
Abstract
BACKGROUND:
Individuals with extensive neuro-motor impairment and lack of speech tend to remain passive and isolated, and to rely on others for communication and leisure. While their problems are known, only limited evidence is available about intervention tools that could help them curb those problems.
OBJECTIVE:
This study was aimed at upgrading and assessing a smartphone-based technology package, which was recently developed to help those individuals to independently engage in basic communication and leisure.
METHODS:
The study included 11 non-ambulatory participants who had no speech or functional active communication. They were provided with (a) a Samsung A3 smartphone with Android 6.0 Operating System, which was fitted with WhatsApp Messenger and programmed via MacroDroid, and (b) cards fitted with radio frequency identification (RFID) tags. By bringing those cards in contact with the back of the smartphone, the participant could start a communication event (e.g., sending a message to a friend) or activate a leisure event (e.g., a song). The smartphone would automatically read to the participant any incoming messages.
RESULTS:
During the baseline (i.e., when a standard smartphone was available), the participants were unable to engage in communication or leisure. Once the aforementioned technology package was introduced, the participants spent between about 65 and 85% of their session time engaging in communication and leisure.
CONCLUSIONS:
The smartphone-based technology package seems to be a useful tool to support basic communication and leisure in individuals like those involved in this study.
Introduction
Extensive neuro-motor impairment and absence of speech are common among people with severe neurological damage due to congenital and perinatal causes (e.g., cerebral palsy) or a plurality of other causes, such as stroke, traumatic brain injury, and neuromuscular diseases (Anderlini, Wallis, & Marinovic, 2019; Basilakos, 2018; Feenaughty, Tjaden, Weinstock-Guttman, & Benedict, 2018; Lampe, Bluemenstein, Turova, & Alves-Pinto, 2018; Moser, Basilakos, Fillmore, & Fridriksson, 2016; Neto, Constantini, & Chun, 2017). The combination of extensive neuro-motor impairment and absence of speech can have a dramatically negative impact on the individual’s chances to engage in functional (e.g., leisure) activities as well as in communication with caregivers and staff present in the context and with distant people who can only be reached via telephone calls or text messages (Holmqvist, Thunberg, & Dahistrand, 2018; Lancioni et al., 2018a; Lyons, 2015; MacDonald, 2017; Thiessen, Brown, Beukelman, & Hux, 2017; Wade et al., 2018). Failure to manage leisure engagement and to interact/communicate with others can lead the individual to a condition of isolation, passivity, and unhappiness that cannot be ignored or underestimated within contexts in charge of his or her well-being (Buunk, Groen, Veenstra, & Spikman, 2015; Gauthier et al., 2018; Lancioni et al., 2018a; Manskow et al., 2017; Sharpe & Hemsley, 2016; Trojano, Moretta, Cozzolino, Saltalamacchia, & Estraneo, 2011).
Extended communication and leisure support by staff may produce some relief, but cannot be considered a realistic (long-term) strategy. Indeed, extended support would help improve the individual’s general condition, but may be excessively taxing for the context, and emphasize the individual’s overall dependence. The use of conventional information and communication technology devices (e.g., computers and smartphones) may not be feasible for many of these individuals due to the gap between the skills they possess and the skills required for operating those devices (Buchholz, Müller, & Ferm, 2013; Lancioni, 2018; Lancioni & Singh, 2014; Lemke, Rodriguez Ramirez, Robinson, & Signal, 2019; Manzoor & Vimarlund, 2018).
A possible way to address the situation of these individuals involves the use of technology-aided intervention solutions specifically designed to allow the individuals independent access to communication and leisure (Borgestig, Sandqvist, Ahlsten, Falkmer, & Hemmingsson, 2017; Brunner, Hemsley, Togher, & Palmer, 2017; Desai, Chow, Mumford, Hotze, & Chau, 2014; Lancioni et al., 2018a). One such technology-aided solution concerns eye tracking devices (Caligari, Godi, Guglielmetti, Franchignoni, & Nardone, 2013; Hwang, Weng, Wang, Tsai, & Chang, 2014; Spataro, Ciriacono, Manno, & La Bella, 2014). These devices rely on cameras or other specific sensors, which are activated through eye gaze responses and can thus be used by individuals with no hand control (e.g., individuals with advanced amyotrophic lateral sclerosis or severe cerebral palsy) for accessing communication and leisure. For example, Borgestig et al. (2017) reported encouraging results with the use of such technology (i.e., Tobii C12 or Tobii P10 devices) with 10 participants who had a diagnosis of cerebral palsy or cervical spinal cord injury and presented with extensive neuro-motor impairment and lack of speech. Some of them also had an unspecified level of cognitiveimpairment.
Another type of technology-aided solution to support individuals with extensive neuro-motor impairment and lack of speech involves computer systems programmed to present the individuals with communication and leisure options. The individuals can choose any specific option by activating a microswitch (e.g., by pushing a pressure device) in relation to the option being verbally and visually presented on the computer screen (Lancioni et al., 2017; Lancioni, Singh, et al., 2015; Stasolla et al., 2015). For example, Lancioni et al. (2017) set up and successfully used such a system to provide seven participants with acquired neurological damage and multiple disabilities the possibility of choosing among customized communication and leisure options including, among others, verbal requests, text messages, writing, songs, and television.
While the two types of technology-aided solutions mentioned above are considered to represent relevant tools to help individuals with extensive neuro-motor impairment and lack of speech, there are also reasons to argue that new technology-aided solutions are warranted for this group of individuals. For example, the eye tracking technology is excessive and inadequate if the individuals possess some use of their hands and can still rely on them for responding. Moreover, eye tracking technology is rather expensive and setting it up and teaching individuals to use it effectively can be quite difficult and time demanding (Borgestig et al., 2017; Lancioni, Simone, et al., 2015). Computer systems combined with communication modems and touchscreens or microswitches (see Lancioni et al., 2017) cannot be considered a very practical and up-to-date solution for supporting basic communication and leisure needs.
In light of the above, a pilot study was recently conducted with the aim of setting up and evaluating a more easily accessible and functional technology-aided solution (D’Amico, Lancioni, Buonocunto, Ricci, & Fiore, 2019). Such technology-aided solution (a) relied on two smartphones fitted with special applications and cards fitted with radio frequency identification (RFID) tags (Irani, Gunasekaran, & Dwivedi, 2010), and (b) was tested with six participants with extensive neuro-motor impairment and lack of speech. The cards, which were recognized by the smartphones based on their tags, showed pictorial representations/images of preferred communication partners, messages, leisure events, and the caregiver. For example, if the participant placed the card showing a communication partner on the back of the smartphone near him or her, this smartphone verbalized the name of the partner and asked the participant to select the message for that partner. When the participant placed a message card on this smartphone, it verbalized the message and triggered the second smartphone to send it out. If the participant placed a card showing a leisure event (e.g., a comic sketch) on the near smartphone, this smartphone played such event.
The positive communication and leisure engagement results obtained with the six participants using the smartphone-based technology solution described above are highly encouraging and motivate new research efforts to (a) upgrade the technology solution so that only one smartphone (rather than two) would be required for supporting communication and leisure, (b) evaluate the effects of the new, upgraded technology solution to determine whether previous results would be replicated, and (c) develop and evaluate an adapted (simplified) version of the new technology solution for individuals with extra needs. The present study was aimed at pursuing the aforementioned goals and included 11 participants. Eight of the participants were involved in the assessment of the new, upgraded technology solution. The other three participants were involved in the assessment of an adapted version of such technology solution.
Method
Participants
The participants presented with extensive neuro-motor impairment, which forced them to spend their time in a wheelchair or in bed, but were able to manipulate objects. They did not possess speech or functional alternatives for active communication. However, they had receptive language skills that allowed them to understand and respond appropriately (e.g., with “yes” and “no” head movements) to questions pertaining to their life, family, and daily events. Table 1 lists the participants by their pseudonyms, and reports their ages, their neurological disorders, their level of functioning, and the time gap between the diagnosis of their neurological disorders and the start of this study. The participants were between 35 and 83 years old. Three of them (i.e., Alan, Peter and Evelyn) were considered to have mild cognitive impairment, based on assessment guidelines from the Global Deterioration Scale (Reisberg, Ferris, de Leon, & Crook, 1982). The other participants were considered to be between the V/VI and the VII levels of cognitive functioning based on the Levels of Cognitive Functioning Scale-Revised (Hagen, 1998).
Participants’ Pseudonyms, Ages, Neurological Disorders, Cognitive Functioning, and Intervals between Disorder Diagnosis and Start of the Study
Participants’ Pseudonyms, Ages, Neurological Disorders, Cognitive Functioning, and Intervals between Disorder Diagnosis and Start of the Study
1The cognitive functioning is based on the Global Deterioration Scale for the first three participants and the Levels of Cognitive Functioning (LCF) Scale-Revised for the other participants.
The participants’ neurological disorders were connected to (a) neuromuscular diseases (i.e., Alan and Evelyn), (b) multiple sclerosis (i.e., Peter), (c) posterior circulation infarct (i.e., Max, Liz, and Tracy), (d) partial anterior circulation infarct (i.e., Denis), and (d) intraparenchymal hemorrhage (i.e., Kevin, Ruth, Roger, and Edgar). The neurological disorders had been diagnosed between 2 and 11 months prior to the start of this study except for Alan, Peter, and Evelyn. For these participants, the time gap between the diagnosis and this study was of about 3, 6, and 30 years, respectively.
All participants were in medical rehabilitation and care centers, in which they were provided with conventional treatments, such as physiotherapy and occupational and language therapy. Direct observations had indicated that they possessed the main prerequisites for using a smartphone-based technology solution to access communication and leisure on their own. In addition to the receptive language and object manipulation skills mentioned above, in fact, the participants (a) were capable of identifying all the images/representations reported in the cards to be used with the smartphone (some of them could also read printed words), (b) were interested in sending messages to their preferred partners (e.g., family members and friends) and enjoyed listening to the messages received from those partners, and (c) liked to engage in leisure activities (e.g., listening to songs and watching videos of comedy sketches and sport events). Moreover, participants had shown willingness to use the smartphone-based technology (i.e., after demonstrations of its functioning from a research assistant).
Preliminary assessment trials on sending messages (i.e., trials which were introduced by the research assistant describing the response sequence required) provided the following indications. Eight participants (i.e., Alan, Peter, Evelyn, Max, Liz, Kevin, Ruth, Edgar, and Neil) had no difficulties with the task and selected the card of the partner to whom a message was to be sent before the card of the message. The other three participants (i.e., Tracy, Denis, and Roger) showed some inconsistency in organizing the response. For example, they could vary the order with which they took the card with the message and the card of the partner. Based on those trials, the first eight participants were exposed to the upgraded smartphone-based technology solution in its standard form. The other three were exposed to an adapted version of such technology solution (i.e., a version set up to help them avoid failure/frustration). The participants’ families had signed a written consent form on their behalf for their inclusion in the study. The study complied with the 1964 Helsinki declaration and its later amendments and had been approved by an institutional Ethics Committee.
Quiet areas of the centers that the participants attended served as setting for the study. Sessions were conducted on an individual basis, typically two to four times a day, 3 to 5 days a week. The participant was sitting in a wheelchair or in bed, in front of a table containing a smartphone and cards arranged on a panel. Figure 1 provides a view of the smartphone and the panel on the table top. The panel was to the right or the left of the smartphone depending upon the hand the participant used for manipulating the cards. Sessions were scheduled to last 10 min. However, the participant could complete any leisure or communication event that had been started within that limit, with consequent extension of the session duration.
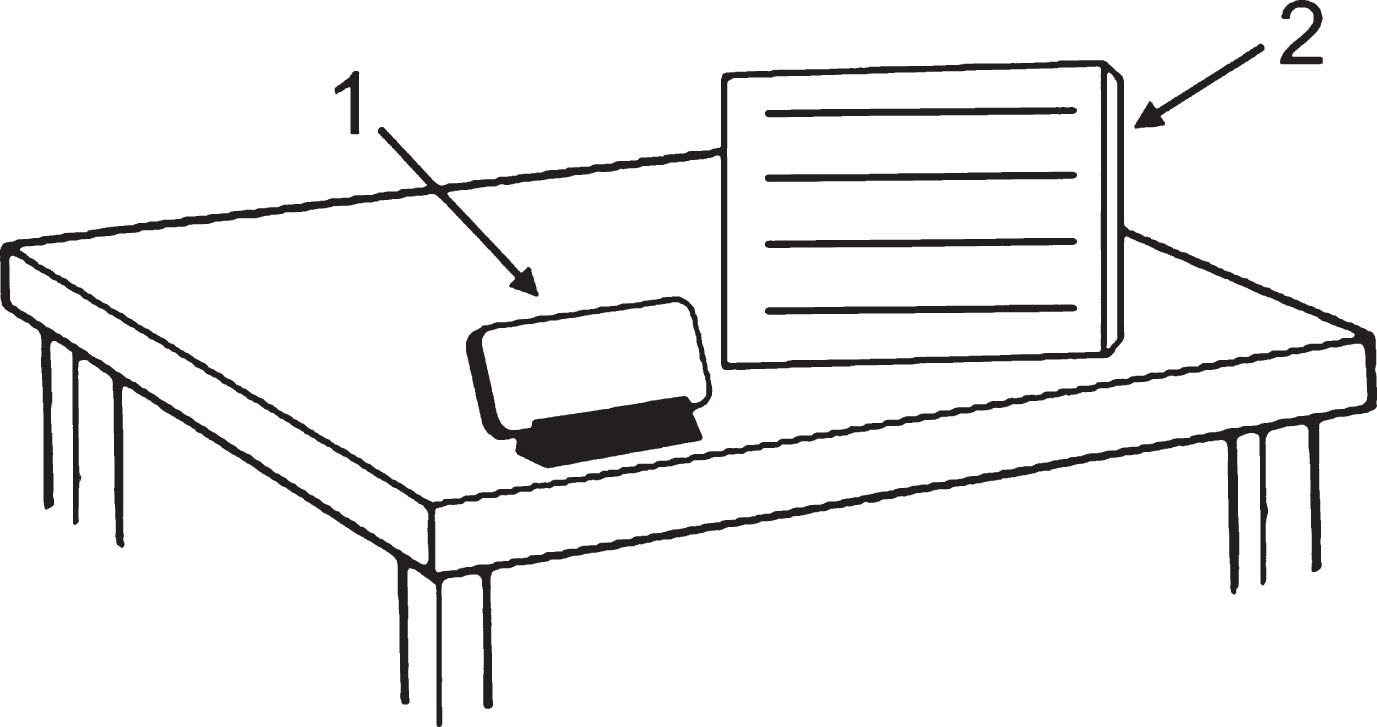
The drawing provides a view of the smartphone (1) and the panel (2) on the table top.
Data recording was conducted by research assistants and concerned the communication and leisure events the participants accessed and the times they spent engaging in those events. Communication events included messages sent out, messages received, and caregiver calls with subsequent responses by the caregiver (see below). The engagement time for messages sent out, caregiver calls, and leisure events also included the participant’s selection of the cards needed to activate them. Recording agreement was checked in at least 20% of the sessions of each participant, with a reliability observer joining the research assistant in data recording. Agreement (requiring that the research assistant and reliability observer reported the same communication and leisure events and total engagement times for each of the two types of events differing less than 45 s) was obtained in more than 90% of the sessions of each participant.
A Samsung A3 smartphone with Android 6.0 Operating System, proximity sensor, multimedia player, near field communication, and Google Assistant was used in connection with a mini speaker. The smartphone was fitted with the WhatsApp Messenger application, which allowed free message exchanges, and the MacroDroid application, which allowed the automation of the smartphone’s functioning in line with intervention and post-intervention conditions (see below). The smartphone was also supplied with numerous multimedia files concerning: the WhatsApp messages that could be sent out (e.g., “I love you”, “I wish you a good day”, “When do you visit me?”), the telephone numbers of the communication partners (i.e., for sending messages), and the leisure options available (e.g., music, comedy sketches, and sport events).
Participants’ cards
During intervention and post-intervention sessions, participants were provided with cards to use with the smartphone (see Setting, sessions, and data recording). Every card was fitted with a RFID tag (Irani et al., 2010), which enabled the smartphone automated via the MacroDroid to discriminate the card and thus respond to it appropriately. The eight participants who were exposed to the upgraded smartphone-based technology solution had 19 cards, out of a pool of about 25, during each session. Four cards contained images and printed names of preferred communication partners. Six cards contained pictures with printed words illustrating the messages (e.g., the picture of a heart for “I love you” and the picture of a bed of the rehabilitation center for “When do you visit me?”). Eight cards contained pictures with printed words indicating the leisure events. One card contained a caregiver image. The participants discriminated the cards and their meanings (see Participants).
The three participants who were exposed to the adapted version of the upgraded technology solution had 15 cards, out of a pool of about 20, during each session. Eight cards contained combinations of partners and messages. Specifically, the image of each of four partners was combined with the picture of two messages. For example, the image of the participant’s daughter was combined with the picture of a heart and the picture of a rehabilitation center’s bed for sending the daughter the messages “I love you” and “When do you visit me?”, respectively (see Fig. 2). Six cards contained pictures of leisure events, and one card contained a caregiver image. Combining the image of preferred partners with message pictures allowed the participants to send messages to those partners with one response (rather than a sequence of two), thus simplifying their performance.
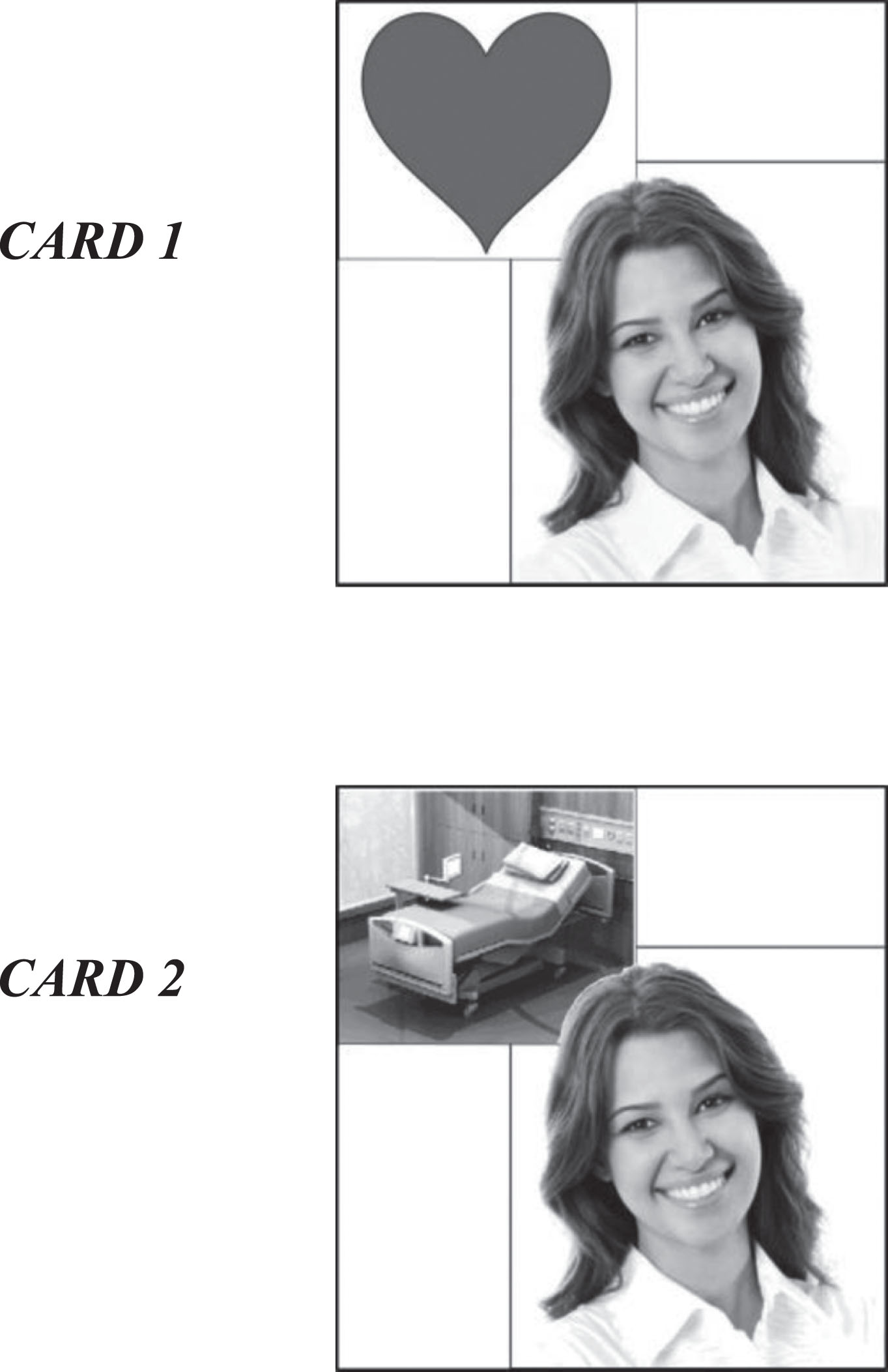
Cards 1 and 2 show the image of the participant’s daughter combined with the picture of a heart and with the picture of a rehabilitation center’s bed. The cards served to send the daughter the messages “I love you” and “When do you visit me?”, respectively.
The caregiver (i.e., the person who was attending to the participant at the time of the session) had seven cards that she showed to the participant when the participant called her (see below). The cards contained pictures of events such as grooming, drinking, handkerchief, and cream. The cards (the events they represented) were discriminated by the participants.
Experimental conditions and data analysis
A non-concurrent multiple baseline design across participants (Barlow, Nock, & Hersen, 2009) was used for each of the two groups of participants. The baseline phase was followed by an intervention phase (introducing the participants to the use of the automated smartphone and cards) and a post-intervention phase. The research assistants, who conducted the data recording (see above), were also responsible for the implementation of the sessions. The participants’ baseline and post-intervention data on communication and leisure engagement were reported in graphic format. The Kolmogorov-Smirnov test was to be used for assessing differences between phases if overlaps existed in the session engagement times (i.e., communication and leisure times combined) of those phases (Parker, Vannest, & Davis, 2011; Siegel & Castellan, 1988). No such overlaps however occurred.
Baseline
The baseline phase included four to seven sessions for the group of eight participants and four or eight sessions for the group of three participants. During these sessions, the participants were provided with a Samsung A3 smartphone, which was fitted with the aforementioned multimedia files but had not been automated via the MacroDroid, and thus could not be used with the cards. The participants could send messages, call the caregiver, or access a leisure event by using appropriate manual inputs. Similarly, incoming messages could only be retrieved through the required sequence of manual inputs. At the start of the sessions, the research assistant modeled the manual sequences required to send a message and to access a leisure event and asked the participant to perform those sequences. During the session, the research assistant encouraged the participant to carry out those sequences and modeled one of them again.
Intervention
The intervention phase included four to eight sessions during which the participants used the smartphone automated via the MacroDroid and the cards with RFID tags. During the initial sessions, the participants performed the responses required for sending messages, accessing leisure activities, and calling the caregiver with the help of verbal and physical prompts from the research assistants (Lancioni et al., 2018b). During the following sessions, the prompts were reduced and eventually eliminated.
The conditions in use for the group of eight participants are summarized in Fig. 3. If the participant brought a card with a communication partner into contact with the back of the smartphone, the smartphone verbalized the name of the partner and asked the participant what message he or she wanted to send to the partner. As soon as the participant brought a message card into contact with the back of the smartphone, the smartphone verbalized the message and sent it out to the partner selected. If the participant brought a card representing a leisure event (e.g., a comic sketch or song) into contact with the back of the smartphone, the smartphone named the event and played it for about 2 min. If the participant brought the caregiver card into contact with the back of the smartphone, the smartphone called the caregiver who then approached the participant and showed seven cards (see above). The participant’s selection of one of the cards led the caregiver to provide the participant with what the card represented (e.g., with a handkerchief or the combing of his or her hair). Conditions for the group of three participants were as those mentioned above, except that they could send out a message by using a single card (i.e., a card with a partner and a message).
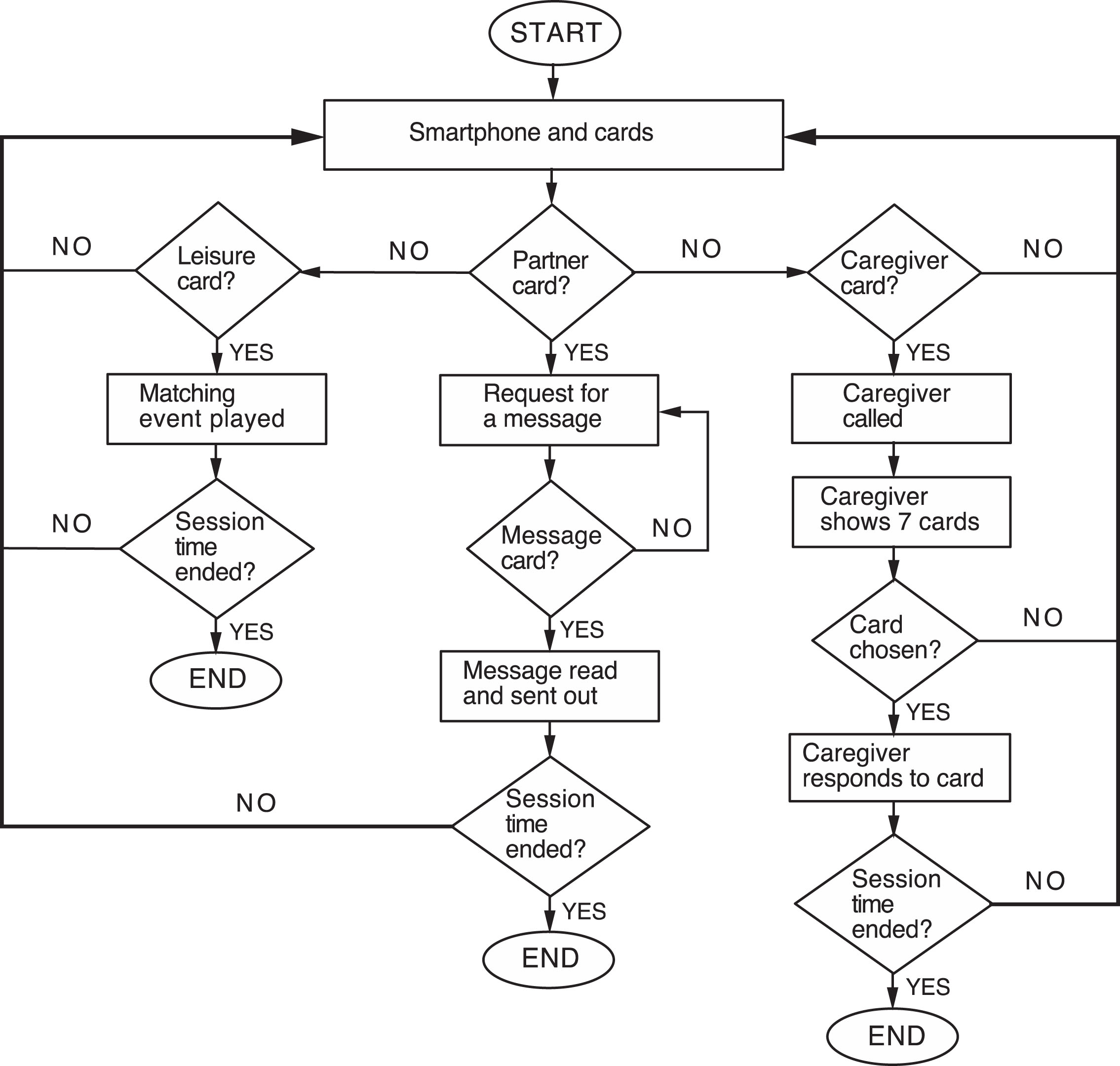
The flowchart illustrates the smartphone and cards’ functioning and the caregiver’s responding.
Conditions for incoming messages were identical across all participants. That is, the messages and the name of the senders were automatically read by the smartphone. Messages arriving during a session were read immediately or shortly after their arrival (not to interfere with ongoing communication events). Messages arriving outside the sessions were read at the start of the next session.
The post-intervention phase included 59 to 108 sessions for the participants of the first group and 47 to 101 sessions for the participants of the second group. Conditions were as those applied at the end of the intervention phase with no research assistant’s prompts available.
Results
The eight panels of Fig. 4 and the three panels of Fig. 5 summarize the data for the participants of the two groups, respectively, during the baseline and the post-intervention phase (i.e., when no prompts were available). The intervention sessions are not reported in the figures, as they simply introduced theparticipants to using the automated smartphone and cards with RFID tags. The bars’ height indicates the mean percentage of session time that the participants spent engaging in communication and leisure over a block of baseline or post-intervention sessions. The black and gray sections of the bars indicate mean percentages of session time spent in communication and leisure, respectively.
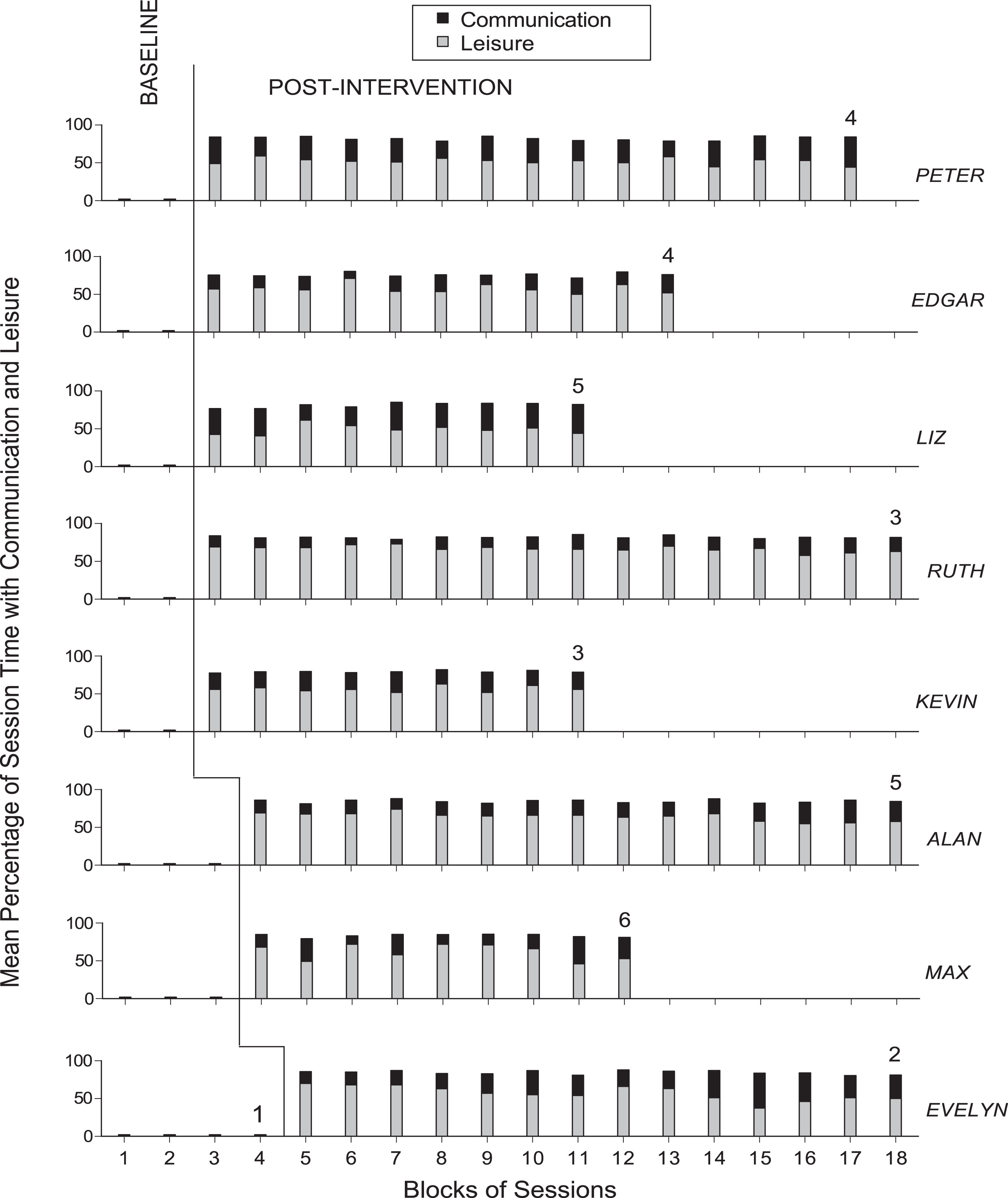
The eight panels show the baseline and post-intervention data for the eight participants of the first group. The bars’ heights indicate mean percentages of session time the participant spent engaging in communication and leisure over blocks of baseline and post-intervention sessions. A bar represents a block of two sessions during baseline and seven sessions during the post-intervention phase. Exceptions are marked with a numeral indicating how many sessions are included. The black and gray sections of the bars indicate the mean percentages of session time spent in communication and leisure, respectively.
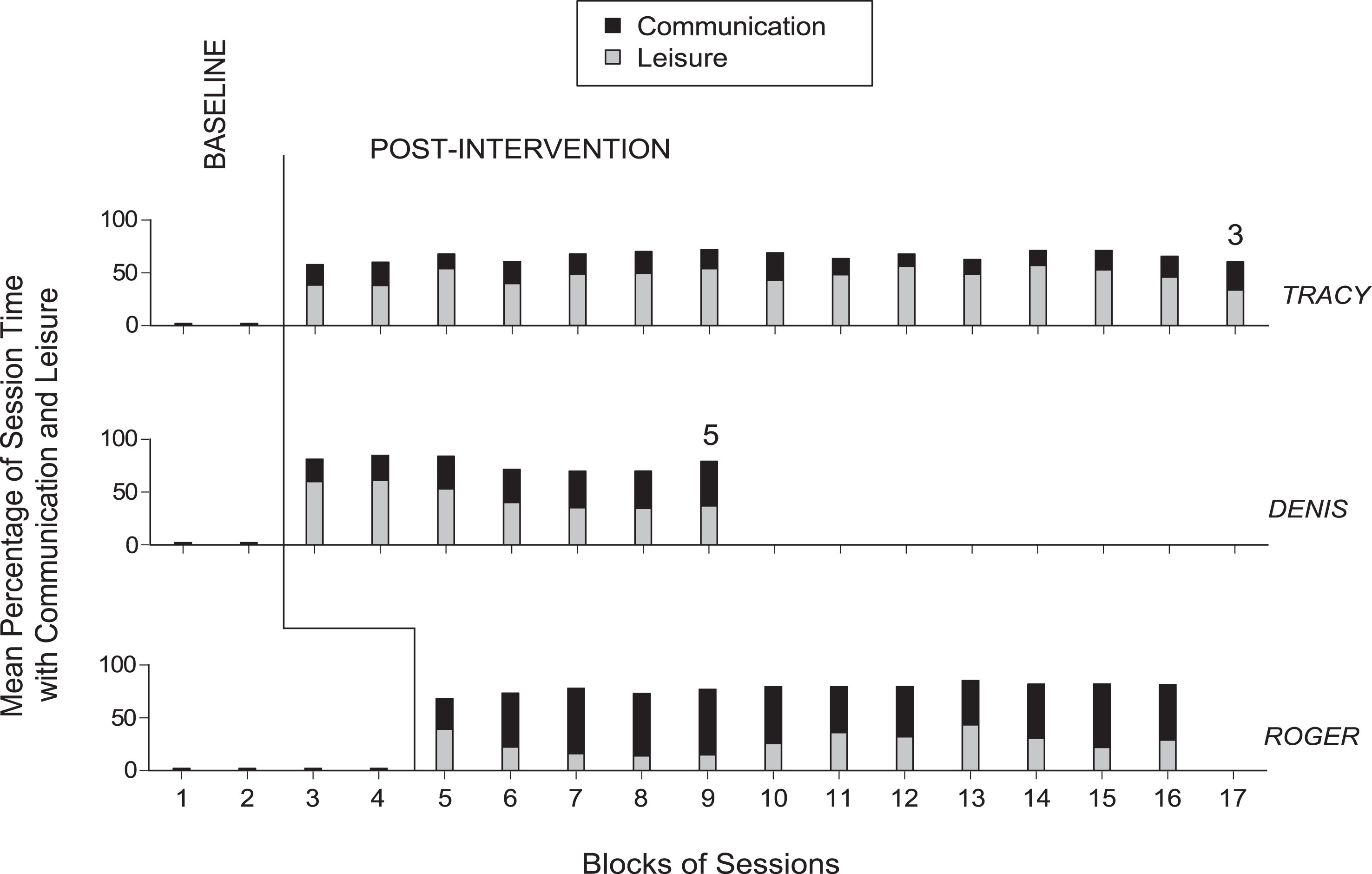
The three panels show the baseline and post-intervention data for the three participants of the second group. Data are plotted as in Fig. 4.
During the baseline, the participants of the two groups were unable to use the standard smartphone available to them, in spite of the research assistant’s modeling, and therefore did not manage any communication or leisure engagement. During the intervention sessions, the participants of both groups learned to use the automated smartphone and cards to send messages, call the caregiver, and access leisure events. They also received messages that were read out to them automatically.
During the post-intervention phase, data showed that all participants consolidated their ability to use the technology independently, and successfully accessed communication and leisure events. The mean amount of time spent in communication and leisure together reached levels of about 75–85% and 65–80% of the total session time for the participantsof the first group and of the second group, respectively. The mean amount of time spent in communication ranged from above 15% (Ruth) to above 30% (Peter and Liz) of the total session time for the participants of the first group, and from about 20% (Tracy) to about 50% (Roger) of the total session time for the participants of the second group. The mean amount of time spent in leisure ranged from close to 50% (Liz) to about 65% (Ruth) of the total session time for the participants of the first group, and from about 25% (Roger) to about 45% (Tracy) of the total session time for the participants of the second group.
The results of the study suggest that the new, upgraded smartphone-based technology solution and the adapted version of it were effective in helping participants with extensive neuro-motor impairment and lack of speech to independently access communication and leisure events. These results, which are in line with those of the pilot study by D’Amico et al. (2019), (a) confirm that smartphone-based technology solutions can help these people achieve levels of self-determination and engagement that would be unattainable without technology support, and (b) the smartphone-based technology solutions can be upgraded and adapted to improve their practicality and usability with persons with different needs. In light of the above, a number of considerations can be made.
First, the upgraded smartphone-based technology solution used with the first group of eight participants and the adapted version of such solution used with the second group of three participants appear readily accessible in terms of components/materials, easily affordable in terms of costs, and friendly for the user. Indeed, the smartphone is a highly conventional and fairly inexpensive device. Applications such as the WhatsApp Messenger and the MacroDroid or accessories such as the RFID tags are available free of charge or for a negligible price. The responses required from the participants are rather basic and frequently available in the participants’ repertoire and can also be simplified/shortened by adapting the technology solution used (i.e., to maximize success for each participant).
Second, the smartphone-based technology solutions applied for the two groups of participants were apparently quite suitable for them to use. Indeed, the data showed that each of the participants learned to manage the technology solution available to him or her with a small number of intervention sessions and easily maintained a highly successful performance throughout the post-intervention phase. One question left without answer is whether the participants of the second group continued to require the adapted technology solution or eventually reached the same level (and thus could use the same technology solution) as the participants of the first group.
In addition to managing the technology solutions successfully, the participants were informally reported to enjoy the sessions. This point seems to be in line with general expectations. One would have, in fact, expected the participants’ enjoyment, given that the technology and sessions allowed them to freely access communication and leisure events, which were known to be meaningful and pleasant for them (Lancioni et al., 2018a, 2018b; Pierce & Cheney, 2008).
Third, it is important to clarify that the smartphone device used for the two groups of participants, albeit readily accessible and inexpensive, is not functional unless it is specifically arranged for the particular purpose of supporting the participants’ communication and leisure engagement (Lancioni et al., 2018a; Plackett, Thomas, & Thomas, 2017). To meet this purpose, one needs to fit the smartphone with a variety of communication and leisure files and to program it according to the needs of the participants. Programming the smartphone involves the use of applications such as the MacroDroid or the WPC-Walden Personal Communicator, and requires a certain level of expertise that may not always be available among caregivers and staff personnel (D’Amico et al., 2019; Kuo, Liu, & Ma, 2013; Lancioni et al.,2018a).
Fourth, different views can be expressed about the cards employed with the smartphone. One view may stress that cards are simple, easy to arrange and to fit with RFID tags, and thus largely practical to manage for staff and caregivers. Another view may emphasize the fact that cards require the participant to possess basic hand responses and thus cannot be used with everybody. With regard to this latter view, it is noteworthy that basic (sufficient) hand responses are often present in the repertoire of people like the participants of this study. Caution is, however, needed with participants with neuromuscular diseases who are likely to lose those responses over time (Lancioni, Simone, et al., 2015; Verde, Del Tredici, Braak, & Ludolph, 2017). For these individuals an adaptation of the technology solution would be eventually required. For example, the participant might be provided with a second smartphone, which is programmed to allow him or her to signal the card he or she wants to use through small head movements.
Fifth, some limitations of the study need to be mentioned here. One limitation is the relatively small number of participants included. New studies with additional participants are needed to assess the effectiveness of the new upgraded technology version as well as its adaptation and determine the reliability of the data obtained in this study (Kazdin, 2011; Makel & Plucker, 2014). New studies may also investigate ways of extending the range/number of communication and leisure options available during the sessions without complicating the response requirements. A second limitation concerns the lack of specific data on (a) whether the participants of the second group eventually became capable of using the same technology as the participants of the first group, and (b) whether the participants of both groups displayed indices of satisfaction/happiness during the post-intervention sessions (Dillon & Carr, 2007; Parsons, Reid, Bentley, Inman, & Lattimore, 2012). Answers to these questions would have important technical and practical implications and should be pursued in further studies. A third limitation is the absence of a social validation of the technology solutions and their impact (Callahan, Henson, & Cowan, 2008; Lenker, Harris, Taugher, & Smith, 2013; Luiselli, Bass, & Whitcomb, 2010). New studies should include such a validation by interviewing staff and families and determining whether their opinion confirms the positive reports obtained in the pilot study by D’Amico et al. (2019).
In conclusion, the results of this study indicate that the new smartphone-based technology solutions were effective in supporting communication and leisure engagement in individuals with extensive neuro-motor impairment and lack of speech. Although quite encouraging this evidence needs to be substantiated by new research before one can draw general conclusions about the aforementioned technology solutions. New research should also (a) address the limitations of this study and (b) determine whether it would be beneficial for the participants to have the technology solutions available throughout the day (rather than for specific sessions), with the provision that staff would rotate some of the cards available.
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
Ethical approval
Approval for the study was obtained from an institutional Ethics Committee. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
The participants’ families provided written informed consent for the participants’ involvement in the study.