
Abstract
BACKGROUND:
Game-based exercise is effective for improving strength and motor function in stroke patients undergoing rehabilitation, and it creates fun and motivation for exercise.
OBJECTIVE:
We investigated the effect of game-based exercise on hand strength, motor function, and compliance in stroke patients.
METHODS:
Fifty stroke patients were randomly divided into experimental and control groups. The experimental group performed a game-based hand resistance exercise. This exercise was divided into isotonic and isometric types and was performed 30 min/day, 5 days/week, for 6 weeks with 70% of the 1-repetition maximum. In contrast, the control group was given a traditional manual exercise by the occupational therapist, and the type of exercise and time involved were the same as those in the experimental group. The primary outcome measure was hand strength test measured using a dynamometer. Secondary outcome measures were manual function tests (MFT) and hand function tests using box and block test (BBT). Subject-based reports of motivation, fun, pain/fatigue evaluated on 0 to 10 numeric rating scales were compared between groups.
RESULTS:
After training, hand strength, MFT and BBT was improved in the experimental group compared to the control group (P < 0.001, both). Subject-based reports of motivation and fun was significantly greater in the experimental group than the control group (P < 0.001, both), except to pain/fatigue (P = 0.728).
CONCLUSIONS:
In conclusion, we demonstrated that game-based exercise is more effective than manual exercise in improving muscle strength, motor function, and compliance in stroke patients.
Introduction
Resistance training in rehabilitation is a typical intervention used to increase muscle strength and improve function (Magni et al., 2017). Hand resistance training has traditionally been used in therapist’s manuals; however, it is not possible to objectively apply an amount of resistance, and it is not easy to apply force for a long time because of limitations involving the physical effort of the therapist. Resistance training is possible using elastomeric materials such as Theraband and springs, as well as the therapist’s manual (Iversen et al., 2017; Vinstrup et al., 2018); however, these also have limitations that make it difficult to quantify resistance. Also these exercises are simply and repetitively performed against resistance, making it difficult to have fun and maintain interest during training.
Successful rehabilitation requires a variety of factors. In resistance training, it is very important to provide the amount of resistance objectively. The concept of 1-repetition maximum (1-RM) is applied to provide an objective resistance value (Tan et al., 2018). A 1-RM was defined as the highest amount that can be generated once. Therefore, training values are set based on 1-RM for effective training. Another important factor for effective resistance training is motivation (Kothari et al., 2014). Resistance training is an exercise that requires much repeated physical effort; therefore, it is important to increase motivation of the exercise using visual feedback. Motivation not only increases the duration of training but also reduces dropout. Motivation also has a positive effect on motor performance.
Games using computers or mobile devices can adjust the intensity of resistance objectively (Dehem et al., 2019). Various types of visual and auditory are possible and can be performed intuitively. These devices increase the motivation of the training by inducing fun and interest (Kothari et al., 2014). Finally, they create the possibility to concentrate more on exercise and to maintain exercise for longer periods. Therefore, this study investigated to compare the effects of a game-based hand resistance exercise and traditional manual exercise on hand strength, motor function and compliance in hemiplegic patients following stroke.
Methods
Simple size estimation
Sample size was calculated using G-power 3.1 software (University of Dusseldorf, Dusseldorf, Germany). The power and alpha levels were set at 0.80 and 0.05, respectively, and the effect size was set at 0.8. According to a prior analysis, each group required at least 21 subjects. Therefore, we assigned 25 subjects to the experimental group and 25 subjects to the control group in anticipation of dropout.
Participants
We recruited 50 patients with hemiplegia after stroke in two university hospital, South Korea. The inclusion criteria were as follows: (1) within 6 months of stroke onset; (2) no significant cognitive deficit (a score of >24 points on the Mini-Mental Status Examination); (3) no limited range of motion of the wrist and hand; (4) Fair grade < manual muscle test of wrist and hand; (5) ability to grip various forms (cylindrical, spherical, and power grip); (6) grip power <30 kilogram; and (7) ability to follow study instructions. The exclusion criteria were as follows: (1) secondary stroke; (2) other neurological diseases; (3) osteoarthritis or rheumatoid arthritis; (4) unilateral neglect or visual filed deficits; and (5) serious pain or swelling, or edema of the affected hand. All participants provided written informed consent forms approved by the institutional review board of Seoul Medical Center, South Korea (SEOUL2018-10-009-001).
This study was registered in the Clinical Research Information Service of Korea National Institute of health (no. KCT0003536).
Study procedure
This study was designed as a 6-week, assessor-blind, two-group, block randomized controlled trial. The participants were randomly assigned to an experimental group (n = 25) or control group (n = 25). The experimental group underwent game-based hand resistance exercise using TPS system (TPS 100, South Korea, Cybermedic Inc.). The TPS system is designed as a resistance training tool using game-based visual feedback. The TPS system consists of pressure sensor, air grip bulb and displayable products (e.g., tablet PC, smartphone) for resistance training. The pressure sensor and tablet PC were connected by Bluetooth (Fig. 1). The external force applied to the sensor was automatically displayed on the Tablet PC screen in various types of information (e.g., figure, value). Before training, the 1-RM was measured to determine resistance training values. 1-RM measured the maximum grip power of the paralyzed hand using a grip bulb of TPS system. This study applied the resistance value to be 70% of the 1-RM.
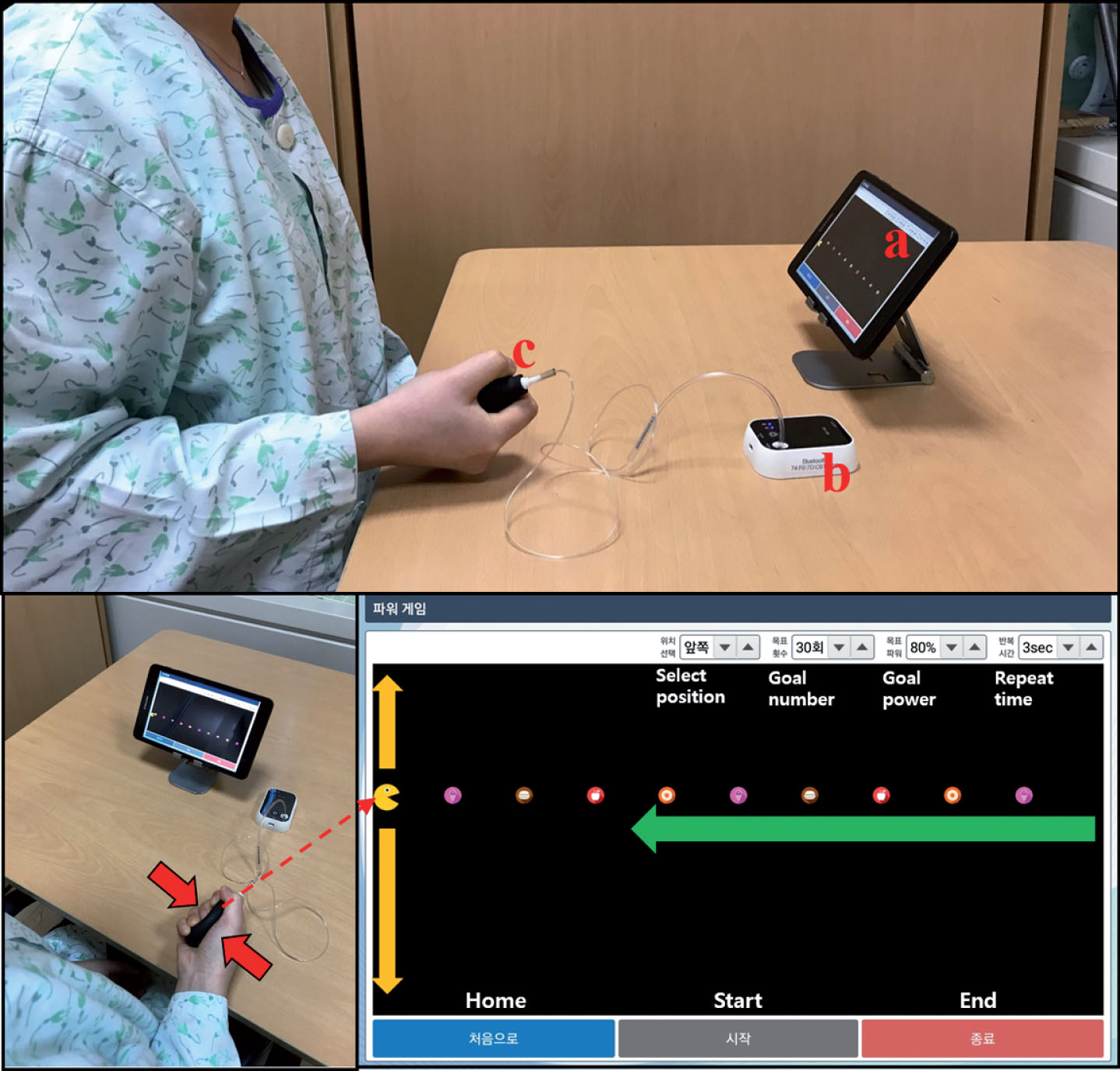
Game-based hand resistance exercise (a) Tablet PC (b) Pressure sensor (c) Air grip bulb. When the pressure is applied to the air grip bulb, the pressure is transmitted to the pressure sensor. The information is then transmitted to the table PC via Bluetooth.
Game-based hand resistance exercise is divided into isotonic and isometric types. Isotonic exercise involves holding the air-bulb with the paralyzed hand and pressing the bulb until the set resistance value (70% of 1-RM) is reached. Then the subject holds for 2 seconds and slowly releases again. In other words, concentric and eccentric contraction is repeated. The isometric exercise method is as follows. The subject holds the air-bulb with the paralyzed hand and presses the bulb for about 10 seconds until it reaches the set resistance value, releasing it slowly again (Fig. 1). Game-based hand resistance exercise performed 30 min/day, 5 days/week, for 6 weeks.
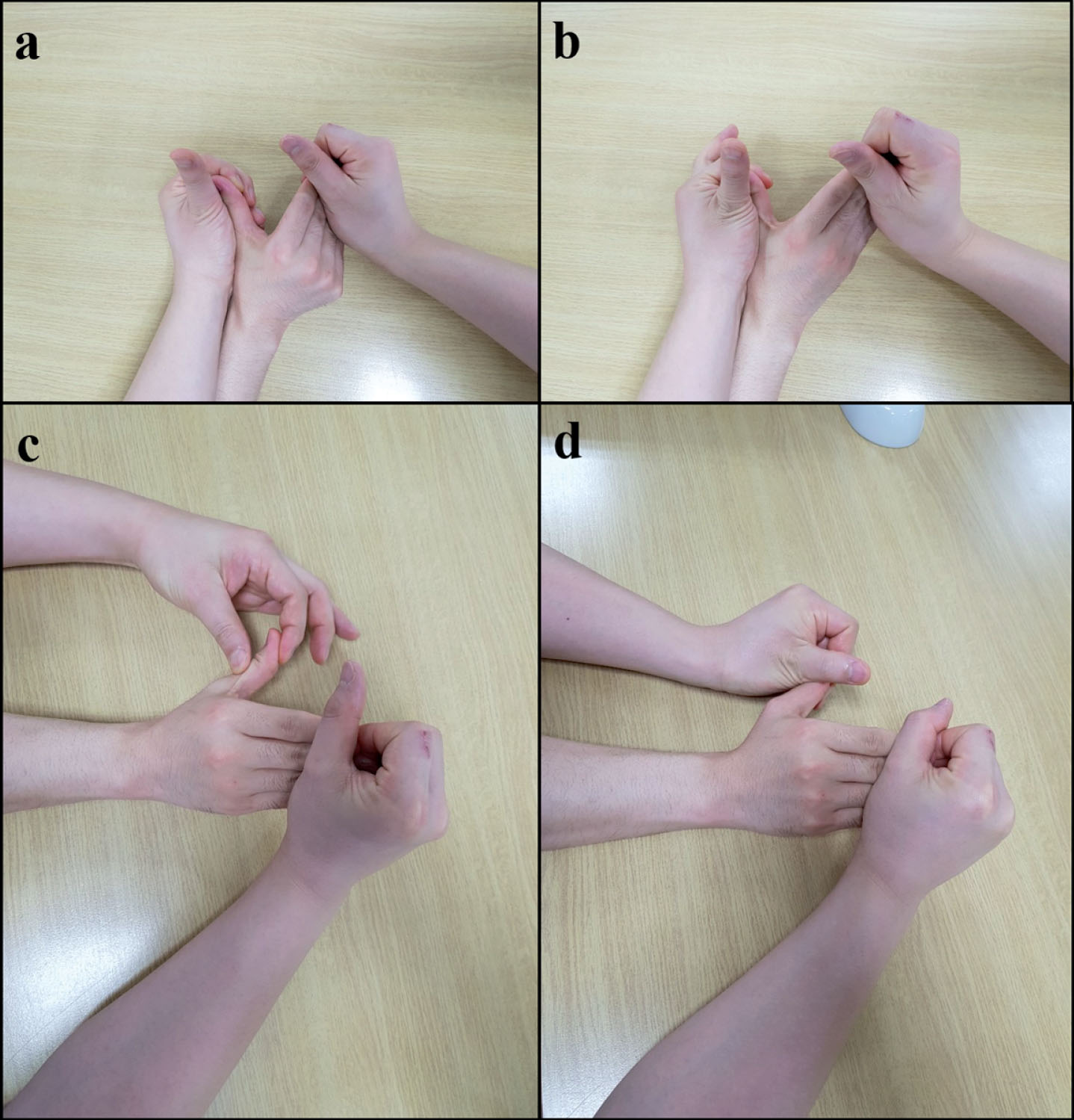
Traditional manual exercises. (a) (b) Exercise of metacarpophalangeal joint (c) Exercise of interphalangeal joint in thumb (d) Exercise of carpometacarpal joint in thumb.
While, control group received traditional manual hand exercises by an experienced occupational therapist. Traditional manual hand exercise was divided into isotonic and isometric types, including resistance exercise of the metacarpophalangeal joint in the fingers, and interphalangeal and carpometacarpal joint in the thumb (Fig. 2). Both groups received the same type of exercise, and the time involved in the exercise was also the same. Additionally, both groups were treated with the same traditional rehabilitation (e.g., occupational and physical therapy). The subjects’ characteristics and all outcome measures were assessed before and after (6 weeks) the intervention by an experienced physician and occupational therapist.
The primary outcome measure was the hand grip strength test using a hydraulic dynamometer (Jamar Technologies, Horsham, PA). The participants adopted a seated, upright position on a height-adjustable chair with their feet supported, shoulders adducted and neutrally rotated, elbow flexed at 90 degree, the forearm in neutral position, and the wrist at extension between 0 and 30 degrees. Three consecutive measurements were taken and mean values were recorded.
The secondary outcome measures were the box and block test (BBT) and manual function test (MFT). BBT is a standardized test to evaluate gross motor hand function. In the BBT, patients grasp a block from one side of a box, transport the block over a middle barrier, release the block to the other side of the box, and repeat the procedure as fast as possible. If they throw a box without transporting it, the repetition is not counted. The number of blocks moved within 60 seconds determines the BBT score (Mathiowetz et al., 1985).
The patients were also evaluated for upper extremity motor functions using the manual function test (MFT). The MFT consisted of 8 items as follows: forward and lateral elevation of the arm, touching the occiput and the back with the palm of the hand, grasping, pinching, carrying a cube, and pegboard manipulations. The MFT score ranged from 0 points (severely impaired) to 32 points (full function) (Miyamoto et al., 2009).
We used a 0-to-10 numeric rating self-report scale after every training session to assess motivation, fun, and pain/fatigue of the exercise. On the scale, 0 indicated no motivation, fun, pain/fatigue (Kothari et al., 2014).
Data analysis
Statistical analyses were performed using SPSS version 15.0 (IBM Corporation, Armonk, NY, USA). Descriptive statistics are presented as means with standard deviations. The Shapiro–Wilk test was used to check normality of the outcome variables. To evaluate training effects, the paired t-test was used to compare measures before and after the intervention in each group. The independent t-test was used to compare post-intervention values and changes in outcome measures between the two groups. Significance level was set at p < 0.05. In addition, the effect sizes (Cohen d) were calculated by dividing the standardized mean difference between the two groups using the pooled standard deviation. Effect sizes (Cohen’s d) of 0.2, 0.5 and 0.8 represented small, moderate and large effects, respectively.
Results
General characteristics and homogeneity test
In total, 45 participants completed the study. Five participants dropped out prior to the follow-up because of discharge. Figures 1–4 shows the CONSORT diagram of participant recruitment.
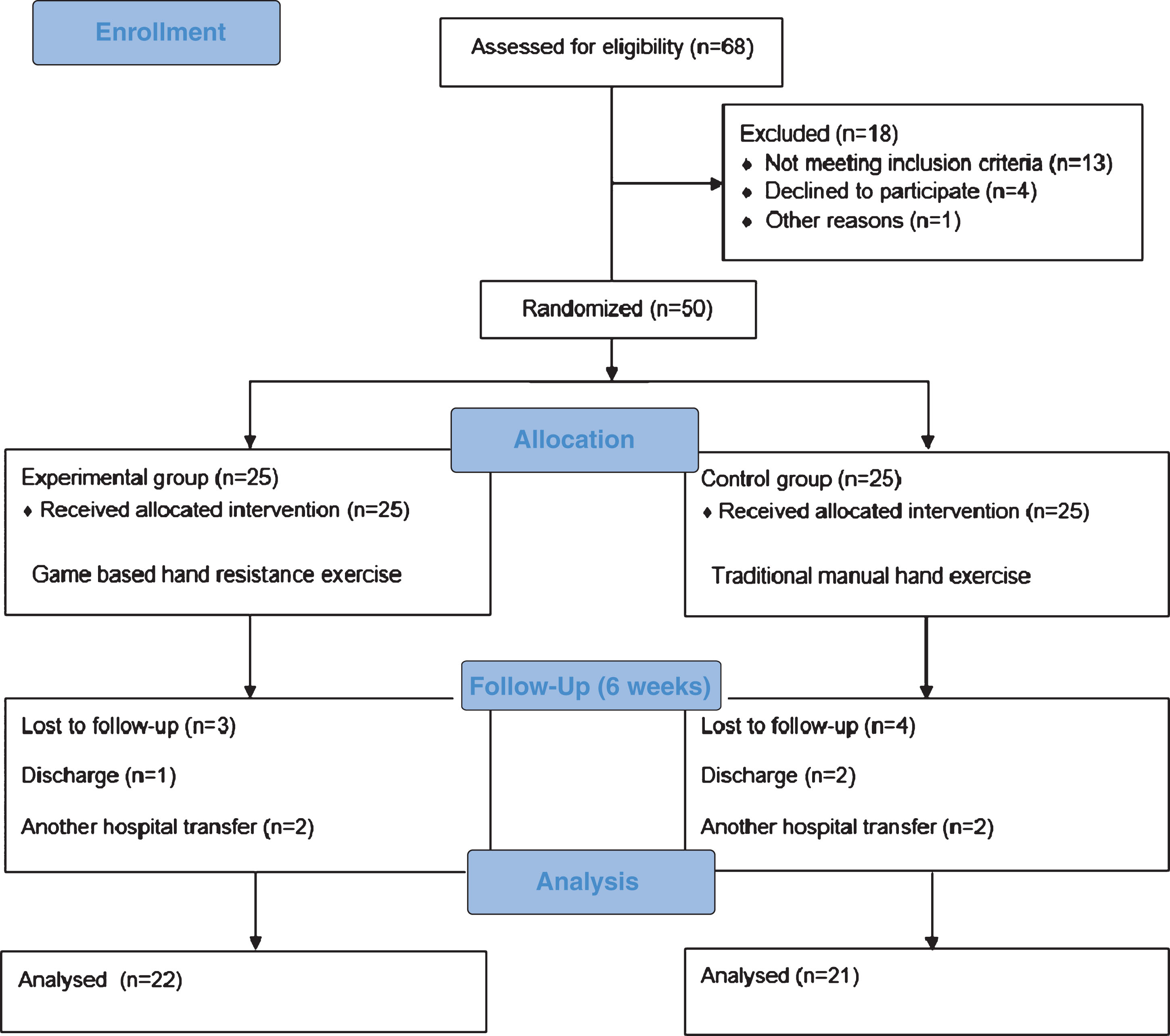
Flow chart of this study.
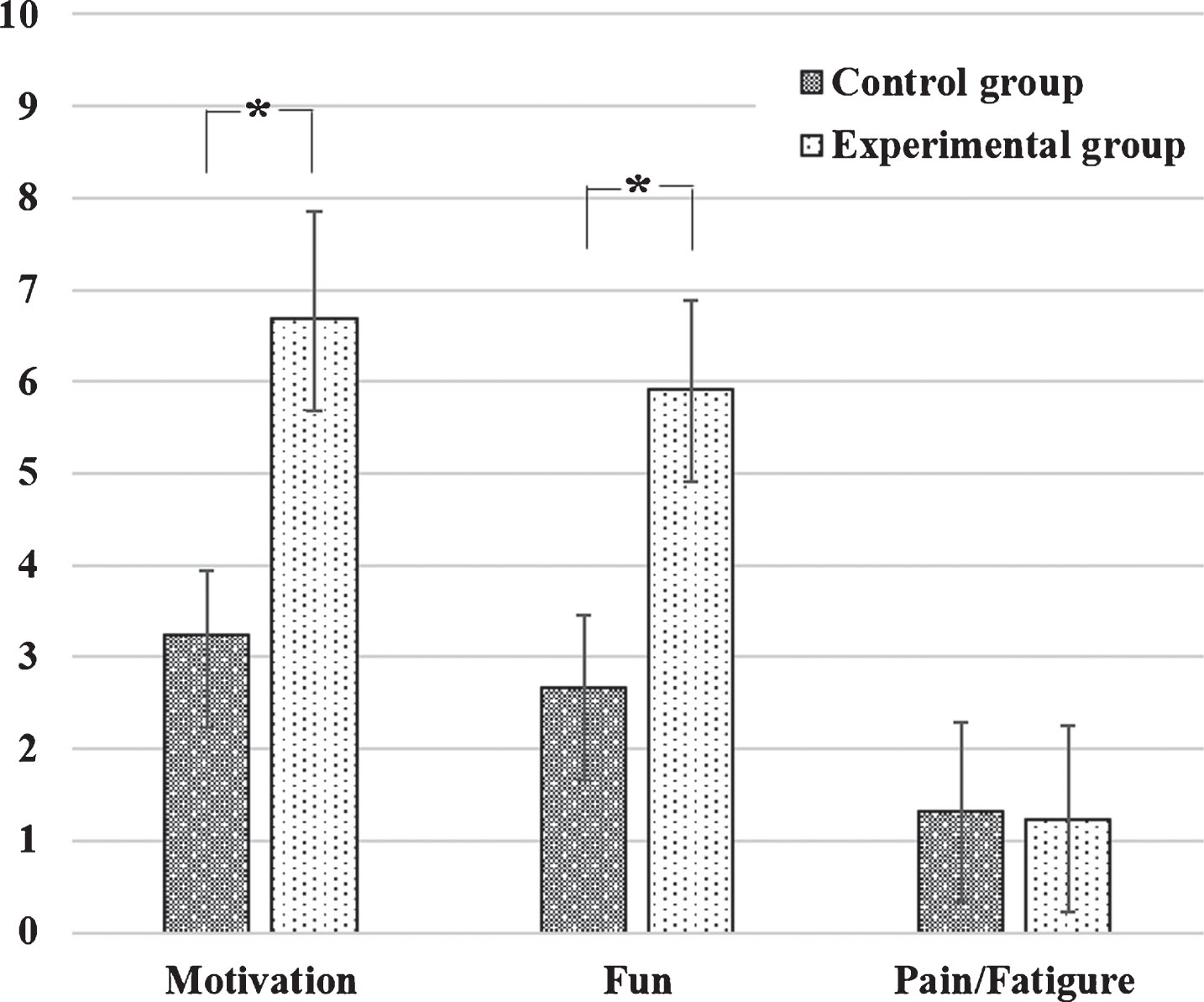
Subject-based report of motivation, fun, and fatigue/pain on a 0–10 numeric rating scale for different groups. A significant difference was found between groups with respect to motivation and fun (p < 0.001) in contrast to fatigue/pain (p = 0.728). Values are expressed as mean±standard deviation.
A summary of the clinical and demographic features of the subjects (n = 45) is shown in Table 1. The homogeneity test of each measurement item showed no significant differences in baseline characteristics between the groups (p > 0.05) (Table 1).
Characteristics of participants
Values are expressed as mead±standard deviation.
After intervention, both groups showed statistically significant improvement in hand grip strength (P < 0.001). Comparing the two groups after the intervention, the experimental group showed more improvement in hand grip strength than the control group (P = 0.041) (Table 2). In a comparison of the amount of change in the groups, both groups showed significant differences in hand grip strength (p < 0.001) (Table 3). Effect sizes were observed 0.93 for the hand grip strength
Changes in parameters before and after treatment
Changes in parameters before and after treatment
Mean±standard deviation. *p < 0.05 by paired t test, †p < 0.05 by independent t test. HST, hand strength test; BBT, box and block test; MFT, manual function test; ES, effect size.
After intervention, both groups showed statistically significant improvement in BBT and MFT (P < 0.001). Comparing the two groups after the intervention, the experimental group showed more improvement in BBT and MFT than the control group (P = 0.042 and 0.036) (Table 2). In a comparison of the amount of change in the groups, both groups showed significant differences in BBT and MFT (p = 0.003 and 0.004) (Table 3). Effect sizes were observed 0.87 and 0.39 for the BBT and MFT.
Comparison of the differences after the 6-week treatment in the two groups
Comparison of the differences after the 6-week treatment in the two groups
Mean±standard deviation. †p<0.05 by independent t test. HST, hand strength test; BBT, box and block test; MFT, manual function test.
There were significant differences between groups with respect to subject-based reports of motivation and fun (p < 0.001) but not pain/fatigue (p = 0.728) (Fig. 4).
Discussion
This study investigated the effect of game-based hand resistance exercise using Table PC on hand strength and motor function in stroke patients with hemiplegia. We demonstrated that game-based hand resistance exercise was more effective for improving hand strength, motor function, and provided more fun and motivation than traditional manual exercise.
This is probably for several reasons: First, game-based exercises improve the effectiveness of resistance training more than manual therapy by providing systematic resistance values. The resistance value is one of the most important factors in resistance training. It is therefore important to provide appropriate resistance values continuously. Even though there are some differences in published studies, it is generally recommended that resistance training should be employed in treatment of neurological diseases by applying 70–80% of 1-RM values (Borde et al., 2015). If intensity of resistance is small, such as with no resistance or 10–20% of 1-RM, the exercises cannot induce physiological changes in muscles, and it is difficult to expect effects such as muscle hypertrophy or muscle strength increases. Conversely, if resistance intensity is too large, as with 100% of 1-RM, the patient is exposed to muscle fatigue; not only can the exercise not be repeatedly performed, but it also causes discomfort or temporary pain. Therefore, we applied resistance of 70% of 1-RM for effective and effective resistance training. Conversely, the resistance of traditional manual hand exercise for the patient was very subjective; that is, the degree of resistance depended on various factors such as the therapist’s clinical experience, physical ability, and gender. Therefore, traditional manual hand exercise does not guarantee effective resistance.
Second, game-based exercises are goal-directed, and repetitive training uses visuo-auditory feedback (Choi et al., 2014). Game-based training is exercise that requires effort to reach target values set in real time through visual feedback. Choi et al. (2016) reported that task-oriented/goal-directed exercise is more effective in improving motor function than conventional exercise in post-stroke patients. Because goal-directed exercise provides motivation, it helps to maintain constant concentration during exercise. Focusing on activity during exercise increases excitability of the motor-related area of the cerebral cortex (Eryilmaz et al., 2017). As a result, activation of the cerebral cortex has a positive effect on brain plasticity. The theoretical evidence supports the results of this study.
Visuo-auditory feedback in rehabilitation could have positive effects on repeated motor control and learning because it allows us to visualize and correct errors immediately. This is because it is important for functional movement that exercise learning be obtained through the repetitive execution of the exercise; at this time, it is possible to provide continuous feedback and opportunities to correct or reduce errors by oneself (Lee et al., 2017; Saposnik et al., 2010). Therefore, game-based training is a method that can reduce motion errors to a relatively greater extent than manual therapy and to perform it through accurate movement.
Finally, game-based exercises can stimulate motivation, fun, and interest for the patients, contributing to more active participation, in turn increasing patient compliance. The game programs induce pleasure and interest in the rehabilitation therapy, thereby acting positively to promote motor learning (Lee et al., 2017). The games also inspire, motivate, and trigger pleasure and interest in rehabilitation by utilizing the player’s intrinsic sense of competition and desire for interaction, thereby promoting learning movements. It provides interactive stimulation and feedback, both of which are fundamental to motor skill learning (Adams et al., 1972). In addition, higher motivation and active participation has been associated with better rehabilitation outcomes (Merians et al., 2002). Repetitive resistance exercise can be challenging activity and tedious work for the patient. By contrast, games have the advantage of motivation and active participation in activities by creating fun and interest while receiving audio-visual feedback. Therefore, we believe that game-based training has a positive impact on encouraging the participation of activities such that it can be actively trained.
Conclusion
In conclusion, we demonstrated that game-based exercise is more effective than manual exercise in improving muscle strength, motor function, and compliance in stroke patients.
Conflict of interest
The authors claim no conflicts of interest
Footnotes
Acknowledgment
This work was supported by Dongseo University, “Dongseo Cluster Project” Research Fund of 2019 (DSU-2019002).