
Abstract
INTRODUCTION:
Although the role of trunk exercises in the chronic phase of stroke is acknowledged, the addition of specific inpatient training in the subacute stage is a matter of debate and varies among centers. Recent new evidence suggests the question should be revisited.
OBJECTIVE:
To assess the impact of the addition of specific trunk training to inpatient rehabilitation protocols after a recent stroke.
METHODS:
A systematic review was performed assessing the impact of inpatient trunk training. The search was performed in LILACS, SciELO, PEDro, Cochrane, and NCBI PubMed databases for clinical trials published up to December 31st, 2017. The initial bibliographic research identified 3202 articles. After analyzing the titles, 19 abstracts were selected for detailed analysis. After application of the eligibility criteria, the final selection included nine studies. Outcome measurements from the same evaluation instruments were submitted to a meta-analysis to improve homogeneity (7 studies).
RESULTS:
All patients in the included studies were recruited less than three months after a stroke. Seven studies assessed trunk control using the Trunk Impairment Scale (TIS). There was a significant improvement in trunk control with a pooled increase in TIS score of 3.3 points from the baseline (CI95:2.54–4.06, p < 0.0001). Three studies assessed balance using the Brunel Balance Assessment (BBA) scale. There was also a significant improvement in balance with a pooled increase in BBA score of 2.7 points (CI95:1.5–4.03, p < 0.0001). The Berg Balance Scale was used for balance assessment in three studies. The meta-analysis of their results showed a pooled increase of 13.2 points (CI95:9.49–16.84, p < 0.0001). Weight transfer was evaluated in four studies using different methods. The addition of inpatient trunk exercises was associated with an improvement in the ability to transfer the trunk laterally in three studies.
CONCLUSION:
The introduction of trunk-based inpatient training protocols brings short-term benefits in trunk performance and balance in stroke patients.
Introduction
Although stroke sequelae vary in location and extent of the cerebral lesion (Pompeu, Pompeu, Rosa, & Silva, 2011), hemiparesis is the most frequent motor deficit. Consequently, trunk control is often compromised as a result of multidirectional losses involving flexor, extensor, and rotator muscles (Tanaka, Hachisuka, & Ogata, 1997, 1998). The postural asymmetry and altered weight bearing generate instability and gait disturbance (Trindade, 2011).
Adequate rehabilitation has the potential to enhance proximal stabilization, improving balance and reducing the risk of falls (Cabanas-Valdes et al., 2016; Karatas, Cetin, Bayramoglu, & Dilek, 2004; Ryerson, Byl, Brown, Wong, & Hidler, 2008; Sorinola, Powis, & White, 2014). Even when walking is difficult, trunk exercises can positively influence sitting balance, which mostly depends on trunk muscles (Cabanas-Valdes et al., 2016; Sorinola et al., 2014). In addition to treating weakness, specific exercises work on the harmonization of trunk and limb movements for the enhancement of functional ability. Trunk performance is currently recognized as a predictor of functional recovery and outcome after stroke (Hsieh, Sheu, Hsueh, & Wang, 2002; Karthikbabu et al., 2012; Sorinola et al., 2014).
The benefit of trunk exercises during the chronic phase of stroke is acknowledged, but the addition of specific training in the subacute and early phases is a matter of debate and varies among centers. Most evidence comes from studies focused on chronic patients or ambulatory strategies. However, this experience is not transposable to recent stroke victims, as they present different weakness and mobility patterns. Spasticity is generally less severe, albeit variable, and the environmental characteristics of hospital facilities influence therapy. Furthermore, such patients often undergo simultaneous treatments for active clinical conditions, which raises questions about the priority order of the patient’s problems and the optimization of the therapeutic strategies.
A 2014 meta-analysis summarized the effect sizes reported in clinical trials with inpatients and outpatients (Sorinola et al., 2014). The study showed moderate evidence that the addition of specific exercises improved standing balance and mobility. No significant difference was observed for trunk performance and functional independence. There was considered to be limited evidence at that time to support the addition of specific trunk exercises to conventional rehabilitation, and insufficient evidence to evaluate the effect on trunk performance and overall functional independence.
Generalization of findings is difficult because data on the efficacy of inpatient trunk training during the first months after stroke comes from a limited number of studies with small sample sizes. In addition, different quantification tools have been used, which may be a source of confusion. The typical solution to these problems is to combine values from different instruments into a single numeric scale by calculating the effect size. However, this strategy is limited by the need for certainty that all measurements assessed exactly the same effects, which is rarely the case in performance scales. It introduces heterogeneity and bias, which can lead to overestimation of an effect or masking of important phenomena (Puhan, Soesilo, Guyatt, & Schunemann, 2006).
A strong statistical correlation should exist between scores for the instruments to be safely combined (Puhan et al., 2006). It has been noted that there is loss of homogeneity during standardization due to standard deviations varying between results expressed in different units. In the specific question of the benefit of trunk exercises, these issues may have limited the interpretation of results in previous assessments. In addition, new clinical trials have been published in the last five years. Thus, the present study presents an update meta-analysis for assessment of the impact of the addition of specific in-patient trunk training in the first three months after stroke. We propose a conservative approach including the new data but restricting the analysis to results expressed in the same units and using the same instruments for assessment.
Methods
This review was planned and conducted according to the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyzes) (Moher, Liberati, Tetzlaff, Altman, & Group, 2009).
Search strategy and study selection
We included randomized clinical trials (RCTs) that evaluated the effects of inpatient trunk training on stroke victims. The search was performed in the LILACS, SciELO, PEDro, Cochrane NCBI and PubMed database for studies published up to December 31, 2017, using keywords related to cerebrovascular accidents, trunk training, and trunk control, as follows: (((“brain injury” OR “cerebrovascular accident” OR “brain ischemia” OR “intracranial arterial diseases” OR “intracranial hemorrhages” OR “brain infarction” OR “stroke”)) AND (“physical therapy” OR “exercise therapy” OR “exercise” OR “trunk exercise” OR “trunk exercise” OR “trunk performance” OR “trunk training”)) AND (“trunk function” OR “trunk balance” OR “trunk control” OR “balance” OR “trunk”). Reference lists from significant studies and review articles were also consulted for additional inclusions. An English language restriction criterion was used.
Inclusion and exclusion criteria
An initial evaluation of titles and abstracts was performed. To be included in the study, publications had to be a randomized clinical trials in which participants were stroke victims attending inpatient rehabilitation protocols. The study also had to have a control group with patients undergoing conventional rehabilitation and to have used at least one validated measurement tool to assess trunk control, balance or weight-transfer ability. Studies on patients with neurological pathologies other than stroke, those in the chronic phase, or those performed in outpatients were excluded.
Eligibility and quality assessment
The initial bibliographic research identified 3202 articles. After analyzing the titles, 19 abstracts were selected for detailed analysis and considered potentially relevant. Two independent authors (DCBS; MSS) examined the full texts of the selected publications to confirm eligibility. If at least one of the authors considered it an eligible reference, it was examined for possible inclusion. In case of disagreement on the fulfillment of inclusion or exclusion criteria, the evaluators discussed together for adjudication.
After application of the eligibility criteria, the final selection included nine studies (Buüyuükavcı, Şahin, Sağ, Doğu, & Kuran, 2016; Cabanas-Valdes et al., 2016; Fujino et al., 2016; Haruyama, Kawakami, & Otsuka, 2017; Howe, Taylor, Finn, & Jones, 2005; Karthikbabu et al., 2011; Kumar, Babu, & Nayak, 2012; Saeys et al., 2012; Verheyden et al., 2009). Figure 1 shows the study selection process.

Flow diagram of study search and selection.
The publications were then analyzed using the Physiotherapy Evidence Database (PEDro) scale for quality assessment (de Morton, 2009; Verhagen et al., 1998). This scale has 11 criteria that assess the quality of RCTs and whether sufficient statistical information was reported for the interpretation of results. In addition, the studies were assessed for risk of bias by two authors (DCBS, ILM) using the Cochrane Risk of Bias tool.
Descriptive data and the results of the rehabilitation protocols were extracted using standardized electronic forms adapted from the Cochrane Collaboration model for data extraction and were added to a computerized database. Data extracted from the publications included author, year, allocation groups, number of patients in each group, blinding measures, time since stroke, therapy protocol in each group, outcome measurement instruments, number of therapeutic sessions, treatment duration, length of follow-up, loss of follow-up, baseline measurements and all outcome measurements
Statistical analysis
Continuous variables were expressed as mean±standard deviation (SD). When pertinent, intervals (minimum value – maximum value) were also reported, frequencies and percentages were calculated for the categorical variables. Mean difference forest plots were used for continuous outcomes that varied from baseline. A random-effect model was used applying the inverse variance method. A pooled score change different to 0 favored a specific therapy modality. The effect of the intervention was considered statistically significant with 95% confidence intervals for the pooled score change not overlapping 0 in the forest plot. Higgins I2 was used to check for heterogeneity of the combined result. Studies were considered heterogeneous with p < 0.10, I2 > 50%, or evident methodological sources of heterogeneity. The random effect model was used for heterogeneity. Potential sources of heterogeneity were investigated by subgroup analysis. Sensitivity analysis was conducted excluding studies one by one. The statistical significance threshold was considered to be p < 0.05. The software used for statistical analysis was Review Manager, version 5.3 (Cochrane, Copenhagen, 2014).
Results
Study characteristics
The study sample sizes ranged from 20 to 80 (Table 1). The program duration ranged from one to eight weeks, with frequencies ranging from 3 to 8 times per week (mean 4.6±2.4) and the duration of each session ranged from 30 minutes to 1 hour (mean 43.1±14.9 min). The studies included patients of both genders with a diagnosis of ischemic or hemorrhagic stroke. Ages were not always described; however, the maximum limit for inclusion was reported to be 85 years.
Summary of basic characteristics
Summary of basic characteristics
Qualified physiotherapists in hospital settings conducted the exercises. The effect of trunk training on trunk control was assessed using the Trunk Impairment Scale (TIS) or the Trunk Control Test (TCT). The studies used different methods to assess weight-transfer ability, such as Side Reach Test, Standing Static Equilibrium, Sit and Rise Test, and Kinematic Analysis. Balance-related abilities were assessed through variable tools such as the Fourth Balance Scale (FTBS), Berg Balance Scale (BBS), Dynamic Gait Index (DGI), Brunel Balance Assessment (BBA), Tinetti Scale, Function in Sitting Test, Balance Evaluation Systems Test-brief version (Brief-BESTest), Functional Reach Test, Timed Up-and-Go Test (TUG), and Functional Ambulation Category (FAC). A meta-analysis was performed on studies assessing performance using the same clinical tool, which was the case for trunk control (TIS, seven studies) (Buüyuükavcı et al., 2016; Cabanas-Valdes et al., 2016; de Morton, 2009; Haruyama et al., 2017; Karthikbabu et al., 2011; Kumar et al., 2012; Saeys et al., 2012; Verhagen et al., 1998; Verheyden et al., 2009) and balance (BBA and BBS, three studies each) (Buüyuükavcı et al., 2016; Cabanas-Valdes et al., 2016; Karthikbabu et al., 2011; Kumar et al., 2012; Saeys et al., 2012).
The PEDro scale quality evaluation showed a mean score of 7.55±1.13 (mean±standard deviation, range 5-9) (Table 2). All nine studies were rated as at high risk of bias, due to the impossibility of blinding of participants.
Summary of quality assessment results
Eight studies (Buüyuükavcı et al., 2016; Cabanas-Valdes et al., 2016; Fujino et al., 2016; Haruyama et al., 2017; Karthikbabu et al., 2011; Kumar et al., 2012; Saeys et al., 2012; Verheyden et al., 2009) evaluated trunk control. The increment in scores was superior in the interventional groups in relation to control groups in all studies. Nevertheless, measurable improvement was present in all control groups.
A meta-analysis of the seven studies assessing trunk control by TIS is presented in Fig. 2. The analysis included 291 participants, of which 148 were randomized to the treatment group and 143 to the control group. There was a highly significant improvement effect on trunk control with a pooled increase in TIS score of 3.3 points from the baseline (p < 0.00001). A moderate level of heterogeneity was observed (58%). A sensitivity analysis removing studies one by one and filtering according to the time of follow-up and the baseline scores did not substantially impact the effect size or heterogeneity.
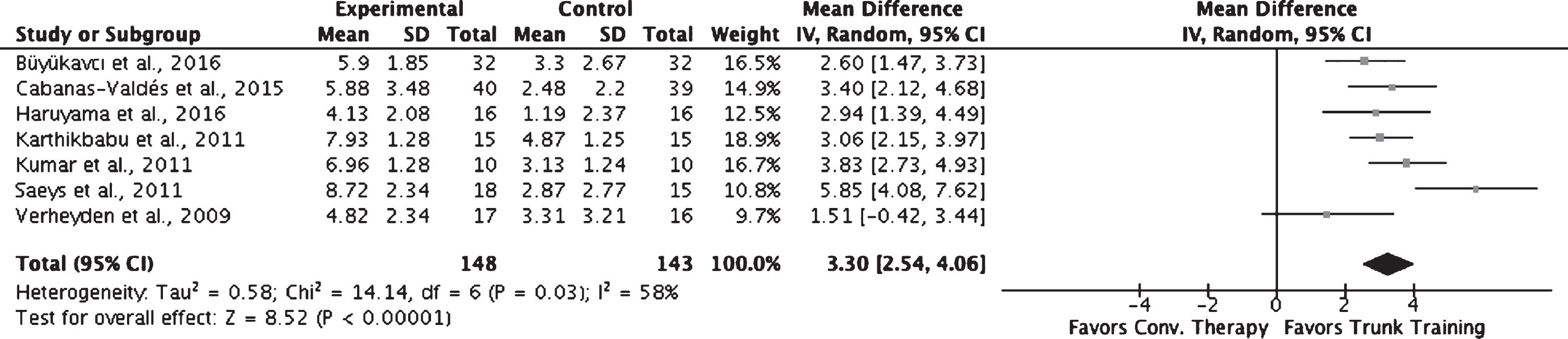
Forest plot of the meta-analysis from seven randomized clinical trials on the effect of trunk exercises on the Trunk Impairment Scale scores.
Seven studies (Buüyuükavcı et al., 2016; Cabanas-Valdes et al., 2016; Haruyama et al., 2017; Karthikbabu et al., 2011; Kumar et al., 2012; Saeys et al., 2012; Verheyden et al., 2009) presented the results of balance evaluations after training using quantitative scales. Although improvement in performance was observed in both intervention and control groups, the results were superior in the treatment group in six studies (Buüyuükavcı et al., 2016; Cabanas-Valdes et al., 2016; Haruyama et al., 2017; Karthikbabu et al., 2011; Kumar et al., 2012; Saeys et al., 2012). In a specific publication (Verheyden et al., 2009), a difference was observed only for the TIS sitting dynamic subscale.
A meta-analysis was performed for three studies that assessed balance using the BBA (Fig. 3A). It included 125 participants, of which 65 were randomized to the treatment group and 64 to the control group. There was also a significant improvement effect on balance with a pooled increase in BBA score of 2.7 points from the baseline (p < 0.0001). A substantial level of statistical heterogeneity was noted (81%) in relation to the dispersion of values of mean differences and confidence intervals.
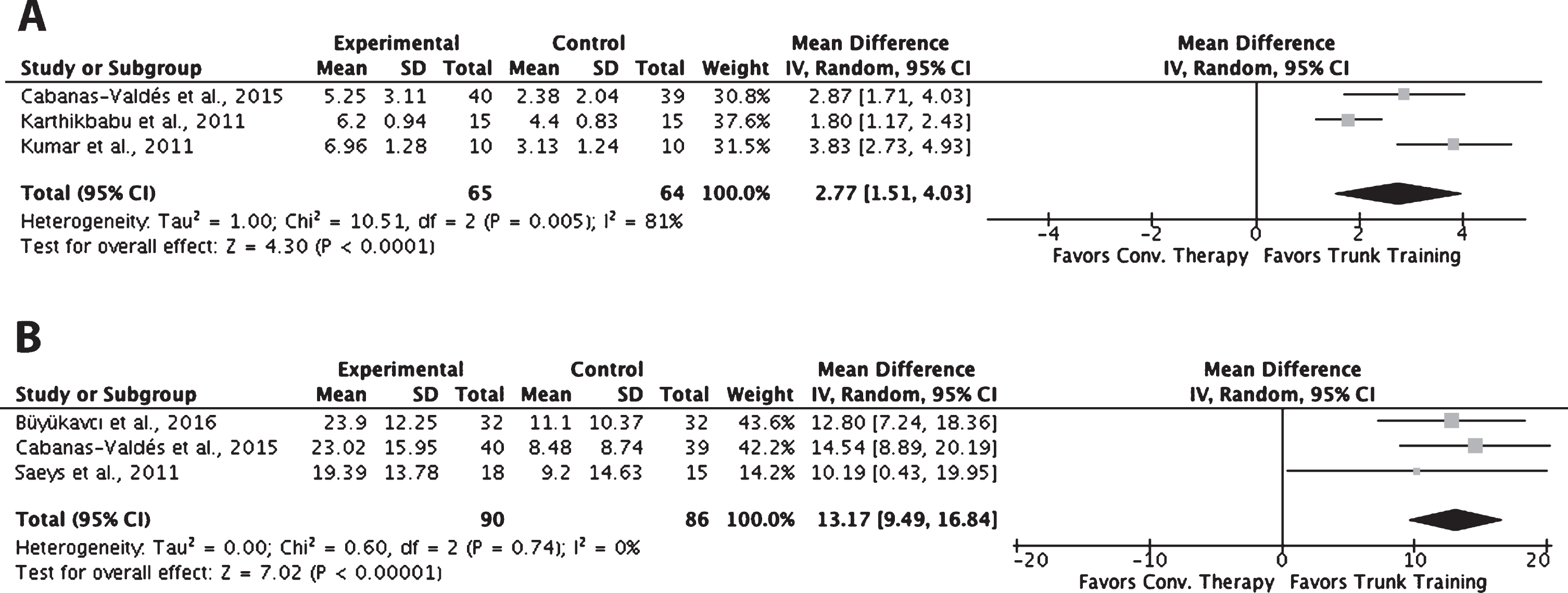
Forest plot of the meta-analysis from randomized clinical trials on the effect of trunk exercises on the Brunel Balance Assessment (A) and the Berg Balance Scale (B) scores.
The BBS was used for balance assessment in three studies. Figure 3B shows the meta-analysis of their results with a highly significant pooled increase of 13.17 points from the baseline (p < 0.00001). The analysis included 176 participants, of which 90 were randomized to the treatment group and 86 to the control group.
Four studies evaluated weight transfer. In three (Buüyuükavcı et al., 2016; Cabanas-Valdes et al., 2016; Fujino et al., 2016; Howe et al., 2005), the inclusion of a protocol specific for trunk rehabilitation in the hospital environment was associated with a significant improvement in the ability to transfer the trunk laterally. Howe et al. did not observe a significant difference in this parameter; however, there was improvement in the oscillation during static positioning and reduction of the time needed to return to the original position (Howe et al., 2005).
In this meta-analysis, we addressed the impact of inpatient trunk exercises after recent stroke. The results showed that such a measure contributes to the medium-term rehabilitation of stroke victims, especially in relation to trunk control and balance; the outcomes observed being superior to those obtained with traditional techniques. To the best of our knowledge, this is the first meta-analysis dedicated to inpatient trunk training and associated impact on specific and homogenous clinical scales, which seems to bring some clarification to the effectiveness of this type of additional exercise.
In a previous meta-analysis that assessed the general results (Sorinola et al., 2014) of six randomized clinical trials, moderate evidence was observed to suggest that the addition of trunk exercises could facilitate improvement in standing balance and walking ability, but not in trunk control. Nevertheless, the improvement in balance and trunk performance in this study is very significant. The most probable explanation for the disagreement relies on the fact that the two studies did not analyze the same outcomes. In the present one, only researches using the same instrument (TIS, BBA, and BBS) for a given performance assessment were included in each analysis. This criterion may have provided more homogeneity to the pooled examination, even though its conclusions had to be limited to the considered scales. In addition, the present study focused on in-patient treatment and more clinical trials have become available since that time.
Trunk control is the ability of the trunk muscles to allow the body to remain vertically upright, adjust weight shifts, and perform selective movements, maintaining the support base during static and dynamic postural adjustments (Karthikbabu et al., 2011). Several studies report the relevance of this for the functional performance after stroke. The ability to remain seated vertically is a prerequisite for performing head and upper limb movements, and consequently has considerable influence over the individual’s ability to perform the activities of daily living (Di Monaco, Trucco, Di Monaco, Tappero, & Cavanna, 2010; Karatas et al., 2004).
One of the domains in which the effect of trunk training was most evident was balance. The benefits concerned both static and dynamic balance in sitting and standing positions, which are important for functional performance and quality of life after stroke. It may be assumed that this gain is related to the fact that the therapy enhances the recovery of the muscular strength necessary to raise the pelvis, rotate the upper part of the trunk or control the shoulder girdle. Thus, a given patient may reach a better condition to achieve trunk stability, perform anticipatory postural adjustments, and work against resistance (Karthikbabu et al., 2011; Kumar et al., 2012; Saeys et al., 2012; Verheyden et al., 2009).
A less homogeneous result was observed for weight-transfer capacity. In three studies, significant benefits were reported, and one study found no significant gain relative to the control group. In the latter case, intra-group improvement was observed in both balance and posture (Howe et al., 2005).
The results summarized in this study reinforce the benefits of performing specific trunk training in the relatively early post-stroke phase. Considering that trunk stability is a core component of balance, coordination, and performance of daily activities, it is possible that such gains have a considerable medium-term impact on tasks not directly related to the trunk and that they help reducing the risk of clinical complications associated to prolonged bed rest, hypotheses that may be targeted by future research. A major limitation for current and future research is the difficulty to blind participants and practitioners during physical therapy.
Conclusion
Trunk control, balance, and weight transfer ability are basic motor skills crucial for the performance of various tasks and independence. The results of this study show that the introduction of trunk-based inpatient training protocols brings short-term benefits in these three domains. A meta-analysis of randomized clinical trials reveals significant improvement on the Trunk Impairment Scale, Brunel Balance Assessment scale, and Berg Balance Scale after the application of inpatient trunk exercises for stroke.
Conflict of interest
None to report.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.