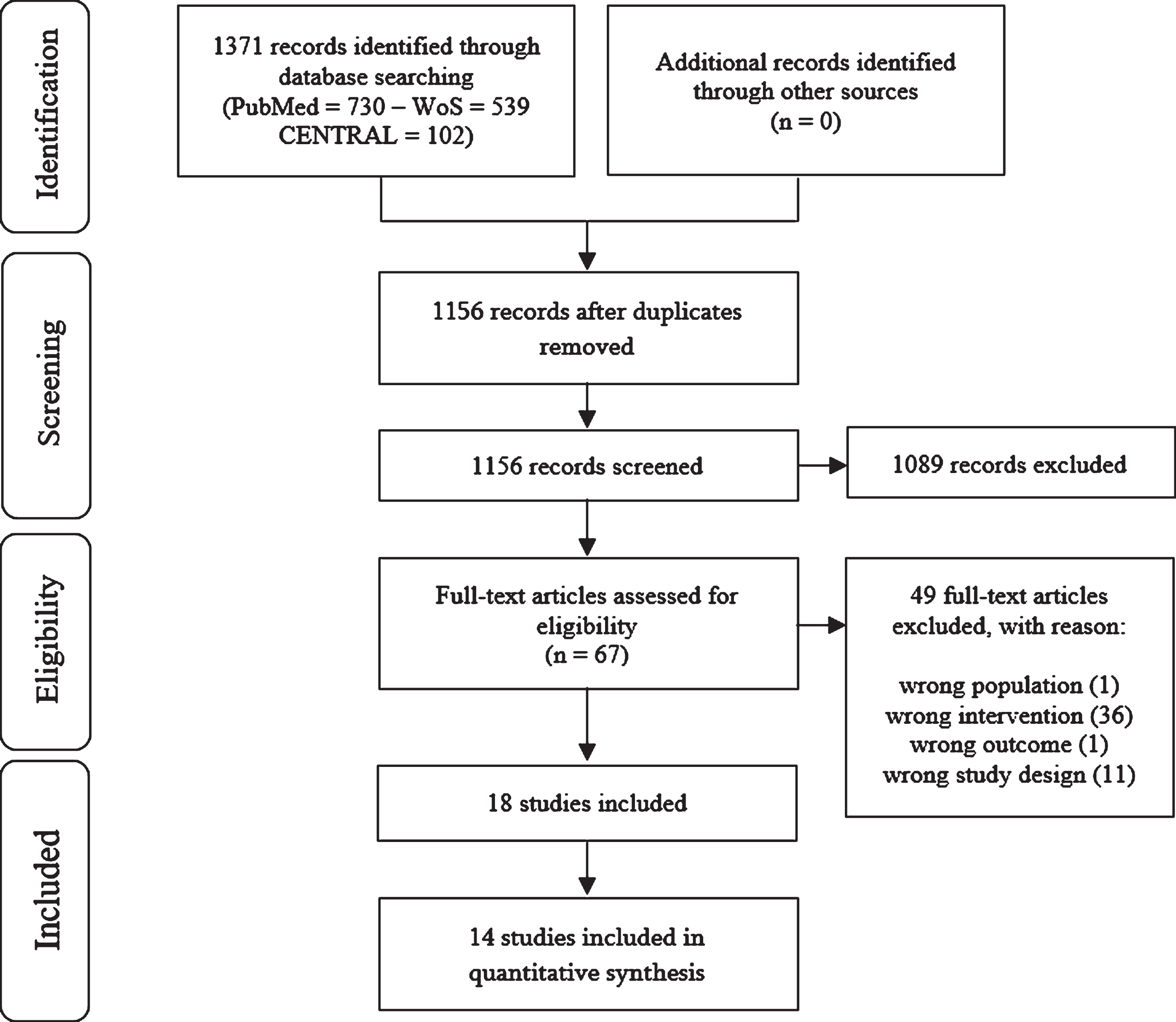
Flowchart of the study selection process.
Characteristics of included studies assessing the effect of VR-enhanced gait training on gait outcomes in persons with CNS movement disorders
Continues values are reported as mean (SD). Abbreviations: N: number, M: male, F: female, n/r: not reported, n/a: not applicable, VR: virtual reality, VE: virtual environment, HMD: head-mounted display, RAGT: robot-assisted gait training, TM: treadmill, RMI: Rivermead Mobility Index, Tinetti POMA: Tinetti Performance – Oriented Mobility Assessment, LL: lower limb, par: paretic side, SLSP: single limb support period, DLSP: double limb support period, BBS: Berg Balance Scale, TUG: Timed Up and Go, 6MWT: 6-Minute Walk Test, WAQ: Walking Ability Questionnaire.
Table 1 lists more detailed information about the study characteristics.
Patient characteristics
In total, 337 participants (155 males, 143 females and 39 unknown) were included (sample size: 6–20 participants). Out of 18 studies, 12 studies included people post-stroke (219 participants, age (pooled mean ± standard deviation): 58.7 ± 8.28 years, time post-stroke (pooled mean ± standard deviation): 18.09 ± 29.68 months) (Calabro, Naro, et al., 2017; Cho et al., 2015; Cho & Lee, 2013, 2014; Jung et al., 2012; Kang et al., 2012; Kim et al., 2015; Mao et al., 2015; Walker et al., 2010; Xiao et al., 2017; Yang et al., 2011; Yang et al., 2008), 4 studies people with MS (86 participants, age (pooled mean ± standard deviation): 43.3 ± 9.74 years, time after diagnosis (pooled mean ± standard deviation): 143.42 ± 67.22 months) (Calabro, Russo, et al., 2017; Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017), one study people with PD (20 participants, mean age ± standard deviation: 67.1 ± 6.5 years, mean time after diagnosis ± standard deviation: 117.6 ± 67.2 months) (Mirelman et al., 2011) and one study people with traumatic brain injury (TBI) (12 participants, mean age ± standard deviation: 27.5 ± 4.9 years, mean time after diagnosis ± standard deviation: not reported) (Sessoms et al., 2015).
Interventions
People post-stroke received VR-enhanced gait training with the combination of a treadmill and a screen in 8 studies (Cho et al., 2015; Cho & Lee, 2013, 2014; Kim et al., 2015; Mao et al., 2015; Walker et al., 2010; Xiao et al., 2017; Yang et al., 2011), a treadmill with a HMD in 2 studies (Jung et al., 2012; Kang et al., 2012), a treadmill with multiple screens in 1 study (Yang et al., 2008) and a robotic device (i.e. Lokomat exoskeleton) with a screen in 1 study (Calabro, Naro, et al., 2017). People with MS received VR-enhanced gait training by combining a treadmill with a screen in 2 studies (Peruzzi et al., 2015; Peruzzi et al., 2017), a robotic device (i.e. Lokomat exoskeleton) with a screen in 1 study (Calabro, Russo, et al., 2017) and a treadmill with either a HMD or a screen in 1 study (Peruzzi et al., 2016). In people with PD, the combination of a treadmill with a projection was used in 1 study (Mirelman et al., 2011). One study involving people with TBI combined a treadmill with a CAREN system (Sessoms et al., 2015). None of the studies combined overground walking with VR. In all studies, the training duration ranged between 3 weeks and 8 weeks and the number of sessions between 9 and 40 with a training time from 10 to 60 minutes. Only 3 studies included a follow up measurement after 4 weeks (Mirelman et al., 2011; Peruzzi et al., 2016; Yang et al., 2008).
Gait outcome measures
Following gait outcomes were reported in the included studies involving people post-stroke: spatiotemporal gait parameters (Cho et al., 2015; Cho & Lee, 2013, 2014; Kang et al., 2012; Kim et al., 2015; Walker et al., 2010; Xiao et al., 2017; Yang et al., 2011; Yang et al., 2008), functional gait (Calabro, Naro, et al., 2017; Cho & Lee, 2013, 2014; Jung et al., 2012; Kang et al., 2012; Walker et al., 2010; Xiao et al., 2017; Yang et al., 2008), lower limb kinematics (Mao et al., 2015) and lower limb kinetics (Calabro, Naro, et al., 2017). Studies regarding people with MS also included spatiotemporal gait parameters (Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017), functional gait parameters (Calabro, Russo, et al., 2017; Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017), lower limb kinematics (Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017) and lower limb kinetics (Calabro, Russo, et al., 2017; Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017). The study regarding people with PD reported spatiotemporal and functional gait parameters (Mirelman et al., 2011). The study involving people with TBI reported one spatiotemporal gait parameter (Sessoms et al., 2015).
For 8 studies, authors were contacted for missing data items of interest (Calabro, Russo, et al., 2017; Cho et al., 2015; Kim et al., 2015; Peruzzi et al., 2016; Peruzzi et al., 2015; Sessoms et al., 2015; Walker et al., 2010; Yang et al., 2011). One author provided us the missing data by email (Cho et al., 2015). For the remaining 7 studies, data items of interest remained missing. One author was not able to provide us the missing data of 2 included studies (i.e. more detailed results of the lower limb kinematic and kinetic data) because she moved abroad and had no longer access to those data (Peruzzi et al., 2016; Peruzzi et al., 2015). Authors of the remaining 5 studies did not respond. In 1 study (Kim et al., 2015), there was a mismatch regarding the results of step and stride length between the text and corresponding table. Since the author did not reply and it was clear that the correct results were written down in the text, we decided to use these results. The remaining 4 studies (Calabro, Russo, et al., 2017; Sessoms et al., 2015; Walker et al., 2010; Yang et al., 2011) and the results of only the lower limb kinematic and kinetic outcome measures of the 2 studies (Peruzzi et al., 2016; Peruzzi et al., 2015) could not be included in quantitative nor descriptive analysis and are not further discussed in synthesis below. Results of these studies are presented in supplemental appendix S5.
Risk of bias assessment
The risk of bias within studies is presented in Table 2. ’Sampling bias’ was rated high in 10 studies (Cho & Lee, 2013; Jung et al., 2012; Kang et al., 2012; Mao et al., 2015; Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017; Sessoms et al., 2015; Walker et al., 2010; Yang et al., 2011). Only 1 study recruited a random population sample (Calabro, Russo, et al., 2017) and in the remaining 7 recruitment was not or insufficiently reported (Calabro, Naro, et al., 2017; Cho et al., 2015; Cho & Lee, 2014; Kim et al., 2015; Mirelman et al., 2011; Xiao et al., 2017; Yang et al., 2008). ’Sequence generation’ was rated unclear in 10 studies (Calabro, Naro, et al., 2017; Cho et al., 2015; Cho & Lee, 2013, 2014; Kang et al., 2012; Mao et al., 2015; Peruzzi et al., 2015; Sessoms et al., 2015; Yang et al., 2011; Yang et al., 2008), only 4 studies had a random component in their sequence generation process (Calabro, Russo, et al., 2017; Jung et al., 2012; Kim et al., 2015; Peruzzi et al., 2017). ’Allocation concealment’ was rated low in 8 studies (Calabro, Naro, et al., 2017; Calabro, Russo, et al., 2017; Cho et al., 2015; Cho & Lee, 2013, 2014; Kang et al., 2012; Peruzzi et al., 2017; Yang et al., 2008), whereas in the remaining 6 studies the allocation of participants was not addressed or reported insufficiently (Jung et al., 2012; Kim et al., 2015; Mao et al., 2015; Peruzzi et al., 2015; Sessoms et al., 2015; Yang et al., 2011). ’Performance bias’ was rated low in all studies, except one where the amount of therapy was different between groups (Sessoms et al., 2015). The outcome assessor was blinded in 10 studies (Calabro, Naro, et al., 2017; Calabro, Russo, et al., 2017; Cho et al., 2015; Cho & Lee, 2013, 2014; Jung et al., 2012; Kang et al., 2012; Peruzzi et al., 2017; Yang et al., 2011; Yang et al., 2008). Only 2 studies, did not blind the outcome assessor (Mirelman et al., 2011; Walker et al., 2010) and in 6 studies blinding was not addressed or reported insufficiently (Kim et al., 2015; Mao et al., 2015; Peruzzi et al., 2016; Peruzzi et al., 2015; Sessoms et al., 2015; Xiao et al., 2017). ’Attrition bias’ was rated high in 1 study (Cho & Lee, 2013), where the missing data were likely to have an impact on the observed results and in 2 studies missing data were not reported (Jung et al., 2012; Yang et al., 2011). Only 3 studies provided a preregistered protocol (Calabro, Naro, et al., 2017; Calabro, Russo, et al., 2017; Xiao et al., 2017), in the remaining studies ’reporting bias’ was rated unclear.
Risk of bias assessment
Risk of bias assessment
Legend. +: high bias, ?: unclear bias, -: low bias, n/a: not applicable (one group studies),
Effect of VR on outcome measures reported in one study
Continues values are reported as mean (SD); ¥: values calculated based on reported means/SD. Abbreviations: MS: multiple sclerosis, PD: Parkinson’s disease, FU: follow up, n/a: not applicable, RMI: Rivermead Mobility Index, Tinetti POMA: Tinetti Performance – Oriented Mobility Assessment, DLSP: double limb support period, 6MWT: 6-Minute Walk Test, par: paretic side, 10MWT: 10-Meter Walk Test, FMA-LE: Fugl-Meyer Assessment – Lower Extremity, BBA: Brunel Balance Assessment, WAQ: Walking Ability Questionnaire, FSST: Four Square Step Test, EDDS: Expanded Disability Status Scale, ROM: Range of Motion, % GC: percentage of gait cycle. The asterisk (*) denotes a significant within-group difference.
Is VR-enhanced gait training effective to improve gait outcomes in persons with CNS movement disorders?
Detailed results of outcome measures that were reported in a single study are presented in Table 3.
VR-enhanced gait training in people post-stroke.
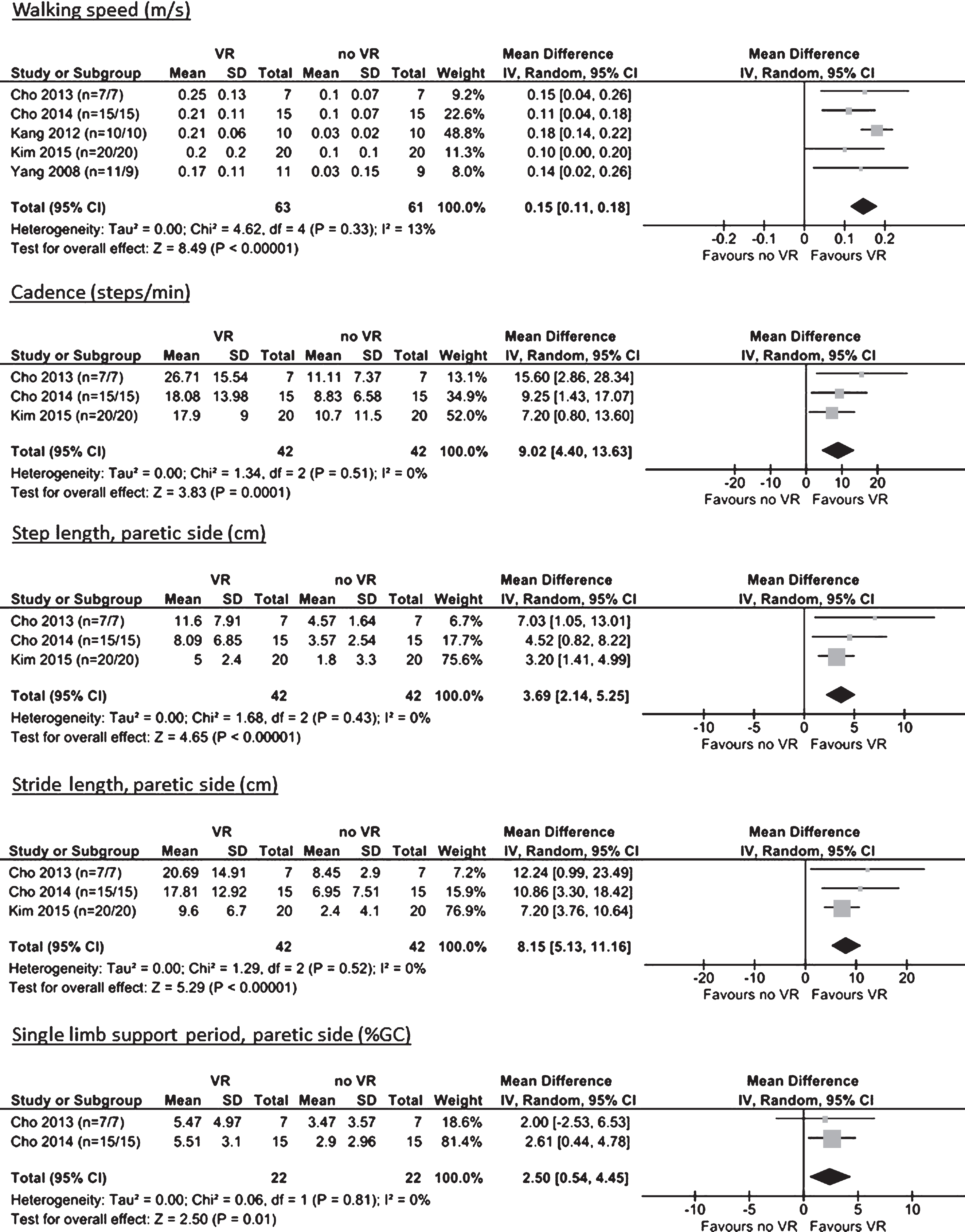
Spatiotemporal gait parameters were reported in 7 studies (Cho et al., 2015; Cho & Lee, 2013, 2014; Kang et al., 2012; Kim et al., 2015; Xiao et al., 2017; Yang et al., 2008), with in total 8 different gait parameters. For 5 parameters, a meta-analysis could be performed (Figure 2). The meta-analyses showed significant improvements for walking speed (MD 0.17 m/s, 95% CI 0.12 to 0.22, I2 = 0%), cadence (MD 15.59 steps/min, 95% CI 7.26 to 23.91, I2 = 29%), paretic step length (MD 6.53 cm, 95% CI 3.69 to 9.37, I2 = 0%), paretic stride length (MD 12.27 cm, 95% CI 6.98 to 17.56, I2 = 0%) and single limb support period (MD 5.49%, 95% CI 2.87 to 8.12, I2 = 0%). Paretic step time, paretic stride time and double limb support period were reported in 1 study only and also improved significantly after the VR intervention.

Effect of VR on spatiotemporal gait parameters in people post-stroke. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group, % GC: percentage of gait cycle.
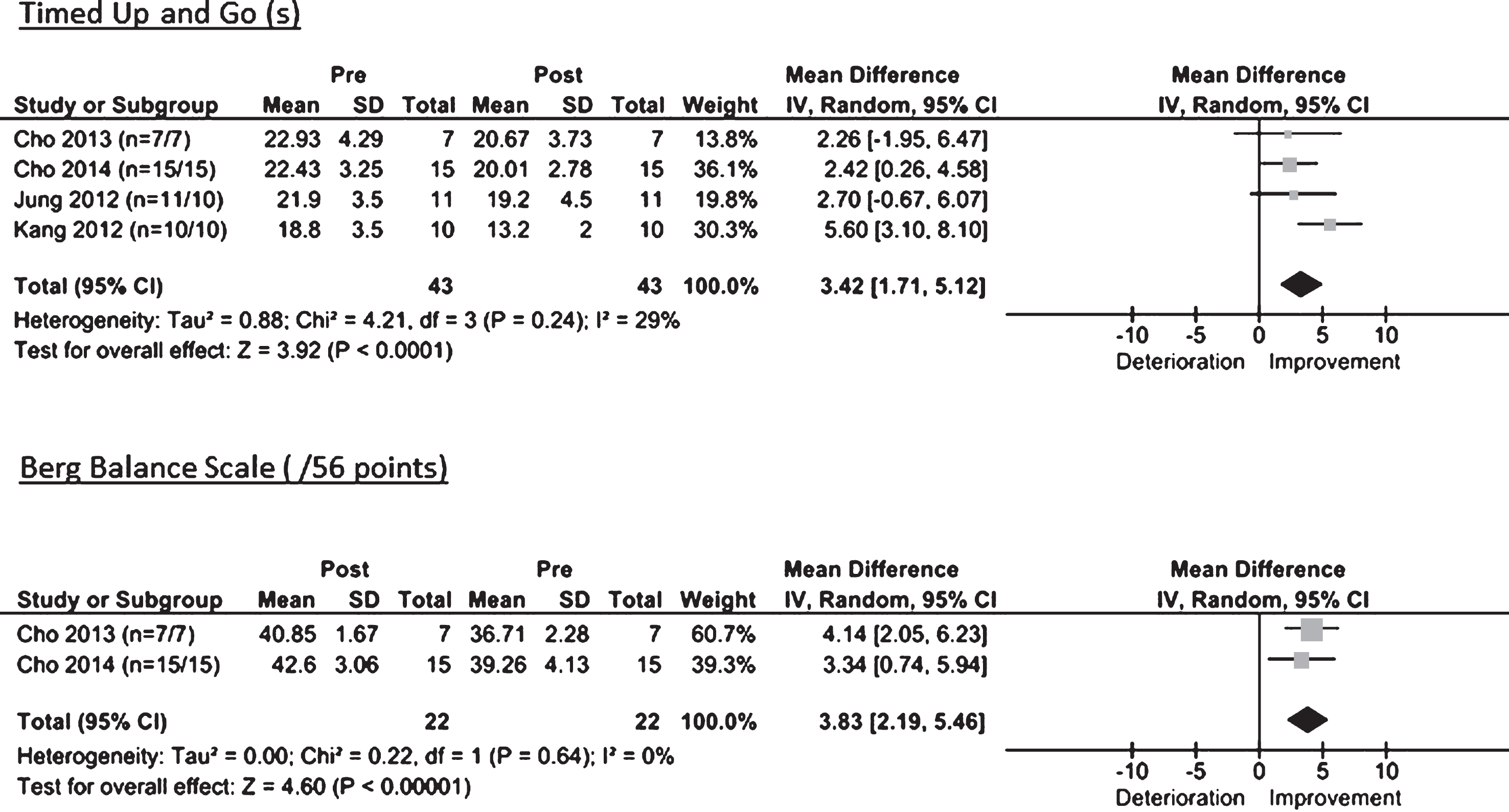
Effect of VR on functional gait in people post-stroke. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group
One study (Yang et al., 2008) investigated the long-term effect of VR on walking speed and reported that after 4 weeks, walking speed was still increased significantly.
Functional gait was reported in 7 studies (Calabro, Naro, et al., 2017; Cho & Lee, 2013, 2014; Jung et al., 2012; Kang et al., 2012; Xiao et al., 2017; Yang et al., 2008), with in total 10 different functional outcomes. For 2 outcomes, a meta-analysis could be performed (Figure 3). The meta-analyses showed significant improvements for both Timed Up and Go (MD 3.42 s, 95% CI 1.71 to 5.12, I2 = 29%) and Berg Balance Scale (MD 3.83, 95% CI 2.19 to 5.46, I2 = 0%). Regarding the 8 parameters reported in 1 study only, significant improvements were seen for the 6-Minute Walk Test, 10-Meter Walk Test, Fugl-Meyer Assessment, Community Walking Time, Walking Ability Questionnaire, Rivermead Mobility Index and Tinetti POMA. The Brunel Balance Assessment Scale was the only parameter that did not improve significantly.
One study (Yang et al., 2008) also assessed the long-term effect of VR on the Community Walking Time and Walking Ability Questionnaire. Both parameters were still improved significantly after the follow up period of 4 weeks.
Lower limb kinematics were reported in 1 study (Mao et al., 2015), measured by pelvic tilt, pelvic obliquity and pelvic rotation. No meta-analysis could be performed. The study reported a significant decreased amplitude of the pelvic anterior tilt post-intervention. No significant differences were observed for pelvic obliquity and rotation.
Lower limb kinetics were reported in 1 study (Calabro, Naro, et al., 2017), measured by the hip and knee forces. No meta-analysis could be performed. The study reported significant increases in both hip and knee forces after the VR intervention.
Spatiotemporal gait parameters were reported in 3 studies (Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017), with in total 4 different gait parameters. For 3 parameters, a meta-analysis could be performed (Figure 4). The meta-analyses showed significant improvements for walking speed (MD 0.11 m/s, 95% CI 0.02 to 0.20, I2 = 0%) and cadence (MD 6.22 steps/min, 95% CI 1.00 to 11.45, I2 = 0%). Stride length (MD 0.09 cm, 95% CI -0.02 to 0.19, I2 = 0%) did not improve significantly. Stride time, reported in 1 study only, also did not improve significantly after the VR intervention.

Effect of VR on spatiotemporal gait parameters in people with MS. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group.
One study (Peruzzi et al., 2016) investigated the long-term effect of VR on walking speed, stride length and stride time. The study reported no significant improvements after the follow up period of 4 weeks.
Functional gait was reported in 3 studies (Peruzzi et al., 2016; Peruzzi et al., 2015; Peruzzi et al., 2017), with in total 6 different functional outcomes. For all outcomes, a meta-analysis could be performed (Figure 5). The meta-analyses showed significant improvements for the Berg Balance Scale (MD 4.65, 95% CI 2.83 to 6.46, I2 = 0%), 6-Minute Walk Test (MD 32.87 m, 95% CI 1.51 to 64.22, I2 = 0%), 10-Meter Walk Test (MD 0.19 m/s, 95% CI 0.07 to 0.31, I2 = 0%) and Four Square Step Test (MD 1.80 s, 95% CI 0.14 to 3.46, I2 = 0%). The Timed Up and Go (MD 0.56 s, 95% CI -0.73 to 1.85, I2 = 0%) and Expanded Disability Status Scale (MD 0.60, 95% CI -0.05 to 1.25, I2 = 0%) did not improve significantly.

Effect of VR on functional gait in people with MS. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group
Added value of VR on gait outcomes reported in one study
Continues values are reported as mean(SD); ¥: values calculated based on reported means/SD. Abbreviations: MS: multiple sclerosis, FU: follow up, RMI: Rivermead Mobility Index, Tinetti POMA: Tinetti Performance – Oriented Mobility Assessment, DLSP: double limb support period, 6MWT: 6-Minute Walk Test, par: paretic side, WAQ: Walking Ability Questionnaire, EDSS: Expanded Disability Status Scale, ROM: Range of Motion, % GC: percentage of gait cycle. The asterisk (*) denotes a significant between-group difference.
One study (Peruzzi et al., 2016) investigated the long-term effect of VR on 6-Minute Walk Test, Four Square Step Test and Expanded Disability Status Scale. After the 4 week follow up period, only the Four Square Step Test and Expanded Disability Status Scale were significantly improved.
Lower limb kinematics were reported in 1 study (Peruzzi et al., 2017), measured by the hip, knee and ankle range of motion. No meta-analysis could be performed. The study reported significant increases of the hip and knee range of motion after the VR intervention. No significant differences were found for the ankle range of motion.
Lower limb kinetics were reported in 1 study (Peruzzi et al., 2017), measured by the hip and ankle power. No meta-analysis could be performed. The study reported a significant increase of only the hip pull-off flexor power. No significant differences were found for the ankle plantar-flexor power.
Spatiotemporal gait parameters were reported in 1 study (Mirelman et al., 2011), measured by walking speed, stride time and stride length. No meta-analysis could be performed, but the study reported significant improvements for all parameters. The study also assessed the long-term effect of VR and reported that only walking speed and stride length were still improved significantly after the 4 week follow up period.
Functional gait was reported in 1 study (Mirelman et al., 2011), measured by the Four Square Step Test. No meta-analysis could be performed. The study reported significant improvements for the Four Square Step Test after the VR intervention and after the 4 week follow up period.
Does VR-enhanced gait training elicit a greater effect on gait outcomes in persons with CNS movement disorders than training without VR?
Detailed results of the outcome measures that were reported in a single study are presented in Table 4.
Added value of VR during gait training in people post-stroke.
Spatiotemporal gait parameters were reported in 5 studies (Cho & Lee, 2013, 2014; Kang et al., 2012; Kim et al., 2015; Yang et al., 2008), with in total 8 different parameters. For 5 parameters, a meta-analysis could be performed (Figure 6). The meta-analyses showed significant differences between the two training arms for walking speed (MD 0.15 m/s, 95% CI 0.11 to 0.28, I2 = 13%), cadence (MD 9.02 steps/min, 95% CI 4.40 to 13.63, I2 = 0%), paretic step length (MD 3.69 cm, 95% CI 2.14 to 5.25, I2 = 0%), paretic stride length (MD 8.15 cm, 95% CI 5.13 to 11.16, I2 = 0%) and single limb support period (MD 2.50 %, 95% CI 0.54 to 4.45, I2 = 0%) all in favor of the VR intervention. Paretic step time, paretic stride time and double limb support period, parameters reported in 1 study only, also improved significantly more in the VR group than in the control group.
Added value of VR compared to gait training without VR on spatiotemporal gait parameters in people post-stroke. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group, % GC: percentage of gait cycle.

Added value of VR compared to gait training without VR on functional gait in people post-stroke. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group.
One study (Yang et al., 2008) also assessed the long-term effect of VR on walking speed and reported that after the 4 week follow up period, the intervention group was no longer significantly faster than the control group.
Functional gait was reported in 6 studies (Calabro, Naro, et al., 2017; Cho & Lee, 2013, 2014; Jung et al., 2012; Kang et al., 2012; Yang et al., 2008), with in total 7 different functional outcomes. A meta-analysis could be performed for 1 outcome (Figure 7). The meta-analysis showed a significant difference between the two training arms for the Berg Balance Scale (MD 1.97, 95% CI 1.22 to 2.73, I2 = 0%) favoring the VR intervention. Data of the Timed Up and Go could not be pooled due to significant statistical heterogeneity (I2 = 80%, P = 0.002). Regarding the 5 parameters reported in 1 study only, significant between-group differences were seen for the Rivermead Mobility Index, Tinetti POMA, 6-Minute Walk Test and Community Walking Time, favoring VR. No between-group difference was seen for the Walking Ability Questionnaire.
One study (Yang et al., 2008) assessed the long-term effect of VR on the Community Walking Time and Walking Ability Questionnaire and reported that after the 4 week follow up period the VR group scored significantly higher on the Walking Ability Questionnaire only.
Lower limb kinetics were reported in 1 study (Calabro, Naro, et al., 2017), measured by the hip and knee forces. No meta-analysis could be performed. Both hip and knee forces increased significantly more in the VR group.
Spatiotemporal gait parameters were reported in 2 studies (Peruzzi et al., 2015; Peruzzi et al., 2017), with in total 3 different parameters. A meta-analysis could be performed for all parameters (Figure 8). No between-group differences were observed for walking speed (MD 0.02, 95% CI -0.08 to 0.11, I2 = 0%), cadence (MD -0.52, 95% CI -6.01 to 4.97, I2 = 0%) and stride length (MD 0.01, 95% CI -0.11 to 0.13, I2 = 0%).

Added value of VR compared to gait training without VR on spatiotemporal gait parameters in people with MS. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control group.
Functional gait was reported in 2 studies (Peruzzi et al., 2015; Peruzzi et al., 2017), with in total 6 different functional outcomes. For 5 outcomes, a meta-analysis could be performed (Figure 9). Between-group differences were only seen for the Berg Balance Scale (MD 3.62, 95% CI 1.90 to 5.33, I2 = 0%), in favor of the VR. The Timed Up and Go (MD 0.04, 95% CI -1.27 to 1.36, I2 = 0%), 6-Minute Walk Test (MD -12.01, 95% CI -52.90 to 28.78, I2 = 0%), 10-Meter Walk Test (MD 0.10, 95% CI -0.05 to 0.25, I2 = 0%) and Four Square Step Test (MD 0.45, 95% CI -2.03 to 2.92, I2 = 0%) showed no between-group differences. The Expanded Disability Status Scale was reported in 1 study only and no between-group differences were observed.

Added value of VR compared to gait training without VR on functional gait in people with MS. Abbreviations: SD: standard deviation, IV: inverse variance, CI: confidence interval, Random: random effects model, n: number of participants in intervention group/control
Lower limb kinematics were reported in 1 study (Peruzzi et al., 2017), measured by the hip, knee and ankle range of motion. No meta-analysis could be performed. The hip and knee range of motion increased significantly more in the VR group. No between-group differences were found for the ankle range of motion.
Lower limb kinetics were reported in 1 study (Peruzzi et al., 2017), measured by the hip and ankle power. No meta-analysis could be performed. The hip pull-off flexor power increased significantly more in the VR group. No between-group differences were observed for the ankle plantar-flexor power.
This systematic review and meta-analysis answered two questions: (1) Is VR-enhanced gait training effective to improve gait outcomes in persons with CNS movement disorders? and (2) Does VR-enhanced gait training elicit a greater effect than training without VR in persons with CNS movement disorders?
This meta-analysis specifically focused on the effect of VR on gait outcomes in persons with CNS movement disorders. In comparison to previous reviews, which focused more on the use of VR to improve upper limb function, postural balance or mobility in general (Casuso-Holgado et al., 2018; Corbetta, Imeri, & Gatti, 2015; Dockx et al., 2016; Gibbons, Thomson, de Noronha, & Joseph, 2016; Laver et al., 2015), this review is the first that provides a more in-depth knowledge about VR-enhanced gait training and its effect on several gait outcomes (i.e. spatiotemporal, functional, kinematics and kinetics).
Our results stipulated that VR-enhanced gait training is an effective approach to improve gait function in persons with CNS movement disorders. We found strong evidence that VR-enhanced gait training is effective to improve spatiotemporal and functional gait parameters in people post-stroke. Improvements in these parameters were not only statistically significant, but also exceeded the minimal clinically important difference (MCID) of 0.15 to 0.25 m/s for walking speed, 3.4 to 4.9 points for the Berg Balance Scale and 3.8 to 2.9 seconds for the Timed Up and Go, reported in previous studies by Flansbjer and colleagues (Flansbjer, Blom, & Brogardh, 2012; Flansbjer, Holmback, Downham, Patten, & Lexell, 2005). In people with MS, improvements in walking speed and the Berg Balance Scale also exceeded the MCID of 0.10 to 0.20 m/s and 3 points, respectively (Bohannon & Glenney, 2014; Gervasoni, Jonsdottir, Montesano, & Cattaneo, 2017). However, due to the lower number of studies – only 4 studies were identified regarding people with MS – more research within this population is necessary to strengthen the current evidence. For the effects on kinematics and kinetics, as well as for the influence of VR-enhanced gait training in people with PD and TBI, there is still insufficient evidence.
Furthermore, our results indicated that, overall, VR-enhanced gait training is more effective than an identical gait training without VR to improve spatiotemporal gait parameters (i.e. walking speed, cadence, step length, stride length, single limb support period) and functional gait parameters (i.e. Timed Up and Go) in people post-stroke. By ensuring that the use of VR was the only difference between the two interventions, differences in results could truly be attributed to VR. In people with MS, only the Berg Balance Scale showed larger improvements after VR-enhanced gait training compared to gait training without VR. For other outcome measures, no between-group differences were observed, indicating that VR-enhanced gait training is as effective as training without VR to improve gait function in people with MS. Here too, insufficient evidence was found for the added value of VR on kinematics and kinetics, as well as for people with PD and TBI. Moreover, for both research questions, there are other CNS movement disorders such as spinal cord injury or cerebral palsy for which no studies were found that investigated the effect of VR-enhanced gait training on gait function.
Although it is becoming more clear that VR-enhanced gait training could be an effective therapeutic approach, it still cannot be said which sort of VR training is the most suitable for improving patients’ gait function. A critical point of gait training is to preserve patients’ interest while performing these repetitive training tasks and ensure a continued motivation to complete the training. VR has the potential to increase patients’ motivation and enjoyment by offering more interactive environments during the gait training. There are several aspects of VR that could influence its effectiveness in improving patients’ gait function such as the level of immersion (i.e. non–, semi–, or fully immersive). Recent literature suggests that more immersive VR systems can generate a stronger feeling of ’being physically present’ and could therefore bring additional benefits compared to training with less immersive VR systems (Menin, Torchelsen, & Nedel, 2018; Tieri et al., 2018). Nevertheless, in this review only three studies used a fully immersive HMD (Jung et al., 2012; Kang et al., 2012; Peruzzi et al., 2016), whereas the majority of the included studies provided patients with non-immersive VR (i.e. a single TV-screen). Although a recent review of Rose et al. (2018) found no distinct correlation between the level of immersion and performance/motor recovery, it is not clear whether this also applies in improving specifically the gait function and more research is still needed.
In addition to the level of immersion, differences between the VEs in which patients had to walk were also observed in the included studies. In a previous review with meta-analysis regarding stroke rehabilitation, VR therapies using either customized VEs or commercially available games (e.g. Wii games, PlayStation games) were both found to be effective to improve balance and upper and lower limb function (Lohse, Hilderman, Cheung, Tatla, & Van der Loos, 2014). Although this review did not include any commercially available games, in general we also could distinguish two main groups: one in which patients were given an assignment (e.g. collecting coins, passing obstacles, searching for items) (44% or 8/18 studies) and one in which patients did not receive any assignment and just had to walk around in the VE (56% or 10/18 studies). This review did not find any notable differences between these two groups, however it is plausible that by adding some sort of game to the VE it could alter the effect by, for example, influencing the motivation and pleasure of the patients. More research is needed in order to make a statement about this. In addition, there are other factors, such as motion sickness, associated costs of implementation, and usability of the different VR displays that also need to be taken into consideration when using VR to enhance gait training in persons with CNS movement disorders.
In order to improve the walking ability of persons with CNS movement disorders, it is important to offer an intensive gait training with a high level of repetitions. A highly repetitive VR training where patients had to walk for at least 30 minutes was provided in the majority of the included studies. In 4 studies patients walked less than 30 minutes (Sessoms et al., 2015; Walker et al., 2010; Yang et al., 2011; Yang et al., 2008), however these studies found also positive effects which may indicate that VR-enhanced gait training can be found effectively, even with shorter training times.
In all included studies patients walked on a treadmill. A combined treadmill training with a robotic device (i.e. Lokomat exoskeleton) was done in only two studies (Calabro, Naro, et al., 2017; Calabro, Russo, et al., 2017). It appears that just like VR-enhanced treadmill training, adding VR to robot-assisted gait training is more effective in people post-stroke (Calabro, Naro, et al., 2017) and equally effective in people with MS (Calabro, Russo, et al., 2017). Nevertheless, this is based on one study in each population, so more research regarding VR combined with robot-assisted gait training is desirable.
The majority of gait outcomes could be classified under spatiotemporal and functional gait parameters, for which we found evidence favoring the use of VR. The most employed outcome measures were walking speed (67% or 12/18 studies), stride length (44% or 8/18 studies), Timed Up and Go (39% or 7/18 studies), cadence (33% or 6/18 studies) and Berg Balance Scale (33% or 6/18 studies). The influence of VR-enhanced gait training on kinematics and kinetics is still largely unknown, probably because this is more difficult to routinely test as it requires more expensive material, more time and specialized personnel who can interpret the results. The long-term effects of VR-enhanced gait training were only investigated in three studies, all included a follow up period of 4 weeks. Since each study included a different type of population – one included people post-stroke, one people with MS and one people with PD – it would be interesting to investigate this area in future studies.
Certain patient characteristics, such as disease duration or severity, can influence the results of VR-enhanced gait training. Our data, however, did not allow us to make a statement about this. For example, regarding time post-stroke almost all of the included studies recruited people who had a stroke more than 6 months before study enrolment, with only 3 studies investigating subacute stroke patients. Moreover, disease severity was not consistently reported in the included studies. All people with MS had an EDSS score below 6, meaning that they were still able to walk without walking aids. It is very likely that VR-enhanced gait training may be of greater importance during the subacute phase of stroke or in non-ambulatory patients as there is a stronger capacity of recovery. It is therefore also advisable for future research to focus on this population.
This systematic review demonstrated some limitations that have to be taken into consideration when interpreting the results. First, there was only a limited number of studies that assessed the effect of VR-enhanced gait training on the same gait-related outcome measure. As a result, the majority of the meta-analyses performed in this review consisted of only 2 or 3 studies, which lowers the strength of evidence. The second issue was the low number of studies included in this review for following population groups: people with MS (4 studies), people with PD (1 study) and people with TBI (1 study). Therefore, in order to establish a clear comprehension about the effectiveness of VR-enhanced gait training in these type of patients and other CNS movement disorders, more research is necessary.
Conclusion
VR has the potential to improve conventional gait training used today. Therefore, understanding the effect that VR-enhanced gait training has on the gait function in persons with CNS movement disorders is important for clinicians. This systematic review and meta-analysis supports that VR-enhanced gait training is an effective method to improve spatiotemporal gait parameters and functional gait in people with stroke and MS after 3 to 8 weeks of training. Current evidence also supports that, in comparison to training without VR, VR-enhanced gait training could be a more effective approach for people post-stroke. No added value was seen when VR was added to the gait training of people with MS. Additional research within other CNS movement disorders (e.g. PD, TBI, spinal cord injury, cerebral palsy) is needed to permit judgement about the effect of VR.
Conflict of interest
E.D.K has an interim fellowship for one year funded by the Vrije Universiteit Brussels, Belgium. N.L. is a strategic basic research fellow funded by the Research Foundation Flanders (FWO). The authors declare no further potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Acknowledgements
The authors would like to thank drs. Ward Willaert and dra. Amber Werbrouck for their assistance in the initial stages of this systematic review in terms of general ideas and preparatory work on the development of the search strategy.