
Abstract
BACKGROUND:
Physical exercise combined with occupational therapy (OT) can lead to a global improvement in personal well-being.
OBJECTIVE:
To assess in PD patients: 1) if a rehabilitation program involving OT, Nordic walking (NW) and therapeutic touch (TT) yields motor/non-motor benefits; 2) if the time collocation of OT within the program influences results.
METHODS:
This is a pilot study on 17 PD patients undergoing a 10-week rehabilitation program consisting of OT, NW and TT. Patients were randomized to receive OT in the first [Group 1, n = 8] vs. last five weeks [Group 2, n = 9] of the program. Scales (MMSE, FAB, BDI, UPDRS II and III, PDQ39 and AES-S) and 6MWT, Gait speed and length were assessed at three time-points.
RESULTS:
Thirteen out of 17 patients were analyzed. 6MWT, Gait speed and length improved in time without between-group differences (p < 0.05) as did UPDRII, UPDRSIII, FAB and PDQ39 (p < 0.05). Baseline UPDRS II and III significantly determined Δ6MWT (adjusted R2 = 0.6738) and ΔGAIT speed (R2 = 0.6746) at multiple regression, while ΔGAIT length showed the best regression (adjusted R2 = 0.8247) with impact of age, gender and baseline PDQ39 (ADL and cognition dimensions).
CONCLUSIONS:
Multidisciplinary rehabilitation including OT can improve motor and non-motor conditions in PD patients. The OT time-collocation at beginning or end of the rehabilitation program does not significantly affect results.
Keywords
Introduction
Parkinson’s disease (PD) is a common neurodegenerative disorder with increasing prevalence due to population aging. PD is characterized by both motor and non-motor symptoms and, while the main treatment is pharmacological, non-pharmacological interventions are a vital part of the multidisciplinary approach to the disorder (Cusso, Donald, & Khoo, 2016; Ferrazzoli et al., 2018; van der Marck et al., 2009). Among non-motor symptoms, of great importance are psychological symptoms, present in 70% of patients (Aarsland et al., 1999; Starkstein et al., 2009). The most frequent is depression, estimated in about 40% (Cummings, 1992). Overlapping with depression are anhedonia and apathy (Leentjens et al., 2008; Marin, 1991; Starkstein, 2012; Starkstein et al., 2009). PD patients, in fact, are generally depressed, incapable of experiencing pleasure, have a poor quality of life (Pedersen, Larsen, Alves, & Aarsland, 2009) and show a “quantitative reduction of self-generated voluntary and purposeful behaviors” directly correlated to the increasing motor and cognitive problems (Levy & Dubois, 2006).
Motor and non-motor symptoms are closely inter-related. Working on the cognitive area or, vice versa, on motor status inevitably benefits the other sphere (Alves Da Rocha, McClelland, & Morris, 2015; Cusso et al., 2016; Morberg, Jensen, Bode, & Wermuth, 2014), promoting a global improvement of the patient’s wellbeing (Abbruzzese, Marchese, Avanzino, & Pelosin, 2016; Carne et al., 2005; Post, van der Eijk, Munneke, & Bloem, 2011; Radder et al., 2017). Not only drugs but also complementary therapies such as physical exercise and occupational, speech, and music therapy are useful (Subramanian, 2017). In this pilot study evaluating a combination of interventions in PD, we selected Nordic walking (NW), Occupational therapy (OT and Therapeutic touch (TT). Several reports show the beneficial effect of NW and OT in PD on both motor symptoms (Bang & Shin, 2017; Ellis et al., 2008; Warlop et al., 2017) and quality of life (Clarke et al., 2009; Reuter et al., 2011).
NW provides a safe and effective way to enhance physical activity in the elderly (Skorkowska-Telichowska et al., 2016). In PD, recent clinical trials and systematic reviews documented the effectiveness of treadmill walking and NW in improving gait speed and other walking capacity parameters (Alwardat, 2018; Bang & Shin, 2017; Fritz et al., 2011; Herman, Giladi, & Hausdorff, 2009; Monteiro et al., 2017). OT focuses primarily on supporting participation in daily life through manual and voluntary repeated activities. It helps patients to express their emotions, abilities and resources and improve their quality of life. OT acts mainly on the neuropsychological aspect of PD and its potential role is recognized in multidisciplinary guidelines (Grimes et al., 2012; Stewart, 2007). Moderate to strong evidence exists supporting the use of OT in PD (Arbesman, Lieberman, & Metzler, 2014; Clarke et al., 2009; Ellis et al., 2008; Foster, 2014; Parkinson et al., 2014; Saint-Hilaire, 2014; Sturkenboom et al., 2014).
We added TT to OT and NW because it helps the patient attain a state of well-being through mental and physical relaxation (Monroe, 2009; Newshan & Schuller-Civitella, 2003; Senderovich et al., 2016). We inserted the first two phases of the Kreme Technique in our program because they are simple to learn and execute. Our study aimed to: 1) evaluate if a multidisciplinary rehabilitation program of ten weeks including OT, NW and TT can induce modifications particularly in non-motor areas such as depression, anhedonia and quality of daily life; 2) compare two different temporal collocations of OT within the rehabilitation program: in the first vs. last 5 weeks. The hypothesis was that OT at the beginning of the program might create a “social group” with a consequent positive effect on treatment outcomes (particularly in the non-motor area).
Material and methods
Study design
This was a pilot study on 17 patients affected by idiopathic PD on stable therapy (L-dopa and dopaminergic drugs) admitted for outpatient rehabilitation at the XXX between 2006 and 2007. Inclusion criteria were: history of PD for at least 5 years, age 55– 75 years, and Hoehn & Yahr score <2.5. Patients with presence of essential tremors were excluded.
Patients were randomized into two groups: Group 1 (n = 8) received OT in addition to physical exercise in the first five weeks of the 10-week rehabilitation program, Group 2 (n = 9) received OT in addition to physical exercise in the last five weeks of the rehabilitation program. Due to incomplete data in Group 2, the number of patients analyzed was reduced from 9 to 5 (for details see Flow chart, Fig. 1). Three time points were analyzed: at entry (T0), 5 weeks (T1), and 10 weeks (T2). T1 was the midpoint, to allow between-group comparison of non-motor factors.
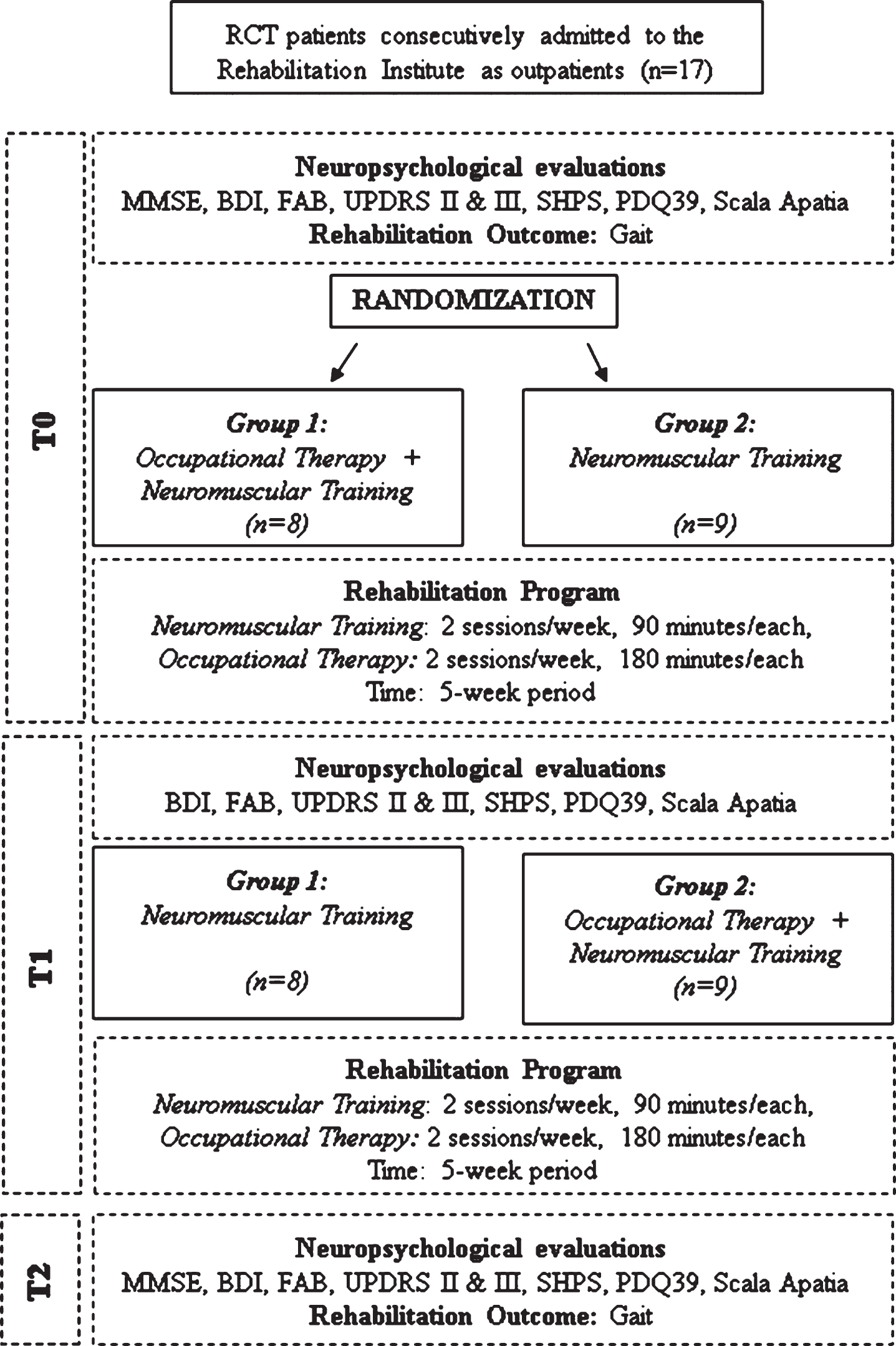
Flow chart of the study.
The exercise program, for both groups, consisted of two 90-min sessions of NW per week for a total of 3 hours/week, 1 session/week of standard exercises and 1 day per week of TT. OT consisted of two 3-hour sessions per week (Fig. 1). In addition to usual OT aimed at improving ADLs, time was spent also in group activities (card games, checkers) and individual recreational activities, e.g. reading, embroidery, writing, creating objects with various materials (modeling clay, salt dough), painting, collage, puzzles. Patients could choose whatever activity they preferred.
The study was approved by the XXXXX, Local Review Board (Technical and Scientific Committee) and Ethical Commettee (XXXXCE). Patients gave their written informed consent for use of their clinical data for scientific purposes.
Sociodemographic and anthropometric data, including age, gender and education level, were collected at baseline (T0). Both groups were administered motor/non-motor assessment scales and motor capacity tests at T0 and T2. At T1, only the scales indicated in the study design were evaluated.
Motor/non-motor assessment scales
Depression, apathy, anhedonia and quality of life were investigated with specific scales by a neuropsychologist and neurologist, as follows:
Patients completed all scales in dopaminergic “ON” state.
Motor performance
NW was performed on a Gait Trainer (Hesse & Uhlenbrock, 2000). The Gait Trainer used in this study (BIODEX, Gait trainer 2, New York, USA) is connected to a computer treadmill that records/stores walking parameters (in relation to the physiological reference values adjusted for gender, age and height). The following parameters were analyzed: mean walking velocity (GAIT speed) (Herfurth et al., 2015); step length (GAIT length) (Herfurth et al., 2015); 6-min walking test (6MWT), a measure of walking capacity, i.e. meters walked in 6 minutes (Picelli et al., 2012).
Statistical analysis
All data were expressed as mean±SD or delta changes (absolute values for delta T2-T0 and delta T1-T0). All data were evaluated for Gaussian distribution (Shapiro-Wilk test) before statistical analysis using the Graph Pad Software (Prism 4) and the R (R-Core-Team, 2017). Depending on the results, we used Student’s t test or Wilcoxon test for comparison between groups and absolute delta. Groups and times were compared with two-way ANOVA. When significant, Holm-Bonferroni post-hoc test was used to confirm differences between groups. We also evaluated the effect size, i.e. the degree of relationship between dependent and independent variables, independently of the sample size. Values of 0.01– 0.02 indicate a trivial effect, 0.03– 0.05 small effect, 0.06– 0.13 medium effect; and 0.14– 0.20 large effect according to thresholds proposed by Cohen (Cohen, 1988). Multiple regression analysis investigated relations between independent variables such as demographic parameters (gender, age), groups, assessment scales at T0 and the absolute delta T0-T2 for motor performance as the dependent variable. A p value <0.05 was considered as statistically significant.
Results
Table 1 shows demographic characteristics and all evaluations performed at entry (T0) for the two groups. No significant differences were found between Group 1 and Group 2. Tables 2 and 3 report two-way mixed ANOVA results for the assessment scales (2 groups, 3 times) and motor performance tests (2 groups, 2 times). Only ANOVA significant evaluations for Time and/or Group and/or Interaction Time*Group are reported. In general, there was no influence of Group on non-motor or motor evaluations.
Demographic characteristics and assessments of patients at baseline (T0, n = 17 patients)
Demographic characteristics and assessments of patients at baseline (T0, n = 17 patients)
Legend: MMSE: Mini-Mental State Examination, UPRDS2 and 3: Unified Parkinson’s Disease Rating Scale II and III, FAB: Frontal Assessment battery, Total PDQ 39: Quality of Life Scale for PD summary standardized index, BDI: Beck Depression Inventory, AES-S: Apathy Evaluation Scale, self-rated version, 6MWT: 6-min walking test, GAIT Trainer speed and length: mean walking velocity and step length.
Regarding the assessment scales, only Time was significant for UPDRII, UPDRSIII, FAB and PDQ39 summary index, with a large effect size for all (Table 2). PDQ39 significance was influenced by the PDQ39 ADL (Time: p = 0.03) and communication (Time: p = 0.007) dimensions.
Two-way Mixed ANOVA and Effect size for UPDRSII, UPDRSIII, FAB, PDQ39 in the 2 groups. Three time-points (T0, T1 and T2) were evaluated in 13 patients with complete data
Legend: Effect size indicates trivial effect for 0.01– 0.02, small effect for 0.03– 0.05, medium effect for 0.06– 0.13; and large effect for 0.14– 0.20 according to thresholds proposed by Cohen [Cohen, J. Statistical power analysis or the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum, 1988].
The motor performance tests confirmed a significant ANOVA for Time with a large effect size (Table 3) for all three parameters: 6MWT, GAIT speed and GAIT length.
Two-way Mixed ANOVA and Effect size for 6MWT, GAIT speed and length in the 2 groups. Two time-points (T0 and T2) were evaluated in 13 patients with complete data.
Legend: Effect size indicates trivial effect for 0.01– 0.02, small effect for 0.03– 0.05, medium effect for 0.06– 0.13; and large effect for 0.14– 0.20 according to thresholds proposed by Cohen [Cohen, J. Statistical power analysis or the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum, 1988].
Absolute delta T2-T0 and, for the assessment scales only, delta T1-T0 results are reported in Table 4 and Fig. 2 (Fig. 2). Multivariate regression analysis on absolute delta T2-T0 for 6MWT, GAIT speed and GAIT length as Dependent Variables is presented in Table 4. Gender emerged as a common independent determinant in all three regressions (but was significant only in GAIT length), with an increase of delta in males with respect to female. UPDRS II and UPDRS III at baseline resulted as significant determinants of 6MWT and GAIT speed with different sign impact on delta (positive for UPDRSIII and negative for UPDRSII). GAIT length showed the best regression with a negative impact of age, PDQ39 ADL and cognition domains.
Multivariate regression analysis on absolute delta T0-T2 for 6MWT, GAIT speed and length as dependent variables (n = 13 patients with complete data).
Legend: Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1. For the three different regressions, Gaussian distribution of residuals has been checked and confirmed.
Figure 2 shows comparisons between the two groups for absolute delta T1-T0 and delta T2-T0, in different panels, for all assessment scales. No significant difference was found between the two groups for either of the two deltas, although the groups showed a different trend. Group 2 seemed to have greater absolute delta with respect to Group 1 for all evaluations except FAB and AES-S (for delta T2-T0) and UPDRSII and FAB (for delta T1-T0). Moreover, in Group 2 the absolute delta T2-T0 was greater than T1-T2 for UPDRS II, FAB and BDI while in Group 1 this was the case only for FAB and AES-S.
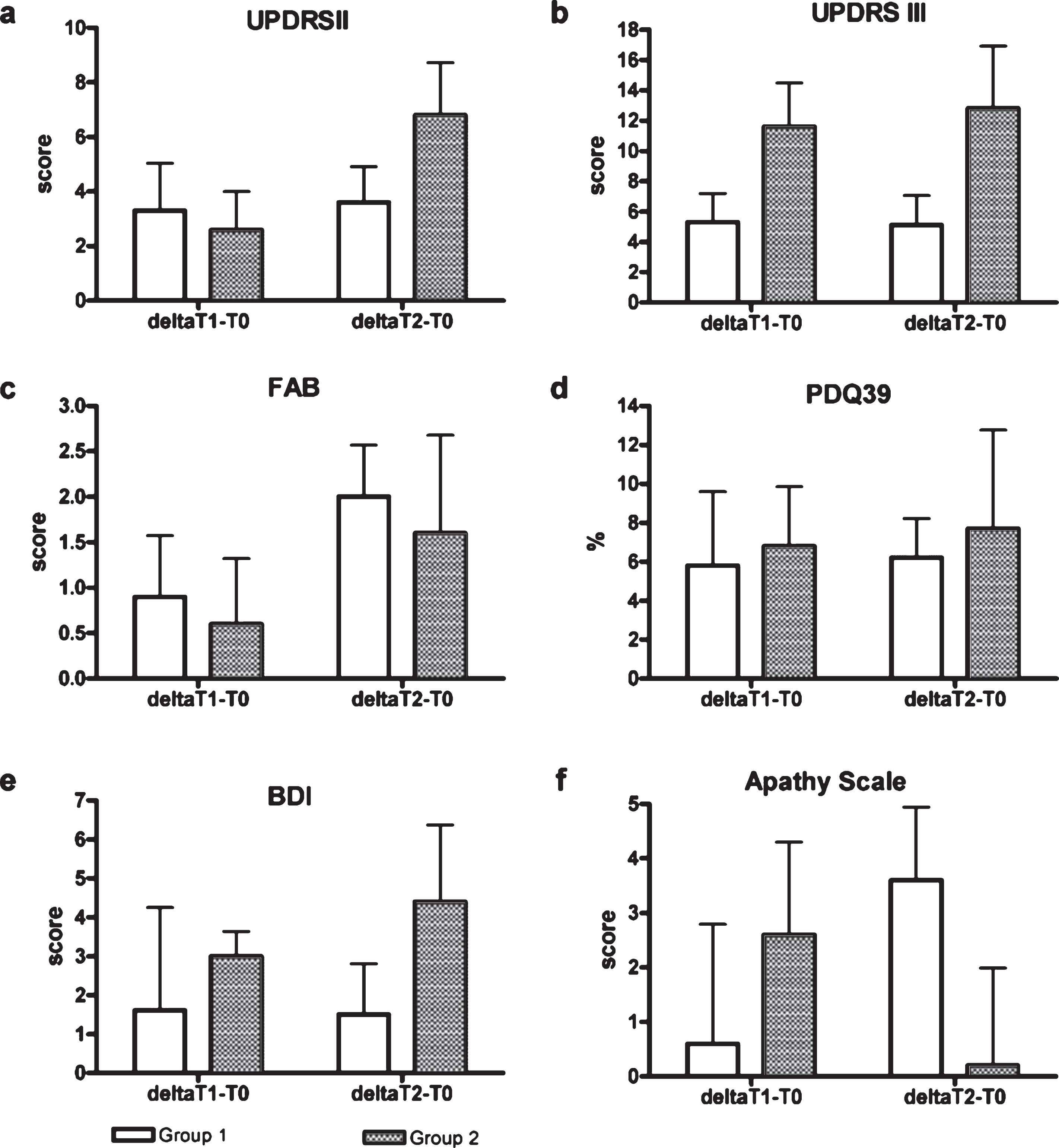
Comparison between Group 1 and Group 2 on absolute delta T2-T0 and T1-T0 related to motor and non-motor assessment scales. The panels refer to UPDRSII (a), UPDRS III (b), FAB (c), PDQ39 (d), BDI (e), and AES-S (f).
The main finding of this study is that the proposed multidisciplinary rehabilitation treatment (based on OT, NW and TT) leads to improved non-motor and motor outcomes, but the time when OT is scheduled within the rehabilitation program has no significant effect. Our findings are in line with reports in the literature showing that a proper multidisciplinary care program can improve motor and not-motor symptoms and quality of life in PD (Arbesman et al., 2014; Preissner, 2014; van der Marck et al., 2009). Occupational therapy and Nordic walking are valid tools to use in rehabilitation, as the recent literature confirms (Alwardat, 2018; Ferrazzoli et al., 2018; Monteiro et al., 2017; Radder et al., 2017; Sturkenboom et al., 2014).
In relation to the first aim of this study, ANOVA showed an improvement in both groups at the end of the study regarding most of the parameters assessed. This confirms the validity of the multidisciplinary intervention per se (Carne et al., 2005; Frazzitta et al., 2015) though it was not possible to compare the efficacy of OT+NW+TT with a control group, i.e. traditional rehabilitation program for PD patients. The improvement was most evident in the walking parameters 6MWT and GAIT (Table 3) and in the motor component of scales such as UPDRIII (Table 2), indicating that the positive effect of this program is mainly in the motor sphere. This is confirmed by the majority of studies in the literature that measure the effect of treatments in terms of measurable motor symptoms improvement (Bang & Shin, 2017; Warlop et al., 2017). We found a less significant improvement in UPDRSII (ADL area), FAB (executive function area) and PDQ39 (quality of life) confirming the positive impact of the rehabilitation program also in this area. Unfortunately, the poor standardization makes comparisons between studies difficult (Cusso et al., 2016; Frazzitta et al., 2015; Subramanian, 2017).
Analyzing the different PDQ39 dimensions, ADLs and communication were the two domains that showed significant improvement and influenced the improved PDQ39 summary index. These domains are closely connected to OT, whose primary focus is to support patients’ participation in daily life and relations. The ADL domain, at multiple regression analysis, also resulted as a significant independent predictor of motor function improvement. UPDRSII and UPDRSIII at T0 influenced absolute delta T2-T0 for both 6MWT and GAIT speed: a greater improvement was seen in patients with less deficit in ADL function but more motor impairment. Absolute delta T2-T0 for GAIT length was influenced by gender, age and PDQ39 (ADL and cognition) at T0: a greater improvement was seen in males and younger patients. Also for 6MWT and GAIT speed improvement, the correlation with gender was close to significant (p = 0.073 and p = 0.070 respectively): again we found a greater improvement in male patients (Table 4).
In relation to the second aim, in all statistical analyses conducted no significant differences emerged between the two groups. In ANOVA, only “Time” reached statistical significance in some parameters, but not “Group” nor the “interaction Group*Time” (Tables 2 and 3). In regression analysis, to investigate relationships between motor function improvement and T0 parameters, Group was included in the list of dependent variables, but it was not significant. Finally, comparison of the absolute delta T2-T0 and T1-T0 showed no significant difference between Group 1 and Group 2 concerning the improvement in any parameters (Fig. 1).
We found some differences between the two groups on the assessment scales change over time that, though not significant, merit comment. The high variability of the assessment scales and the low number of subjects investigated could have had an effect on significance. In fact, similar differences in median value and variability are significant in studies with greater sample size [e.g. PDQ39 between-groups: Control = 48, Experimental group = 186 in Ferrazzoli et al. 2018 (Ferrazzoli et al., 2018)]. Apart from AES-S, whose trend in time is difficult to interpret (Group 2 showed a smaller T0-T2 improvement than T0-T1), for the other 5 parameters analyzed we found an improvement at T2 versus T0 in both groups. Of note, Group 2 showed a continuous, clear, positive change over time in 3 of 5 evaluations (UPDRSII, FAB e BDI), while Group 1 only in 1 of 5 (FAB). Thus, we conclude that there are no differences between the two groups. However, though not significant, we note that: 1) the improvement in Group 2 seems more continuous in time, 2) improvement in BDI (not found in Group 1) is important because it suggests a positive change in depression state, 3) differences in the PDQ39 dimensions between the two groups are very difficult to interpret due to the great variability (data not reported). A possible explanation of points 2) and 3) is that OT introduced after a period of physiotherapy rehabilitation (Group 2) with its general benefit on motor deficits, especially thanks to NW, could be more effective in some non-specific motor areas because executed in a better patient general condition.
The low number of patients and the unbalanced group distribution may be minor limitations. The main limitation is surely the absence of a control Group (receiving only traditional treatment) but, assuming that rehabilitation of any kind lead to patient condition improvement, this study is designed to focus essentially on the way to obtain this improvement.
Conclusions
Patients following a multidisciplinary rehabilitation program including OT, although in a pilot study without a control group, show a significant improvement in their condition over time, more in the motor than non-motor area. This has an impact on patients’ quality of life as well and suggests the feasibility of the program, although no conclusions on efficacy can be drawn because of the absence of a control group (traditional rehabilitation program for PD). It is possible that some differences between OT planned at the beginning or at the end of rehabilitation could emerge with a greater number of patients. Future studies are necessary to investigate this point.
Conflict of interest
The authors report no conflict of interest. The work was supported by an Institutional funding.
Footnotes
Acknowledgments
The Authors thank Daniela Belleri and Michela Manfredi for collecting data, Daniel Peli for technical assistance, Lidia Gazzi for critical reading and Rosemary Allpress for the English revision.