
Abstract
BACKGROUND:
Pediatric acquired brain injury may result in a significant gap between the “pre” and “post-injury” child.
OBJECTIVE:
We aimed to quantitatively explore the mechanism underlying parents’ loss experience by examining the mediating role of behavioral outcomes (observed-problems and perceived-change) in the relationship between injury severity and grief.
METHOD:
The study employed a cross-sectional retrospective design and comprised 40 parents of children (aged 3–18 years) with moderate-severe brain injury. Data for each parent included an adapted version of the Two-Track Bereavement Questionnaire and Socio-demographics; Data for each child included the child’s Information Processing Speed Index; the Child Behavioral Checklist and Parental Perception of Behavioral Changes scale.
RESULTS:
Slowed information processing speed was significantly associated with elevated ratings on both measures of behavioral outcomes and with intensified grief. Mediation analyses revealed that parental perceived behavioral change, significantly mediate the relationship between information processing speed and grief; the Child Behavioral Checklist total score also mediated the same relationship but only in 90% confidence interval.
CONCLUSIONS:
Findings reveal the adverse impact of behavioral outcomes on grief and suggest parents’ loss experience to be stemming primarily from their subjective perception over their “changed-child”, rather than the observed problems. Implications for clinical practice are discussed.
Introduction
It is well known that children and adolescents who sustained moderate to severe brain injury experience significant disruptions in various domains of functioning which result in permanent deficits (see Beauchamp & Anderson, 2013). In light of the associated neurobehavioral outcomes, the family may struggle to accept the changes and the loss of the former child and experience intense grief (Clark, Stedmon, & Margison, 2008; Jantz, Comerchero, Canto, & Pierson, 2015). The present work attempts to trace the underlying mechanism affecting parental grief reaction (PGR) by examining its interplay with a cognitive measure of injury-severity and measures of behavioral outcomes (BO).
BO following pediatric acquired brain injury (pediatric-ABI) are of common occurrence and oftentimes lead to pronounced modifications in the child’s nature and personality (Max et al., 2015; Middleton, 2001). These may be evident in behaviors directed outward or inward which are oftentimes classified as ‘externalizing’ and ‘internalizing’ problems, respectively (see Li & Liu, 2013 for review). The extent of BO was reported to correlate with the severity of injury (Catroppa, Anderson & Rosenfeld, 2008; Max, 2005). Accordingly, the cognitive impairments associated with such injuries (Lezak, Howieson, Bigler, & Tranel, 2012; Kirkham, 2017) were also reported to correlate with behavioral changes (Max et al., 2015), secondary to deficits in executive functions, attention, and information processing speed (IPS) which are assumed to underlie behavior (Schultz et al., 2016; Miyake et al., 2000). Specifically, IPS was consistently validated as a robust cognitive marker of injury-severity due to its high susceptibility to disruption following a neurological insult (Gorman et al., 2016; Prigatano, & Gray, 2008; Hillary et al., 2010).
With notable consistency, the severity of BO post injury was associated with the family’s long-term adaptation (J’May et al., 1993; Schwartz et al., 2003; Stancin, Wade, Walz, Yeates, & Taylor, 2008). To date, the impact of BO on parents was quantitatively demonstrated mainly in relations to distress, burden and coping via obtaining parental perspective on standardized measures of observed behavioral problems (e.g., Child Behavioral Checklist -Anderson et al., 2006; Prigatano, & Gray, 2007; The Vinland Adaptive Behavior Scale – II - Micklewright, et al., 2012). Conversely, only one study showed such relationship between BO and grief (Zinner, Ball, Stutts, & Philput, 1997) by using a modified version of the Neurobehavioral Rating Scale and reporting severe grief among mothers who rated their children as having poor neurobehavioral functioning.
Qualitative studies further elucidate the distress and burden parents experience due to the need to manage the child’s BO alongside their derivatives (e.g., increased dependency, social isolation, the need to assume semi-professional skills). However, these studies also elucidated the great sense of loss parents experience given the need to adapt to the BO and become a “different parent to a different child” (see Tyerman, Eccles, & Gray, 2017 for review). Accordingly, parents reported that their relationship with the child has changed dramatically and that they continuously grieve over the child they had known (e.g., Roscigno & Swanson, 2011; Jordan & Linden, 2013).
Despite these articulations, parents’ perspective over the “changed-child” received almost no empirical attention in the literature and remained under-represented. We believe that in the context of parental grief both perspectives of “observed problems” and “perceived change” should be examined. It may be that parental ratings of BO on standardized measures may not necessarily represent a “clinical problem” but may still represent a “change” that elicit a strong sense of loss and vice-versa. Such exploration may also help to target psychotherapeutic interventions geared to promote family adaptation within the rehabilitation setting.
As the current study aimed to explore the impact of behavioral outcomes in the context of grief, we examined the mediating role of both BO perspectives in the relationship between injury severity and PGR. To this end, our investigation incorporated the following components: 1) IPS, as an objective cognitive-measure of brain injury-severity. 2) parental ratings of observed problems on the Child’s Behavioral Checklist (CBCL), alongside ratings on a scale designed to assess parental perception of behavioral changes (PPBC); and 3) an adapted version of the ‘Two – Track Bereavement Questionnaire’ as a measure of parental grief reaction (PGR). This study holds the assumption that more severe cognitive impairment will be associated with more severe behavioral outcomes and will lead to greater PGR. Therefore, we hypothesized that elevated parental ratings on both CBCL and PPBC will mediate the relationship between IPS and PGR.
Method
Design and procedure
The study employed a cross-sectional retrospective design. Data concerning parents’ total grief scores, socio-demographics and ratings on the PPBC was obtained from a larger data set of a broad research project on PGR following pediatric-ABI, conducted between the years 2014–2018. Data concerning the child’s demographics and injury related information was obtained from the medical file and archival neuropsychological evaluation (i.e., IPS score, parental ratings on the CBCL summary indexes) conducted between the years 2009–2018. The study took place at a Pediatric Rehabilitation Department (Brain Injury Clinic) at a hospital in central Israel and was approved by institutional review boards of the participating medical institution (protocol number: SMC-1568-14) and the academic institution (approval number: 2015033). All study measures were administered at least a year after the brain injury occurred.
Participants
The sample included 40 parents of children who had sustained moderate to severe ABI between 3 – 18 years of age. Severe traumatic brain injury (TBI) was defined based on lowest post-resuscitation GCS score of≤8 (N = 24), and moderate TBI was defined as a GCS score 9 < 12 (N = 1); Stroke, Tumors and Brain Disease’s severities were based on visible trauma-related intra-cranial findings on neuroimaging; all children underwent a prolonged (at least three months) hospitalization following the injury event and underwent a neuropsychological assessment at follow-up. All children developed normally until the injury event with no history of prior brain injury, severe chronic physical or psychiatric illness. Sample characteristics are presented in Table 1.
Sample characteristics
Sample characteristics
Note. GCS = Glasgow Coma Scale.
Sociodemographic and injury related variables were collected from parents’ sociodemographic questionnaire and review of medical records.
An adapted version of The Two-Track Bereavement Questionnaire (TTBQ) (Rubin et al., 2009) is a questionnaire of 70 self-reported items designed to assess one’s response and adjustment to loss over time, on a 5- point scale. It was developed in accordance with the Two-Track Model of Bereavement (Rubin, 1999), which conceptualizes the response to the loss through two tracks: Track I relates to the biopsychosocial functioning of the bereaved, and Track II focuses on the bereaved’s continuing relationship with the deceased. A higher score indicates greater complexity and more hardship with regard to the bereavement process. Questionnaire was adapted to fit loss following injury rather than death. For the current study only the TTBQ total score was obtained. The internal consistency of full original TTBQ (general score) was found as 0.94 (Rubin et al., 2009). In the current study the Cronbach’s alpha of the general score is α= 0.91.
Information processing speed (IPS) Index (WAIS-III/WISC-IV -Wechsler, 2003, 2008). All IPS index scores were converted into Z scores in order to enable comparison between different IPS tests that were used, due to child’s age at evaluation.
Parental Perception of Behavioural Changes (PPBC); a single item scale designed to assess parents’ subjective perception of behavioral changes in their child following the injury. The scale was stated as followed: “Were there any behavioral changes in your child following the injury? If so, please rate the intensity of these changes: from 1 (minor or unnoticeable) to 5 (prominent and fundamental changes).
The Child behavior checklist (CBCL): (Achenbach, 1991): a 113-item caregiver-report used to evaluate a child’s emotional and behavioral status. Raters score each item on a 3-point scale: 0 =’not true’, 1 =’somewhat or sometimes true’ and 2 =’very true or often true’ for the past 6 months. According to the CBCL scoring system, raw scores are converted into T-scores (M = 50, SD = 10), with higher scores reflecting more pathology. The present study used the Internalizing summary score (The Anxious/ Depressed, Withdrawn/ Depressed and Somatic Complaints scales); Externalizing summary score (i.e., Rule-Breaking Behavior; Aggressive Behavior) and the Total summary score which include three additional scales (Social Problems, Thought Problems and Attention Problems). Scores in those scales range from Normal (T < 60), Clinical Band (T = 60–63) and Clinical (T > 64). There is extensive research evidence supporting the reliability, validity and clinical utility of the CBCL (Achenbach & Rescorla, 2001). The checklist has been translated into 26 languages, including Hebrew (Zilber, Auerbach & Lerner, 1994).
Statistical analysis
First, data were analyzed for missing data. Little’s MCAR test (Little, 1988) was non-significant [χ2(14) = 18.21, p = 0.197], indicating that data were missing completely at random. Then, multiple imputation technique (one-time stochastic regression) was used to handle the missing data, which was lower than 4% for all values. Correlations between background variables and TTBQ were analyzed using Pearson correlation for continuous variables and point biserial for dichotomous variables. Mann-Whitney U test and t test were used to check for order effect. Associations between study variables were tested via Pearson correlation. Lastly, mediation analyses were conducted using the PROCESS macro for SPSS, model 4 (Hayes, 2018). Percentile confidence intervals (CI) were estimated for the indirect effects based on 5,000 bootstrap samples of the data. To have significant indirect effect, the CIs must not include zero (Shrout & Bolger, 2002). All data were analyzed using SPSS 25, and all tests performed were two-tailed with α set at 0.05, except for correlations between study variables, which were analyzed one-tailed.
Results
First we ruled out any possible effect of the background variables on the dependent variable. No significant associations were found between TTBQ score and parents’ characteristics: Gender (r pb = 03, p = 0.82), Age (r = 0.20, p = 0.20), Education (r =–0.02, p = 0.85). Furthermore, no significant association was found between parental TTBQ scores and each of the child’s characteristics: Age at injury (r = 0.21, p = 0.17), Time since injury (r =–0.04, p = 0.78) and Age at assessment (r = 0.16, p = 0.30).
Further, because some parents (n = 7) completed the TTBQ questionnaire one year prior to their child’s neuropsychological-assessment and others at the same year (n = 23) or afterward (n = 10), it was necessary to rule out possible time-order-effect on the dependent variable. A Mann-Whitney U test indicated no significant differences in TTBQ scores between the two order groups: ‘grief-assessment’ (n = 7; Md = 2.92, SD = 0.46) vs. ‘assessment-grief’ (n = 33; Md = 2.92, SD = 0.46), U = 111.5, p = 0.887. A similar result was obtained when using independent sample t-test [t(38) =0.26 p = 0.79]. The latter ascertain that for those parents in the ‘assessment-grief’ group, the interval between the time they were asked to report behavioral problems on the CBCL and the time they were given the TTBQ questionnaire was not associated with elevation in grief score, hence indicating no deterioration in the child behavioral problems.
Descriptive statistics and zero-order correlations between the study variables are presented in Table 2.
Means, standard deviations and zero-order correlations (one-tailed) between the study
Means, standard deviations and zero-order correlations (one-tailed) between the study
Note. N = 40. TTBQ = Two-Track Bereavement Questionnaire; IPS = Information Processing Speed; CBCL = Child Behavior CheckList; INT = Internalizing; EXT = Externalizing; PPBC = Parental Perception of Behavioral Changes. *p < 0.05 **p < 0.01 ***p < 0.001 +Marginally significant (p < 0.10).
As can be seen in Table 2, TTBQ score was negatively correlated with IPS score and positively correlated with all three CBCL summary scores and with PPBC score, though the correlation with CBCL Total summary score and Externalizing summary score was only marginally significant. IPS was negatively correlated with all three CBCL summary scores and with PPBC score, though the correlation with CBCL Internalizing summary score was only marginally significant. Lastly, no correlation was obtained between CBCL and PPBC scores.
To test the mediating role of behavioral outcomes in the relationship between injury-severity and grief a mediation analysis was conducted. In the tested model, IPS served as the independent variable, CBCL total score and PPBC as parallel mediators and TTBQ total score as the dependent variable. The mediation analysis showed that the path between IPS and CBCL was statistically significant, as was the path between CBCL and TTBQ. Similarly, the path between IPS and PPBC was statistically significant, as was the path between PPBC and TTBQ. The significant total effect of IPS on TTBQ was reduced to non-significance in the direct model (see Fig. 1). Bootstrapping for the indirect effects showed significant results for the total indirect effect [B =–0.19, SE = 0.06, 95% CI: –0.34, –0.09] as well as for PPBC [B =–0.15, SE = 0.05, 95% CI: –0.27, –0.06], but not for CBCL [B =–0.04, SE = 0.03, 95% CI: –0.10,0.003]. A comparison between the strength of both indirect effects yielded a significant result [B = 0.11, SE = 0.06, 95% CI:0.10,0.23]. Note, that the indirect effect of CBCL was significant within a 90% CI [B =–0.04, SE = 0.03, 90% CI: –0.10,0.003]. Lastly, approximately 47% of the variance in TTBQ was accounted for by the predictors of the overall model [F(3, 36) = 10.77, p < 0.001, R2 = 0.47].
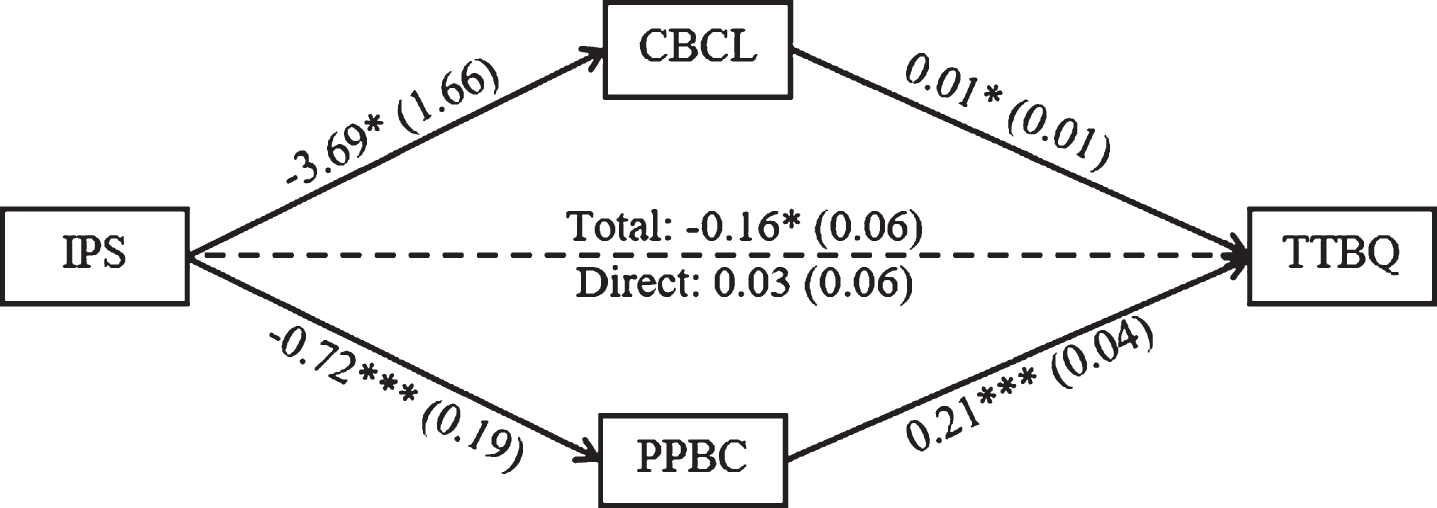
Mediation model of the relationship between IPS and TTBQ as mediated by CBCL and PPBC. Values are unstandardized regression coefficients. In parentheses: standard errors. Solid lines indicate significant paths and dashed lines indicate nonsignificant paths. TTBQ = Two-Track Bereavement Questionnaire; IPS = Information Processing Speed; CBCL = Child Behavior CheckList; PPBC = Parental Perception of Behavioral Changes. *p < 0.05 ***p < 0.001.
The present study aimed to shed light on some underpinnings of PGR following moderate-severe pediatric – ABI by using a quantitative method. Specifically, we explored whether PGR is correlated with the child’s injury severity, with parental ratings of observed problems and/or with parental ratings of perceived-change. In general, our finding indicated IPS as a predictive marker for intensified PGR and revealed the adverse impact of BO, primarily perceived-change, on parents’ living-loss experience.
Objective injury severity and BO
IPS was predictive of the child’s BO. Specifically, slowed information processing speed was associated with more observed problems especially on the Externalizing and CBCL-total summary scores. This finding corroborates with previous studies which identified IPS problems after pediatric-TBI to be strongly related to personality changes in children between 5–14 years of age (Max et al., 2015); to poor social problem solving skills in very young children (Walz, Yeates, Wade & Mark, 2009); to impaired socioemotional functioning (Tonks et al., 2011) and social participation (Schultz et al., 2016). Of a particular interest is the strong significant correlation found between IPS and PPBC. While the latter perspective was newly explored in the current study, this correlation indicates parental subjective perception over the “changed child” to be sensitive to the objective severity of the child’s brain impairment.
Observed problems vs. perceived change
Despite the aforementioned correlation between objective injury severity and both perspectives of BO, no relationship was found between any of the CBCL summary scores and the PPBC. This finding potentially suggest that parental ratings on the CBCL may be more reflective of the child’s current state post-injury rather than grasping changes in the child’s behavioral manifestation. Thus, as ratings on the CBCL (1-year post injury at minimum) can either reflect no behavioral change, a newfound behavioral problem, or exacerbation of the child’s pre-injury characteristics or developmental trajectory (Cattelani, Lombardi, Brianti & Mazzucchi, 1998; Schwartz et al., 2003; Max et al., 2006) they may not correspond with the parents’ perceived change. Additionally, it should be noted that despite reports on pronounced neurobehavioral changes after pediatric-ABI in the literature, most parental ratings on the CBCL in previous studies were classified as “normal” and did not meet the clinical cut-off among severely injured children (e.g., Hayman-Abello, Rourke & Fuerst, 2003; Wetherington, Hooper, Keenan, Nocera & Runyan, 2009; Silberg, Tal-Jacobi, Levav, Brezner, & Rassovsky, 2015). Similarly, in the current study, the majority of children (75%) did not meet the clinical cut-off in any of the CBCL summary indexes. Therefore, this lack of association between measures of “observed-problems” and “perceived-change” strengthen the significance of parents’ subjective perception of the gap between the “pre” and “post” injury child.
Collectively, this finding perhaps bolster the shortcomings of most standardized assessment tools when utilized at a post-injury state. Further, it is alluding to a clinical problem as parents are instructed to rate the child’s behavioral state irrespective of his pre-injury functioning, or his expected developmental trajectories had the injury not occurred. Therefore, we believe that this important, albeit preliminary direction, should be further pursued in future studies.
Behavioral outcomes – grief
Regression analysis indicated elevated parental ratings on the CBCL to be predictive of intensified PGR (especially Internalizing problems as was evident at the level of zero order correlations). While there are inconsistent reports on internalizing and externalizing problems after pediatric – ABI, even at the same age group (Anderson et al., 2005; Chapman et al., 2010), the persistence of overall behavioral problems (Yeates & Taylor, 2006) was noted. However, only Zinner et al., (1997) reported that behavioral problems, especially of the unconstrained type (e.g., social disinhibition, poor insight) in adolescence and early adulthood, highly impacted mothers’ grief. Other problems such as cognitive understanding, verbal expression and physical mobility had a very low impact on grief, hence, consistent with our major finding.
In addition to the CBCL, elevated ratings on the PPBC scale also predicted grief. However, analysis of the mediation model indicated that only PPBC mediated the relationship between injury-severity and grief, while CBCL also mediated this relationship but at 90% confidence interval.
Thus, our finding strongly points to the significant role that parent’s subjective perceived-change play in the context of grief. Such mediation may confirm the assumption that parents do not respond to the injury-severity itself but to its “phenotype” – i.e., to its behavioral manifestation. Moreover, it is suggested that rather than the severity of the observed behavioral problems per-se, it is parents’ appraisals of what the child has become vs. what he will not achieve, that substantially contribute to their loss experience.
Coupled with the loss of dreams parents may have hold for their child, such appraisals may well exacerbate over time as the child mature and parents are left to face the painful aspects of these BO such as social alienations and reduction in social activities (Jordan & Linden, 2013; Tyerman et al., 2017; Catroppa et al., 2015). Furthermore, as most children exhibit impaired self-awareness due to cognitive deficits, emotional or normative age-related factors, parents may hold this experience of loss also for their child who is not fully able to grasp his condition and its future consequences (Collings, 2007).
Clinical Implications
Our findings suggest that clinical work with parents should be targeted to address PPBC, and focus on the way parents perceive the child’s condition and the associated loss and on the way they bridge the gap between observed manifestations vs. expected life trajectory. As parents’ subjective perception may affect grief and visa-versa, putting emphasis on parents’ subjective appraisals may not only mitigate their grief but may also mitigate the child’s reported outcome. The latter proposition accords with several studies which argued for parent-child mutual influence on behavior, and that parents distress can aggravate the child’s behavioral outcome (Taylor et al., 2001; Micklewright et al., 2012; Wade et al., 2011; Brown et al., 2014; Kinsella, Ong, Murtagh, Prior & Sawyer, 1999).
Limitations and future direction
Limitations of the current study have to do primarily with its retrospective design. For some children data concerning neuropsychological evaluation and parental grief were undertaken at two different points of time-order. Although scores on the CBCL were proven to be stable over-time (Mattison & Spitznagel, 1999; Biederman et al, 2001), ideally all study measures should have been taken at the same point in time. Our findings should be further explored on an even larger sample of children and parents to enable their generalization. As previous studies on behavioral outcome were conducted on children who sustained Traumatic Brain Injury (TBI) it is suggested that other forms of acquired brain impairment will be studied. Lastly, it is suggested that future studies and clinical practice will promote the development and incorporation of standardized measures assessing the child behavioral manifestations both pre-injury and post- injury.
Conflct of interest
The authors report no conflict of interest.