
Abstract
BACKGROUND:
Few previous studies have assessed self-perceived functioning, disability and recovery after electromechanically-assisted gait training (EAGT).
OBJECTIVE:
To compare self-perceived functioning, disability and recovery after EAGT and after conventional gait training in the subacute stage after stroke, using the Stroke Impact Scale (SIS), and factors associated with self-perceived recovery, assessed at 6 months after stroke.
METHODS:
Patients were randomized into two groups performing a 4-week intervention period of incorporated EAGT using the Hybrid Assistive Limb (HAL) or conventional physiotherapy only.
RESULTS:
There were no significant differences in self-perceived strength, ADL, mobility, participation and percentage of recovery between intervention groups (p > 0.05). Self-perceived mobility was associated with improvements in objectively assessed walking speed/endurance and balance (R2 0.717, p = 0.002), and self-perceived recovery with self-perceived activities of daily living (ADL) ability (R2 0.34, p = 0.001).
CONCLUSIONS:
This study indicates that EAGT and conventional gait training in the subacute stage after stroke have no differential impact on self-perceived functioning, disability and recovery at 6 months after stroke. Further, the study highlights the importance of interventions targeting ADL and self-care independence during stroke rehabilitation to enhance self-perceived recovery and clinical aspects to be targeted to enhance perceived mobility.
Introduction
Many stroke survivors experience long-term impairment and activity limitations. In a Swedish study about 1/3 of stroke survivors report limitations in self-care, domestic life and community, and social and civic life at 3 months after stroke onset (Alguren, Lundgren-Nilsson, & Sunnerhagen, 2010). At one year post stroke, 29% were still unable to return to the life and activities they had before the stroke and 24% were still dependent in personal activities of daily living (ADL) such as toileting, dressing and/or mobility (“Riksstroke The Swedish Stroke Register”).
During inpatient rehabilitation, a common goal is recovery of independent mobility, including gait (Dobkin, 2005). This has led to a growing field of novel technologies, such as electromechanically-assisted gait training (EAGT), aiming to enhance the dose and intensity of gait training in the subacute stage after stroke. In previous studies of EAGT improvements in independence in walking were found (Mehrholz et al., 2017; Watanabe, Tanaka, Inuta, Saitou, & Yanagi, 2014). However, the additional beneficial effect of such training compared to conventional gait training after stroke is not clear. Moreover, since improved mobility may improve self-care ability (Peurala, Karttunen, Sjogren, Paltamaa, & Heinonen, 2014; Veerbeek et al., 2014) an essential aspect in need of further exploration is potential transfers of regained functions to everyday life activities after EAGT and conventional training (Mehrholz et al., 2017). Particularly among younger individuals (i.e. those in working age), persisting limitations and restrictions in ADL after stroke might have a vast and lifelong impact on major life areas (Teasell, McRae, & Finestone, 2000). In addition, mobility and ADL ability might affect how people rate their recovery from stroke (Duncan et al., 1999).
To investigate the effect of EAGT after stroke, previous studies have used objective, clinical assessments of the patient’s impairments, limitations and restrictions. However, data on self-perceived functioning and disability in everyday life as well as self-perceived recovery in studies using EAGT in general and the exoskeleton Hybrid Assistive Limb (HAL) in particular are scarce (Geroin et al., 2013; Mehrholz et al., 2017; Yilmaz et al., 2018).
Thus, our aim was to explore long-term effects (6 months after stroke onset) of EAGT (here performed with the HAL exoskeleton) compared to conventional gait training in the subacute stage after stroke, regarding self-perceived functioning, disability and recovery and factors associated with self-perceived recovery assessed at 6 months after stroke. Specific research questions were: Are there any between-group differences in self-perceived: 1) strength, 2) ADL, 3) mobility, 4) participation and 5) recovery, at 6 months post stroke? Can self-perceived: 1) mobility and 2) recovery be explained by patient characteristics or improvements in objective clinical outcomes from baseline to 6 months post stroke and are there any differences between groups? Is the degree of self-perceived recovery associated with and explained by self-perceived ratings of 1) strength, 2) ADL, 3) mobility and/or 4) participation?
Materials and methods
Design
The present study is part of a prospective, randomized, open labeled, blinded evaluation (PROBE) study conducted between February 2014 and May 2017. The PROBE-study, investigating the potentially added benefit from EAGT on objective clinical outcomes such as independence in walking, walking speed and balance will be presented in detail elsewhere. In the present study we focused on the patients self-perceived functioning, disability and recovery assessed with the Stroke Impact Scale (SIS) at 6 months post stroke. The study was conducted at the University Department of Rehabilitation Medicine Stockholm at Danderyd Hospital, Sweden, where patients aged 18–67 years underwent team based inpatient rehabilitation in the subacute stage after stroke. The study was approved by the Regional Ethical Committee of Stockholm (2013/1807–31/2) and (2014/1267–32). All participants expressed informed consent and the study was performed in compliance with Good Clinical Practice and the Declaration of Helsinki. The full study protocol can be found on ClinicalTrials.gov Identifier: NCT02410915.
Participants
The inclusion criteria for the main study were:≤8weeks since onset of ischemic or hemorrhagic stroke (verified by CT and/or MRI); hemiparesis; inability to walk or in need of continuous manual support to walk (i.e. Functional Ambulation Categories (Holden, Gill, Magliozzi, Nathan, & Piehl-Baker, 1984) (FAC) score 0–1); the ability to maintain a sitting posture with or without supervision for >5 minutes; sufficient postural control to allow upright position in standing with aids and/or manual support; the ability to understand training instructions as well as written and oral study information in order to express informed consent; and a body size compatible with the HAL suit. Exclusion criteria were cerebellar stroke, primary subarachnoid bleeding, contracture restricting gait movements at any lower limb joint, cardiovascular or other somatic condition incompatible with intensive gait training, and/or severe contagious infections.
Interventions
Patients were randomized into 2 groups performing a 4-week intervention period. Both groups received conventional team-based training (CTBT) by a multidisciplinary team consisting of physiotherapists, occupational therapists, speech and language therapists, physicians, nurses and healthcare assistants, and following current best practice for inpatient rehabilitation after stroke. One group performed CTBT including conventional physiotherapy only (CONV group) and the other group performed CTBT including EAGT using HAL (Kawamoto, 2002) incorporated with conventional physiotherapy (HAL group). Training with HAL was individualized and incorporated in the CTBT 4 days per week during the 4-week intervention period (i.e. 16 sessions in total). The control method of HAL (Kawamoto, 2002; Suzuki, Mito, Kawamoto, Hasegawa, & Sankai, 2007) and the full intervention protocol are described in detail elsewhere (ClinicalTrials.gov Identifier: NCT02410915) and is therefore only briefly outlined here. After the intervention period CTBT continued in both groups until discharge. The rehabilitation performed from discharge to the 6 months follow up assessment was not monitored. However, the referrals to rehabilitation after discharge from inpatient care in the Stockholm region are provided as part of the care and rehabilitation trajectory and may include home based rehabilitation and/or interventions in an out-patient clinic.
Assessments
A blinded physiotherapist experienced in stroke rehabilitation performed the assessments at three time points: before and after the 4-week intervention (T1 and T2) and at 6 months post stroke onset (T3). In the present study we report the results from T1 and T3.
The clinical assessment used at T1 and T3 comprised the Fugl-Meyer Assessment for control of voluntary movement in the lower extremity (FMA-LE Motor) (motor function domain, 0–34 points), the Functional Ambulation Categories (FAC) for independence in walking (0–5) (Holden et al., 1984), the 2-minute walk test at self-preferred speed (2 MWT) (Kosak & Smith, 2005), the Bergs Balance Scale (BBS) (0–56 points) (K. Berg, Wood-Dauphinee, Williams, & Gayton, 1989; K. O. Berg, Maki, Williams, Holliday, & Wood-Dauphinee, 1992) and the Barthel Index for dependence in activities of daily living (BI) (0–100 points) (Mahoney & Barthel, 1965). A blinded senior consultant assessed stroke severity at T1 using the NIH Stroke Scale (NIHSS) (0–42 points) (Lyden et al., 1994).
At T3 study participants responded to the Swedish version of the SIS (version 3.0) which assesses self-perceived functioning, disability and recovery after stroke through questions divided into domains. For the present study the domains used were: strength (domain 1), ADL (domain 5), mobility (domain 6), and participation (domain 8). The questions were responded to using a 5-point Likert scale. For strength from “no strength at all” to “a lot of strength”; for participation from “none of the time” to “all of the time”; and for the other domains from “extremely difficult/cannot do at all” to “not difficult at all”. A summary score of each domain is calculated using an algorithm (((mean -1)/(5–1))*100)) resulting in a minimum score of 0 points (maximum disability) and a maximum score of 100 points (no disability). We also used domain 9, a visual analog scale where self-perceived percentage of recovery is rated, from 0 (no recovery) to 100 (maximum/full recovery). (Duncan, Bode, Min Lai, & Perera, 2003; Duncan et al., 1999). The SIS is developed with input from patients with stroke, caregivers and health professionals (Duncan, Bode, et al., 2003), is reliable and valid (Duncan, Bode, et al., 2003; Duncan et al., 1999) and have previously been found to capture persisting consequences of stroke (Lai, Studenski, Duncan, & Perera, 2002) by assessing a broader description of performance in everyday life and perceived health, beyond impairment.
Primary outcome
The primary outcome for the present study was the SIS mobility domain.
Secondary outcomes
The secondary outcomes were the SIS strength-, ADL- and participation domains and the SIS self-perceived recovery domain.
Statistics
All calculations were performed in SPSS (IBM SPSS Statistics 25) with significant levels set to p < 0.05 (two-tailed) and data analyzed as an all-available-data analysis. Normality were examined using Shapiro-Wilk’s test, skewness, boxplots and histograms.
Between groups differences for gender, diagnosis, and paretic side were tested with the Chi-square test/Fisher’s exact test; for days from stroke to inclusion with the Independent sample t-test; and for age, stroke severity with the Mann-Whitney U-test.
Between groups differences for objective clinical assessments were tested with the Mann-Whitney U-test, and for the SIS-domains strength, ADL, mobility, participation and percentage of recovery the Independent t-test were used.
Associations were computed for the whole (merged) group using Pearson’s Correlation. Partial correlation was performed (one by one) controlling for group and baseline characteristics (age, diagnosis, paretic side, days to inclusion and stroke severity). Correlations were interpreted as ≤0.25: little or no relationship, 0.25–0.50: fair, 0.50–0.75: moderate to good, and ≥0.75: very good to excellent relationship (Colton, 1974). Variables with rp >0.3 were included in a stepwise linear regression model with the mobility- and recovery domain as dependent variables. To check for multicollinearity the variance inflation factor (VIF) was examined (were VIF < 4 was considered as no multicollinearity).
Results
Participants
Of 33 included patients, who completed the intervention period, two patients were lost to follow up (at T3), both in the CONV group (due to private or to medical reasons). In total 31 patients performed the 6 months follow up, 16 in the HAL group and 15 in the CONV group. Another 3 patients were excluded from the analysis due to aphasia (n = 1), cognitive impairments (n = 1) or incomplete answers (n = 1) resulting in 28 patients being analyzed in the present study (Fig. 1).
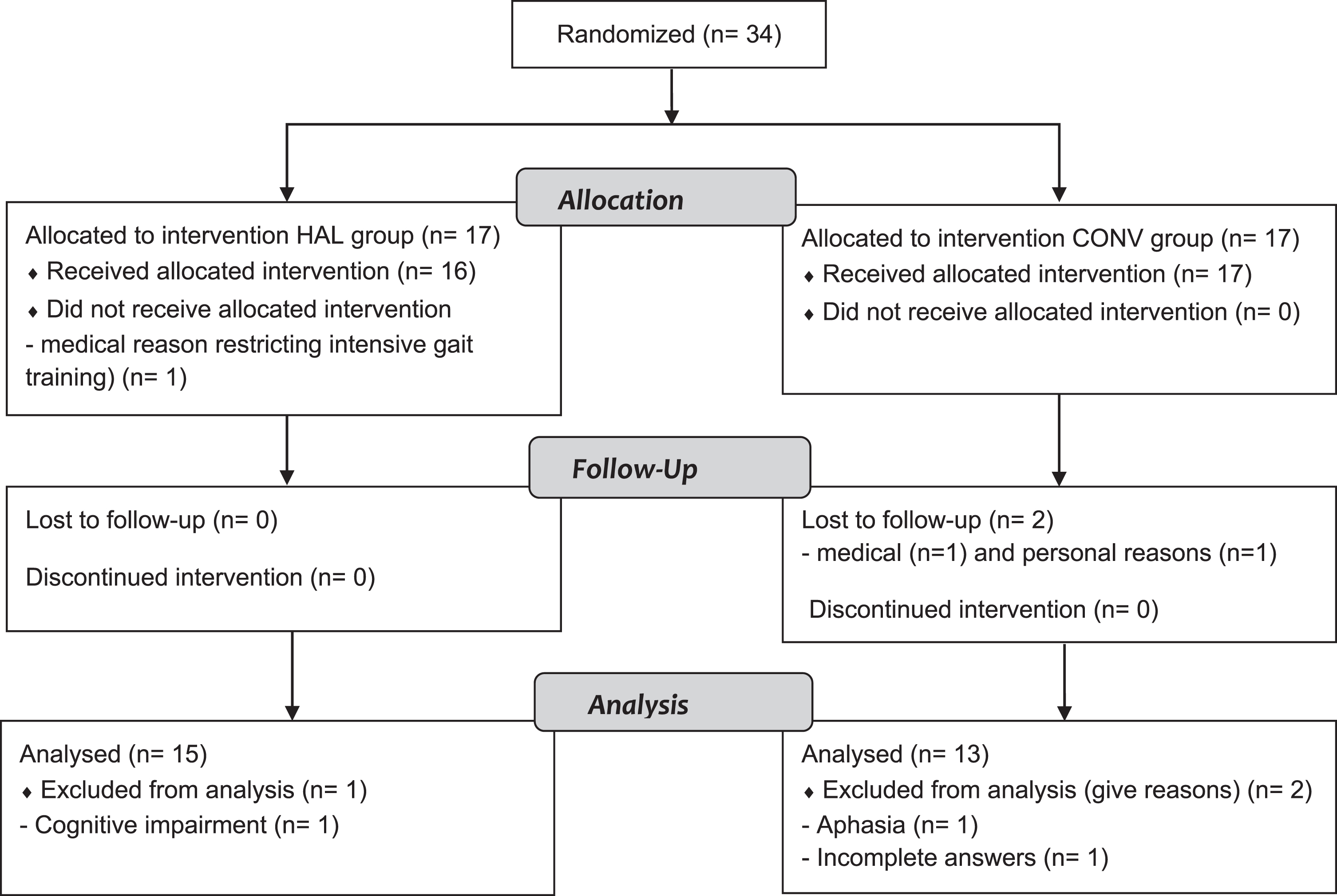
CONSORT flow chart. HAL: HAL group, CONV: Conventional group, T1: baseline assessment, FAC: Functional Ambulation Categories.
Mean age for the whole group was 53 years (SD 12). Most patients were men (82%). Patients were categorized as having moderate severe stroke according to median baseline NIHSS scores as well as ADL ability according to BI (HAL group 35 (IQR 30;50), CONV group 35 (IQR 30; 42.5) (Govan, Langhorne, & Weir, 2009). Most patients (71%) had no functional walking ability (FAC score = 0) at inclusion, all others scored FAC 1. At baseline there were no significant differences (p > 0.05) between the two groups (Tables 1 and 2).
Patient characteristics at baseline (T1)
HAL: HAL group, CONV: Conventional group, NIHSS: NIH Stroke Scale. Values presented as Mean (SD) or Median [IQR]. *Skewed.
Clinical assessments before the intervention (T1), at 6 months post stroke (T3) and change from baseline to 6 months (ΔT1-T3)
HAL: HAL group, CONV: Conventional group, FMA-LE Motor: Fugl-Meyer Assessment Lower Extremity Motor domain, FAC: Functional Ambulation Categories, 2MWT: 2 Minute Walk Test, BBS: Berg Balance Scale, BI: Barthel Index. Values presented as Median [IQR]. P-value for between group differences.
In addition, there were no significant differences in objective, clinical assessments at T3 between the groups. Neither was there any significant difference in the change scores (Δ) T1-T3 between groups (Table 2). At 6 months post stroke, most patients (68%, n = 19/28) were independent in walking (FAC≥4) and in ADL (57%, n = 16/28) (BI≥90) (Celani, Cantisani, Righetti, Spizzichino, & Ricci, 2002).
Mean (SD) length of stay at the inpatient rehabilitation ward was similar in both groups (HAL group 84 (21); CONV group 84 (16) days). After the inpatient rehabilitation period all patients (n = 15) in the HAL group were discharged to their home but dependent on assistance in personal care and/or domestic life. In the CONV group the corresponding number were seven, whereas three were discharged to their home without assistance, and another three to nursing homes.
For both groups the lowest median scores (highest perceived impact) were found in the strength and participation domains. There were no significant differences in self-perceived strength, ADL, mobility, participation or percentage of recovery between intervention groups (p > 0.05) (Table 3).
Self-perceived Strength, ADL, Mobility, Participation and Recovery at 6 months post stroke (T3)
Self-perceived Strength, ADL, Mobility, Participation and Recovery at 6 months post stroke (T3)
P-value represents between group differences. HAL: HAL group, CONV: Conventional group, SIS: Stroke Impact Scale. Values presented as Median [IQR] and Actual range. A score of 0 points means maximum disability/*no recovery and a score of 100 points no disability/*full recovery.
Self-perceived mobility was significantly and fairly correlated with baseline stroke severity (NIHSS T1) and correlation with change in voluntary movements in LE (FMA-LE Motor ΔT1-T3) and independence in walking (FAC ΔT1-T3) was moderate to good. Correlation with change in walking speed/endurance (2 MWT ΔT1-T3) and balance (BBS ΔT1-T3) was very good to excellent. All correlations persisted after controlling for group and baseline characteristics (age, diagnosis, paretic side, days to inclusion and stroke severity), see Table 4.
Associations between patient characteristics, change in clinical assessments and SIS domain scores, and the Mobility and Recovery domains of SIS
Expressed as Pearson’s correlation. *p-value < 0.05. T1 = baseline, T3 = 6 months post stroke. Binary variables were coded as follows: Conventional group = 0, HAL group = 1, male = 1, female = 2, haemorrhage = 1, infarct = 2, left = 1, right = 2.
For self-perceived recovery a fair and significant correlation was found with change in objectively, clinically assessed ADL (BI ΔT1-T3) and a moderate to good and significant correlation with self-perceived ADL according to SIS, all others are non-significant. All correlations persisted even after controlling for group and baseline characteristics (age, diagnosis, paretic side, days to inclusion and stroke severity), see Table 4.
Regression equations are found in Table 5. Multiple regression using stepwise method found change in walking speed/endurance (2 MWT ΔT1-T3) and balance (BBS ΔT1-T3) explaining 72% of the variance in self-perceived mobility (p = 0.002). The variance in self-perceived recovery was explained by change in objectively assessed ADL (BI ΔT1-T3) (Adj R2 0.129, p = 0.034) as well as by self-perceived ADL (R2 0.342, p = 0.001).
Linear regression for factors explaining self-perceived Mobility and Recovery
Dependent variable = Self-perceived mobility and self-perceived recovery; Adj = Adjusted, CI = Confidence interval, SIS = Stroke Impact Scale.
When examining the items included in the ADL domain of SIS we found that items regarding: getting to the toilet on time (rp 0.684), controlling the bladder (rp 0.571) and controlling the bowels (rp 0.566) had the strongest association with self-perceived recovery (all p < 0.01).
In this exploratory study, patients’ self-perceived functioning, disability and recovery after EAGT and after conventional gait training alone were not significantly different when provided as part of conventional team based in-patient rehabilitation at a regional department for specialized neurorehabilitation in the subacute stage after stroke. Both objectively assessed (BI) change in and self-perceived (SIS) functioning in ADL were found to be important factors for self-perceived recovery, and the degree of clinically assessed improvements in walking speed/endurance and balance influenced self-perceived mobility at 6 months post stroke.
To our knowledge there are few previous studies assessing self-perceived functioning, disability and recovery after EAGT. One study (Chua, Culpan, & Menon, 2016) assessed self-perceived functioning using SIS (physical, memory, emotions, communication, participation and recovery domains) after 8 weeks of EAGT in combination with conventional physiotherapy, compared to conventional physiotherapy alone in non-ambulatory (FAC 0–2) patients in subacute stage after stroke (1 months). Corroborating our results, they found no between-group differences in any of the included SIS domains over time (follow up until 48 weeks). At 6 months follow up (7 months post stroke) the self-perceived recovery ratings were higher than in the present study (in mean 65 (SD 21) and 61 (SD 21) for the EAGT and conventional group respectively), yet their study participants were older than ours (mean age 61 (11)).
Moreover, in other studies with stroke patients of older age (in mean between 60 and 73 years of age) the ratings in the SIS domains strength, ADL, participation and recovery are in line with or slightly higher than in the present study (Baer, Salisbury, Smith, Pitman, & Dennis, 2018; Duncan et al., 2011; Duncan et al., 1999; Nichols-Larsen, Clark, Zeringue, Greenspan, & Blanton, 2005) at 3–9 months post stroke. However, despite the more severe limitations in mobility at inclusion in the present study, the mobility-rating has been found to be similar (Duncan et al., 2011; Nichols-Larsen et al., 2005) or somewhat lower (Duncan et al., 1999) than in the present study.
Given the older age of participants in previous studies (Baer et al., 2018; Duncan et al., 2011; Duncan et al., 1999; Nichols-Larsen et al., 2005) the lower scores in self-perceived recovery in the present study could be explained by our study participants being younger. One could speculate that at younger, working age, the requirements for life and expectations of functioning and recovery are different than in older age (Palmcrantz et al., 2012) making lower scores more likely in our study population. This reasoning emphasizes the need to use both self- perceived and objective, clinical assessments to set rehabilitation goals and evaluate outcome.
In contrast to previous studies on EAGT, most often using objective assessments of functioning and disability, the present study also assessed self-perceived aspects that has been considered relevant by patients and caregivers, by use of the SIS. The SIS-ratings are subjective and the impact of stroke on a person’s health and life may differ between patients with the same objective functioning and disabilities. The SIS-ratings may to some extent also reflect cognitive skills, degree of acceptance, apprehension and/or denial of once life situation, including disabilities. Therefore, the self-perceived ratings offer an additional perspective that is not captured with objective, clinical and commonly used outcome measures. Interestingly, in the present study sample, objectively assessed improvements in outcomes were found to be associated with the self-perceived ratings. Thus, in this younger group with severe limitations still in the subacute phase after stroke, the improvements identified with clinical measures appear to influence self-perceived recovery and mobility at 6 months post stroke. These results imply that FMA-LE Motor, FAC, 2MWT, BBS and BI capture aspects of mobility that are perceived as important to this patient group and should be used throughout the care trajectory.
Self-perceived mobility
The items in the mobility domain include different aspects of balance, walking speed and endurance, identified as important by clinicians and persons living with stroke, in the development of the SIS (Duncan et al., 1999). Notably, in the present study, with young participants with initially severe limitations in mobility, the objectively assessed changes in outcomes related to walking and balance were in concordance with the self-perceived ratings of mobility at 6 months. These results emphasize the importance of targeting and providing interventions to limit these restrictions. In line with these findings and suggested interventions, balance has previously been found to be one important determinant of self-perceived mobility after stroke (Chen et al., 2015) and has been suggested important to improve walking independence (Kollen, van de Port, Lindeman, Twisk, & Kwakkel, 2005) and speed/endurance (Patterson et al., 2007). Improvements in walking speed from <0.4 m/s (household ambulator) to >0.4 m/s (and thereby transitioning to a higher class of ambulation according to Perry et al. (Perry, Garrett, Gronley, & Mulroy, 1995) have previously been found to be associated with higher self-perceived mobility and participation after stroke (Schmid et al., 2007). Nonetheless, walking distance requirements to be able to ambulate in the community may vary depending on the person’s life situation (Salbach et al., 2014) and environmental demands. This might explain the wide range in self-perceived mobility (range 31–100) in the present study. Thus, gait training and goal setting must be individualized with regard to each person’s everyday life requirement (e.g. distance) and performed in alike environments.
Self-perceived recovery
In the present study sample, we found that self-care and domestic life ability were the factors with strongest associations with self-perceived recovery at 6 months. Among the items in the ADL domain of SIS, getting to the toilet in time, a fundamental ability, was most strongly related to self-perceived recovery.
Duncan et al. (Duncan et al., 1999) previously found that self-perceived stroke recovery can be predicted by “Physical function” (a combination of strength, hand function, mobility and ADL domains), emotion and participation, together explaining 45% of the variance. However, the Barthel Index alone explained 33%, which is comparable to the 34% explained by self-perceived ADL (according to SIS) in the present study sample. This highlights the importance of activities aiming to improve ADL and self-care independence during stroke rehabilitation. In the Swedish National Board of Health and Welfare Guidelines for Stroke Care, training of ADL-related activities is highly recommended within the first 6 months post stroke. Notably the recommendation is stated as important after discharge from hospital. A majority of patients in the present study improved in BI during the intervention period and until the 6 moths follow up assessment. Nevertheless, 79% of the patients were discharged home with assistance in self-care and/or domestic life and at 6 months post stroke 43% were still considered dependent in ADL (i.e. BI < 90). This highlights the importance of ADL practice both during and after discharge. Targeting and providing evidence-based training to those with impaired ADL ability after stroke might be effective to promote self-perceived recovery. Whether enough effort is put into this training during the subacute, inpatient rehabilitation phase can be questioned and should be explored further.
During team-based stroke rehabilitation most ADL-training, in particular training in self-care, is carried out by the occupational therapists and assistant nurses. Studies have found that working in multidisciplinary team and using a client-centered approach in ADL-training are favorable for change in ADL task performance and participation in everyday life during the first year (Langhammer et al., 2017) especially in moderate to severe stroke (Gustavsson, Guidetti, Eriksson, von Koch, & Ytterberg, 2019). As for motor training during the recovery phase after stroke, ADL-training should include high-intensity, repetitive, task-specific practice (Langhorne, Bernhardt, & Kwakkel, 2011), and interventions should aim to improve ADL task performance (functioning) rather than adopting environmental adaptations (compensating). There are evidence supporting several interventions to improve ADL task performance during inpatient rehabilitation (Wolf, Chuh, Floyd, McInnis, & Williams, 2015). The training should be individualized including goal-directed and repetitive practice of a particular task and, if necessary combined with cognitive strategies (Nilsen et al., 2015). Providing occupational therapy training in the home setting before (and after) discharge has also been suggested to facilitate the ability to transfer skills to the patient’s home (i.e. generalization) (Rasmussen et al., 2016).
Physiotherapy interventions to improve mobility and walking independence are common in early stroke rehabilitation. Based on the results from the present study we propose that attention also should be paid at improving movement performances related to ADL and self-care activities (such as transferring oneself explicit to the toilet). Identifying the task-specific, movement-related components that are difficult for each patient should also support the planning and execution of training, involving all team members to provide enough intensity and repetitions in order to promote recovery.
The R2 values in the present study indicate that there are other factors than those measured that contributes to the variability of the self-perceived recovery-score. In a previous study, in which self-perceived recovery was assessed at 1-year post stroke, the variance among younger individuals (<65 years, median 55 years) was explained by the domains hand function and emotions (explaining 39% together) with only 20% explained by dependence in ADL (Palmcrantz et al., 2012). The hand function and emotion domains were however not included here, since mobility and walking were at focus of this study but might of course influence the self-perceived recovery in our relatively young study sample. Hand function has also been reported to be one of the domains with most perceived problems both 3- and 12-months post stroke (Guidetti, Ytterberg, Ekstam, Johansson, & Eriksson, 2014).
In addition, self-perceived recovery changes over time and have been found to increase up to 1 year post stroke (Duncan et al., 1999; Guidetti et al., 2014) but with no further improvement between 1 to 6 year post stroke (Ytterberg, Dyback, Bergstrom, Guidetti, & Eriksson, 2017). Furthermore, factors explaining perceived health outcome (assessed with EQ5D) may be explained by different aspects at different time points after stroke (Alguren, Fridlund, Cieza, Sunnerhagen, & Christensson, 2012; Richardson, Campbell, Allen, Meyer, & Teasell, 2016). Algurén et al. (Alguren et al., 2012) found that restrictions in body functions, activities and participation explained most of the variance in rated health at 6 weeks and 3 months post stroke, however at 1-year environmental factors became more important. In agreement, Richardson et al. (Richardson et al., 2016) found that self-perceived participation became more important for self-perceived health outcome over time; whereas “Physical function” (combined strength, ADL, mobility and hand domain) was found important/to contribute to self-perceived health across all time points (0, 6, 12 months) within the first-year post stroke in people who received home-based rehabilitation.
These changes in factors contributing to self-perceived recovery and health outcome over time might reflect that patients more easily identified problems in self-care and/or participation after discharge from hospital when back in their everyday life. It is possible that the importance of participation for self-perceived recovery becomes more important when basic functioning like mobility and self-care is improved, explaining the lack of association between the participation domain and self-perceived recovery in our study sample. This suggests that the rehabilitation focuses also must change over time.
The fact that neither self-perceived nor change in objectively assessed mobility was significantly associated with self-perceived recovery at 6 months post stroke in our study sample might be explained by the majority (68%, n = 19/28) of patients being independent in walking at 6 months.
Limitations
In the present study we did not include all SIS domains making it possible that other domains than those measured are explaining some of the variance in self-perceived recovery. However, for patients in the present study we considered it too strenuous for the patients to respond to all items included in the SIS. Future studies may consider using the shorter SIS-16 version (Duncan, Lai, Bode, Perera, & DeRosa, 2003). Still, neither of the SIS-scales cover all aspects of stroke recovery and problems after stroke such as fatigue (Tistad, Ytterberg, Tham, & von Koch, 2012) depression and pain (Carod-Artal & Egido, 2009).
Power was primarily calculated for the main study evaluating walking independence. However, using SIS as the primary outcome measure and with an alpha value of 0.05, the expected difference between treatment groups needed to be 15 points in mean (SD 15), for the planned 18 patients in each group to get a power of 80%. Thus, the small differences between groups and great variances within groups together with fewer patients resulted in lack of power.
Our study sample is not representative for the whole stroke population since they are younger than the mean age at stroke onset (“Riksstroke The Swedish Stroke Register”). The distribution of gender and lesion side were also unbalanced. In addition, we have no data on rehabilitation performed from discharge to the 6 months follow up assessment, yet most of the patients were discharged to their homes and therefor continued training with home-rehabilitation team and/or with allied health care professionals in out-patient care.
Conclusion
In the present study four weeks of additional HAL training did not significantly affect self-perceived functioning, disability and recovery when compared to conventional gait training. Despite no between-group differences, the present study provides new insights related to performance in everyday life and perceived health after EAGT. We found self-perceived ADL ability to be the most important factor for self-perceived recovery at 6 months, explaining 34% of the variance. Thus, interventions targeting ADL and self-care independence might reduce the perceived impact of stroke.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of interest
The authors have no conflicting interests to declare connected to the conducted research.
Footnotes
Acknowledgments
This work was supported by the Promobilia Foundation; Stroke-Riksförbundet; NEURO Sweden; the Norrbacka-Eugenia Foundation and a donation by Lars Hedlund (Karolinska Institutet Dnr 2-1582/2016). The authors would like to acknowledge Ph.D. Katarina Vreede and Associate Professor Disa Sommerfeld for their contribution to this work.