
Abstract
INTRODUCTION:
Evidence indicates that motor deficits in hemiplegic cerebral palsy (HCP) impair both motor execution and planning. However, current rehabilitation efforts focus mainly on relieving impairments in motor execution. Motor imagery (MI) is a promising method for stimulating neural networks underlying the planning and control of movements.
OBJECTIVE:
Evaluate the effectiveness of MI combined with physical practice in improving the function of the upper limbs in children with HCP.
METHOD:
Twenty-four participants, aged 7–14 years were divided into two groups: intervention group (IG) and control group (CG). The IG was subjected to MI training and physical practice twice a week for eight consecutive weeks, while the CG received conventional therapy. Participants were assessed with the Assisting Hand Assessment (AHA) at pre-intervention, post-intervention, and follow up.
RESULTS:
The results showed improved motor functions in both groups. Analysis using the general linear model (analysis of covariance) and Bonferroni post hoc tests showed significant improvements from pre-intervention to post-intervention in the AHA for the IG. The CG showed non-significant improvement in AHA scores.
CONCLUSIONS:
These findings suggest that the MI training, combined with the physical practice program used in this study, was effective in improving upper limb function in children with HCP.
Introduction
The ability to perform various hand activities is reduced in children with hemiplegic cerebral palsy (HCP). Sensory and motor impairments observed in the affected upper extremities are a major cause of functional compromise (Rosenbaum et al., 2006). These impairments limit performance on simple tasks of daily living, such as changing clothes, brushing teeth, combing hair, feeding, and playing, and can be limiting in a wider social context as well (Rosenbaum et al., 2006). Therefore, an obvious goal of neurorehabilitation is to improve the capacity and performance of the affected arm, in order to promote its effective use in daily tasks (Gordon, 2011). According to Buccino et al. (2012), even when involved in an integral rehabilitation program including conventional physical therapy, use of orthosis, and treatment of spasticity, around 75% of children with HCP may present motor impairments in activities of daily living. Therefore, there is an urgent need to propose new rehabilitation programs that aim at adding to the effects of conventional therapy.
In this study, we assessed the feasibility of using motor imagery (MI) as an adjunct technique to improve upper limb motor function in children with HCP. MI could be an alternative or ancillary approach in these children’s rehabilitation of the upper limb. It has been investigated as a therapeutic option in adults with post-stroke hemiplegic deficits (Liu, Chan, Lee, & Hui-Chan, 2004; Crosbie, McDonough, Gilmore, & Wiggam, 2004). To the best of our knowledge, there is no investigation of this approach with HCP.
It has been proposed that motor deficits observed in children with HCP involve impairments in both motor execution and planning (Steenbergen, Verrel, & Gordon, 2007). However, the current rehabilitation techniques focus predominantly on deficits in motor execution and do not specifically address deficits in the movement preparation processes, i.e., in motor planning. Evidence suggests that problems with motor planning can also adversely affect the performance of activities of daily living, and therefore, need to be treated (Steenbergen, Jongbloed-Pereboom, Spruijt, & Gordon, 2013). Research suggests MI as a promising method to train the “cognitive” aspects of motor behavior that can be effective in reducing the motor planning deficits observed in children with HCP (Williams, Reid, Reddihough, & Anderson, 2011; Steenbergen, Crajé, Nilsen, & Gordon 2009).
MI is a cognitive process, in which the covert trial of a motor action is conducted via manipulation of motor representations in working memory without any external manifestation of the motor act (Jackson, Lafleur, Malouin, Richards, & Doyon, 2001). According to Jeannerod (2001), MI is closely related to the motor representations involved in the planning and execution of movements. According to Sirigu and Duhamel (2001), MI corresponds to a process by which the nervous system activates a motor plan and follows its deployment through internal feedback signals, while the motor output remains in a state of inhibition. It is postulated that MI is endowed with similar properties as those of the corresponding motor act and may be involved in the same causal relationship in the generation of a movement (Jeannerod, & Decety, 1995). Thus, when performing MI tasks, impulses are generated and sent to the muscles responsible for that action. This activation may have an important role in assisting the learning and improving of motor skills (Braun, Beurskens, Borm, Schack, & Wade, 2006; Grezes, & Decety, 2001). This hypothesis is supported by a brain imaging study led by Jackson et al. (2001), which demonstrated that MI induced changes in the pattern of brain activation in cortical areas associated with motor planning.
Previous studies have emphasized the similarities between the executed and imagined movements, with regard to neurophysiological and psychophysical parameters, providing evidence that both may be based on similar processes (Malouin, Richards, & Durand, 2012; Jeannerod, 2001; Grezes, & Decety, 2001). From the neurophysiological point of view, experiments using functional magnetic resonance imaging showed that the neural structures activated during the execution of movements are also activated during MI tasks. Specifically, brain regions, such as the supplementary motor area (Grezes, & Decety, 2001), premotor cortex (Jackson et al., 2001), primary motor cortex (Gerardin et al., 2000), cerebellum (Lotze et al., 1999), and posterior parietal cortex (Grezes, & Decety, 2001), are activated during both execution and imagery of different motor actions. Considering the psychophysical similarities, behavioral studies have shown that the time taken to imagine a movement and its effective implementation are temporally coherent (Parsons, 1994). A similarity between MI and execution is also observed with regard to changes in heart and respiratory rate observed during MI tasks. This suggests similar actions of the autonomic nervous system in both situations (Oishi, Kasai, & Maeshima, 2000).
From this evidence, we suggest that MI may favor the acquisition of motor skills through systematic mental trials. Steenbergen et al. (2009) proposed that MI may be useful in training the motor neural networks after injury in the central nervous system. Previous studies mostly investigated the effectiveness of MI in acute (Malouin, Richards, & Durand, 2012) or chronic post-stroke aged patients (Sharma, Pomeroy, & Baron, 2006). Experimental studies indicate a tendency for positive effects of MI on training of motor learning (Jackson Lafleur, Malouin, Richards, & Doyon, 2003), reduction of sensorimotor deficits (Liu et al, 2004), improvement of upper limb function (Page, Levine, & Leonard, 2007), cortical reorganization (Page, Szaflarski, Eliassen, Pan, & Cramer,2009), and performance improvement in the execution of daily activities (Crosbie et al., 2004) in post-stroke subjects. A systematic review by Braun et al. (2006), and a meta-analysis by Kho, Liu, and Chung, (2014) investigated the effects of MI training in the recovery of upper limb function in post-stroke patients. Both studies concurred that MI training effects were beneficial (d = 0.5).
Based on these adult post-stroke beneficial effects, it could be hypothesized that children with HCP might also benefit from a rehabilitation program involving the use of MI. In a preliminary small-scale study, Cabral, Narumia, and Teixeira, (2010) evaluated the effects of MI training on three children with diplegic cerebral palsy by assessing their ability to climb a ladder. The results showed major reductions of up to 88.12% in the time needed to perform the task. In a subsequent study, Cabral-Sequeira, Coelho and Teixeira, (2016) evaluated the effects of pure MI training and its combination with physical practice in motor learning of a sighting task that required speed and precision with the paretic arm of children with HCP. In this experimental design, the experimental group (n = 8) underwent 1 day of mental practice and one of physical practice, while the control group (n = 8) underwent recreational activity on the first day and physical practice on the second day. The authors concluded that MI training appears to be a potentially useful feature to increase motor learning in individuals with HCP. The gains obtained can be justified by the fact that the imagined movement modulates the activity in the neural network, increasing the potential of the physical practice to induce higher levels of motor performance (Cabral-Sequeira, Coelho & Teixeira, 2016).
Despite such evidence, the use of MI in the rehabilitation of the upper limbs of children with HCP has not been explored extensively. Consistent with the experimental results of Cabral-Sequeira, Coelho, and Teixeira (2016), MI associated with physical practice seems to be an effective tool in inducing neural plasticity and improving motor performance. It is also believed that for certain motor tasks, imagined movement can lead to higher performance gains than those observed with physical practice (Allami, Paulignan, Brovelli, & Boussaoud, 2008). In addition, another advantage of this method is the non-exclusion of children with limited physical ability, since this is a factor that limits their participation in many rehabilitation protocols. Thus, for children in whom severe motor limitations impede movement, imaginary training can help to keep the motor program active, facilitating the future execution of movements (Lameira et al., 2008).
The present study aimed to investigate the effects of MI associated with physical practice on upper limb improvement in children with HCP. We developed a specific treatment protocol that aimed at training activities of daily living. We used a quasi-experimental, intelligence-controlled study in 24 children with HCP. We hypothesized that children who received MI intervention associated with physical practice would show better results when compared to children in a control group.
Methods
Participants and study design
Children with HCP were recruited from two large university-associated clinical rehabilitation centers located in Belo Horizonte and its metropolitan area in Minas Gerais, Brazil. Twenty-four participants diagnosed with HCP, aged 7–14 years (mean = 10.75, SD = 2.08) were included in the study. Nineteen children had probable lesions in the left cerebral hemisphere (right hemiplegia) and 5 had probable lesions in the right cerebral hemisphere (left hemiplegia). The individuals eligible to participate in the study met the following inclusion criteria: normal intelligence and working memory, and the ability to collaborate with the physical or occupational therapy at the enrolled institutions and ability to perform the MI task. The ability of motor imagery was assessed by the task of mental rotation (see Steenbergen, van Nimwegen & Craje, 2007). The study excluded children with associated pathologies, such as progressive, epilepsy or hydrocephalus, genetic syndromes, movement disorders, or children who had surgery or botulinum toxin injections in the last 6 months.
The participants were divided into two groups: intervention group (IG; n = 12, mean age = 10.25, SD = 2.95 years) and control group (CG; n = 12, mean age = 11.25, SD = 2.66 years). Group allocation was defined according to geographic location of the participating institutions. Children in the nearest located institution performed the MI training (IG). Children in the other institution served as controls (CG), requiring only the pre-test and post-test assessments, and receiving conventional care in between. IG participants also received conventional treatment regularly.
In a quasi-experimental study, we compared the performance in pre-test and post-test outcome measures of two non-randomly selected groups of children with HCP. One group received MI training, as well as conventional physical therapy (IG); the other group received only conventional physical treatment, and served as control (CG). The primary outcome was measured through the Assisting Hand Assessment (AHA) [41]. The results were controlled for intelligence.
Assessment measures
The domains assessed to select participants and to control for confounding effects were as follows: intelligence, evaluated through the Raven’s Coloured Progressive Matrices test (Bandeira, Alves, Giacomel, & Lorenzatto, 2004) and the Block Design subtest of the Wechsler Intelligence Scale (Wechsler, 2002); the working memory evaluated by the backward Digit Span and backward Corsi Cubes tests (Santos, Mello, Bueno, & Dellatolas, 2005); and manual ability according to the Manual Ability Classification System (MACS) (Eliasson et al., 2006).
Main outcome measure
The AHA (version 4.3) was used as an outcome measure to evaluate the effects of MI training on upper limb function (Krumlinde-Sundholm, Holmefur, Kottorp & Eliasson, 2007). The instrument was selected for evaluating the efficiency with which a unilateral disabled child makes use of their (assistive) affected upper limb during activities that require bimanual coordination. First, a 10—15 min play session with a specific toy from the AHA test kit, which requires bimanual manipulation, is video recorded. Later, the video recordings are analyzed based on 22 predefined items by using a classification scale ranging from 1 to 4 points. The sum of the raw score ranges from 22 (low capacity) to 88 (high capacity) points. The instrument has excellent reliability and validity (Holmefur, Krumlinde-Sundholm & Eliasson, 2007; Krumlinde-Sundholm et al., 2007). For statistical data analysis, the raw score obtained by the participants was considered. A licensed physical therapist, familiar with the AHA, conducted the evaluation. Video evaluations were made by a blinded, trained therapist.
Interventions
MI training protocol
This is the first study to assess the effectiveness of MI training in the rehabilitation of the upper limbs of children with HCP. The MI training protocol used in this study was established based on other investigations that used MI on adults with post-stroke hemiplegia (Malouin, Richards, & Durand, 2012; Riccio, Iolascon, Barillari, Gimigliano, & Gimigliano 2010; Page, Levine, & Leonard 2007), and on children with dyspraxia (Wilson, Thomas, & Maruff, 2002).
The activities in which the children had difficulty performing independently were selected to compose the MI training protocol (see Table 1). The performance of the tasks by a 12-year-old girl was recorded and used as a model for both imagined and physical execution. For each task, a video was made lasting between 1080s.
Daily living activities of participants trained in the MI protocol
Daily living activities of participants trained in the MI protocol
The training protocol of MI for daily activities was conducted as follows: (1) initially, each participant was instructed to focus on the movement technique of the model performing the task (third-person perspective). (2) Next, the participant was asked to concentrate and try to perform this task mentally on his/her own (first person perspective). (3) After mental training, the participant was required to perform the activity physically; the objects needed to perform the tasks were provided on a table. The combination of MI and physical practice was used in the study in view of the evidence that when MI and physical practice are provided in the same session, the results are synergistic (Malouin, Jackson, & Richards, 2013).
In each session, participants in the IG performed all activities listed in the MI protocol. The sessions took place twice a week, for eight consecutive weeks (Table 1). The average length of the sessions was 50 min and they were conducted in the rehabilitation center that the participant attended. IG participants continued to receive conventional therapy (see details below). The MI training was conducted by the first author, who is a licensed physical therapist.
The participants of the CG received no MI training. All individuals continued treatment with conventional therapy. The sessions in the rehabilitation centers were offered once or twice a week, according to the children’s needs. The care offered to participants in the two rehabilitation centers was similar, since both centers are school clinics in partnership with the same University. The duration of the session averaged 50 min and included muscle stretching, strengthening exercises, and exercises to improve grasp function, manipulation, grip, and fine pinch, among others. In contrast to the MI protocol, which focused on upper limb function, conventional therapy sessions also addressed the recovery of plegic lower limbs through stretching, muscle strengthening, balance and gait training.
Procedures
All research procedures were previously approved by the local research ethics board. Participation was dependent on written informed consent by parents and oral consent by children. Each participant was individually evaluated. The first evaluation (pre-intervention) occurred in the first week of the intervention period. The second evaluation (post-intervention), using only the AHA, was performed at the end of the intervention period and 8 weeks after the intervention (follow-up). Researcher 3, a licensed physiotherapist, performed all assessments blindly. Cognitive tests were performed by a licensed psychologist (researcher 4).
Participants allocated to the IG underwent the MI protocol, twice a week, for eight consecutive weeks with an average of 50 min per session. Throughout the training for the MI tasks, the participants were seated comfortably on a chair that was positioned 50 cm away from a 14 inch flat screen laptop. Each previously recorded video was presented individually on the laptop screen. The participants were instructed to watch the videos attentively, concentrating on the technique used by the model performing the task. After this observation period, the participants were asked to perform the task mentally. The actions were presented in a fixed order according to their complexity, as judged by the experimenters. Each mental trial was repeated five times. At the end of each mental repetition, the objects needed for performing the activities were placed on the table. The participants were then instructed to perform the action as demonstrated in the video.
The participants of the CG continued treatment with conventional therapy, which was offered once or twice a week by a physical or occupational therapist. The treatment goals established by the therapists who tended to the children were maintained and no change of routine care occurred during the study period.
Statistical analyses
Sample homogeneity, in relation to sex, laterality of hemiplegia, and manual ability level, was assessed using the chi-square test. The Student’s t-test for independent samples was used to compare the mean age, and the z-score was used for intelligence, working memory, and the AHA prior to the intervention.
Between-group differences in AHA scores in the post-test were analyzed using general linear models (analysis of variance). To investigate to what extent intelligence would influence the results, a model of analysis of covariance (ANCOVA), including intelligence as a covariate, was used. When the results showed significant main effects, the Bonferroni post hoc analysis for multiple comparisons was used to identify differences. The level of significance was defined at p < 0.05. Analyses were performed using SPSS (version 1.4).
Results
All 24 participants who underwent the pre-intervention evaluation completed the study. The groups were homogeneous in relation to sex, laterality of hemiplegia, and MACS level of manual ability. The mean age did not differ significantly between the groups. The number of sessions carried out by participants did not differ between groups. Information regarding the participants’ characteristics and results of between-group comparisons are provided in Table 2.
Characteristics of study participants
Characteristics of study participants
MACS: Manual Ability Classification System.
The groups did not differ significantly regarding intelligence and working memory, as shown in Table 3. Moreover, both groups started the study with a similar level of upper limb functional performance, as evidenced by the AHA (t = 0.026; p < 0.980).
Between-group comparison of intelligence and working memory
Note: Intelligence test values are expressed in z-score.
The results of the comparisons between the intervention and control groups based on the AHA scores from pre-intervention to post-intervention and follow-up assessments are provided in Table 4. Although group differences in intelligence were not significant, the effect sizes were non-negligible. Thus, we decided to control for the effects of intelligence in the outcome analysis. The results of analysis of variance (ANCOVA) for the three measurement points indicated a statistically significant interaction between the group and the AHA (F 7.94; p < 0,001; η2 = 0.254), when controlled for the effects of intelligence. Post hoc comparisons indicated that, for IG, significantly higher values were found in the post-test and follow-up compared to the pre-test (p < 0.05). Post-intervention and pre-intervention AHA scores differed for the IG (p = 0.001). We also observed significant differences between the pre-intervention and follow-up measures (p = 0.015) in the IG. Post hoc comparisons for the three sequential AHA measures did not differ for CG (p > 0.05).
Comparison between outcome measures in the intervention and control groups
*p < 0.005; IG = Intervention group; CG = Control group.
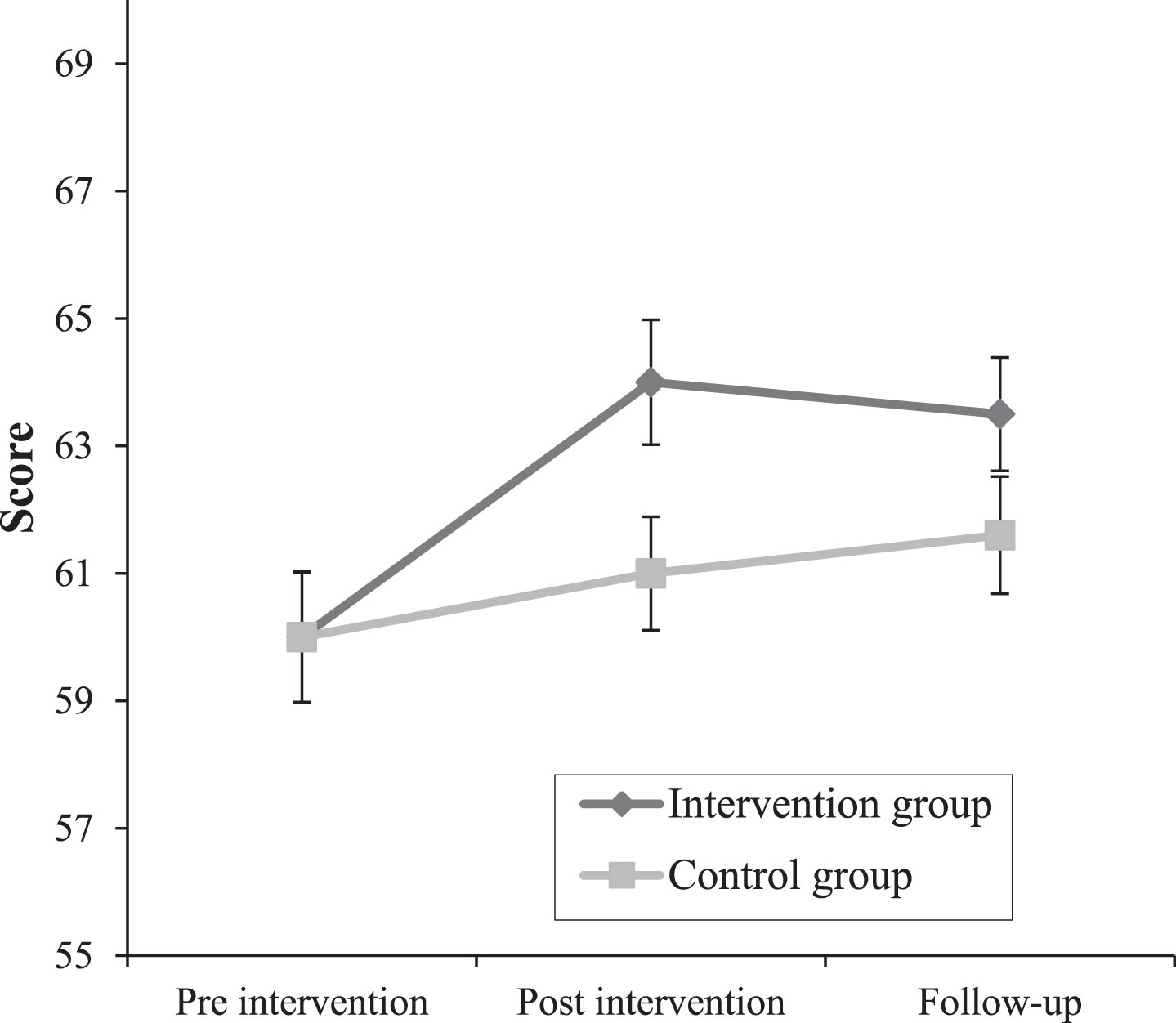
Progression of the evaluation means carried out at three different time points. Note: Each point represents the average obtained by the groups in the AHA test during pre-intervention, post-intervention and follow-up measurements.
In this study, we evaluated for the first time the effect of MI training as a therapeutic alternative, for motor rehabilitation in children with HCP. The results of this study document changes in upper extremity function resulting from a MI protocol associated with physical practice. The IG practiced MI followed by the physical execution of bimanual activities of daily living in two 50-min weekly sessions for 8 weeks. Measures in the CG were taken at corresponding intervals. Significant differences in the AHA were obtained between post-test and pre-test comparisons, and the IG showed a large effect size, even when controlling for the effects of intelligence. Results of the follow-up measure in the IG were non-significant and the effect size was moderate. No intragroup differences for the AHA were observed in the CG, and effect size was small.
Our results suggest that MI training could be a feasible adjunct to physical recovery of upper limb function in HCP children. This is consistent with results of previous studies showing beneficial effects of MI training on upper limb function in adults with stroke sequelae (Kho, Liu, & Chung 2014; Malouin Jackson, & Richards, 2013; Page, Levine, & Leonard, 2007; Liu et al., 2004), walking in diplegic children (Cabral, Narumia, & Teixeira, 2010), manual motor performance in children with intellectual disabilities (Porretta, & Surburg, 1995), and motor learning of the upper limb in hemiplegic children (Cabral-Sequeira, Coelho & Teixeira, 2016).
Our results indicate a trend toward greater gains by combining the imagined movement followed by physical practice compared to conventional single therapy. These findings are consistent with previous results showing that MI training increases gains from subsequent physical practice (Cabral-Sequeira, Coelho & Teixeira, 2016; Allami et al., 2014). We believe that the combined practice reinforced the internal representation of the trained motor act. Allami et al. (2008) showed that physical execution and the sensorial feedback of practice activate different neural networks involved in the executed and imagined movement. Previous studies show that imagined movements share neural substrates similar to the movements executed (Malouin, Richards & Durand, 2012; Grezes, & Decety, 2001; Jeannerod 2001) and induce brain plasticity similar to that obtained with physical practice (Liu et. al., 2004; Page et al., 2009; Jackson et al., 2001). In a neuroimaging study, Zhang et al. (2011) found functional brain changes induced by MI training in the fusiform gyrus, striated body and thalamus. Thus, it is possible that the activation of the motor and somatosensory pathways in both practices favored the acquisition of motor skills, helping to establish and reinforce trained movement patterns. Therefore, from the present and previous results, it is plausible that MI training can explain the superior results of protocols combining MI and physical practice compared with protocols based on physical practice alone (Liu et al. 2004, Page et al., 2009).
In one of the few studies that investigated the effectiveness of imaginary training in hemiplegic adolescents, Cabral-Sequeira, Coelho and Teixeira, (2016) showed, with different kinematic variables, the effect of this technique on performance gains in a goal task. Although a single imaginary training session was used in the cited study, the authors showed that the combination of imaginary and physical practice provided superior performance gains when compared to isolated physical practice. We believe that MI training may result in gains in motor function alone, but it also seems to increase the effects of concomitant physical practice. For Gomes et al. (2012), the practice of isolated imagery is inferior to physical and combined practices, but it is more effective when compared to the absence of practice. According to Allami et al. (2008), when combined proportionally, imaginary and physical practice play an important role in motor gains. On the other hand, there is also evidence that the practice combined with lower rate of imagery practice appears to be less effective in inducing improvements in motor performance (Gomes et al., 2012; Allami et al., 2008).
Our results corroborate the findings already found with MI training in typically developing children. Doussoulin and Rehbein (2011) showed that the benefits of MI training were comparable to those found in physical practice. In a group of 9 to 10 year-olds, the authors reported improvement in movement quality and ball-throwing proficiency. In a sample of healthy adolescents, Hemayattalab and Movahedi (2010) found that MI training followed by physical practice produced significant gains in basketball free throw proficiency. In both studies, the experimental protocol involved the imagined movement and the execution of the same actions in a short time, as proposed in our study. The results of these studies support our findings by showing that imaginary training followed by physical practice is more effective when compared to isolated practice.
We found in the literature a large number of studies evaluating the effectiveness of MI training in upper extremity function after brain injury. For adults with hemiplegia, studies show increased hand and finger movement and relearning of functional tasks after the use of protocols involving MI training (Braun, et al., 2006; Crosbie et al., 2004; Jackson et al., 2003). In a study of people with chronic hemiplegia, Page, Levine, and Stephen (2007) showed that the training of MI, associated with physical practice, resulted in a significant improvement in the movement of the affected upper limb compared to the group that only performed physical practice. The meta-analysis by Kho, Liu, and Chung, (2014), showed that 4 out of the 5 studies analyzed reported significant effects of MI in post-stroke patients. Our study is one of the first to evaluate the effectiveness of MI training associated with physical practice in the rehabilitation of the upper limb of hemiplegic children. The results found are similar to those reported in adult hemiplegia and reaffirm the potential of the combination of physical and imaginary practices in neurological rehabilitation.
Our study revealed significant differences between the pre- and post- intervention measures for the IG, evidencing improvements in functional abilities. The absence of statistical differences between the post-intervention and follow-up measures indicates that the improvements obtained persisted after a period of 8 weeks and did not suffer a decrease after the suspension of the intervention protocol. We believe that the maintenance of the motor gains in the children of the IG was because of the potential of MI training in triggering specific sensorimotor representations that increase the learning potential of physical tasks in the subsequent period, thus achieving neuroplasticity. Strengthening our hypothesis, evidence suggests that motor imaging increases the excitability of different brain areas associated with motion planning and control (Allami et al. 2008; Sharma, Pomeroy & Baron, 2006; Jackson et al., 2003). Previous studies have also demonstrated the persistence of imaging training effects (Cabral-Sequeira, Coelho & Teixeira, 2016; Debarnot et al., 2009), supporting the hypothesis that when associated with physical training, this technique can induce stable performance gains. From these results, our study supports the hypothesis proposed by Steenbergen et al. (2009) that MI is a potential therapeutic tool for the rehabilitation of individuals with cerebral palsy.
Two main limitations of the present study must be discussed. First, the design of this study was not randomized. Group allocation was geographically based. We have reasons to believe, however, that no substantial sociodemographic differences exist in the target population of the two centers. Both centers are affiliated with the same university and follow similar theoretical and methodological guidelines. In addition, the groups were homogenous for all variables evaluated, including gender, age, laterality of hemiplegia, performance of manual ability, and intelligence. Second, the sample size was small. However, it is worth noting that the CG did not present significant differences in the comparisons between pre-intervention and post-intervention and pre- and follow-up- measures, with a small effect size, d = 0.05 and d = 0.03, respectively. Thus, the sample size needed to obtain statistical significance at p < 0.05 would require 1237 participants (Mackey, & Gass, 2015).
When performing a statistical power analysis for the comparisons between groups in the post-intervention AHA score, we verified that a sample of 310 volunteers was necessary to reach statistical significance, since the magnitude of the effect size was small (d = 0.20). When comparing the AHA score between groups during the follow-up period, the effect size was found to be even smaller (d = 0.15) and would require a sample of 1237 participants. Knowing that the incidence of cerebral palsy is around 2 to 3 per 1000 live births in developed countries and 7 per 1000 live births in developing countries (Paneth, Hong, & Korzeniewski, 2006), it is unfeasible to achieve such a high sample count. In addition, to apply an intervention study on such a large sample would require a large team of researchers as well as greater financial resources.
Despite these limitations, strengths of the study to be highlighted include the use of the AHA, a well-validated outcome measure, and the relatively good comparability of the two groups before receiving the intervention. Regarding intelligence, for example, a small effect size of d = 0.24, would require a sample size between n = 138 and n = 310 to become statistically significant at α= 0.05 and β coefficient = 0.80. We also required that participants had a reasonable working memory and processing capacity to complete the training. Furthermore, the training protocol was easily comprehensible for the children, it was easy to apply, relevant for daily activities, and can be used even with children with major degrees of paralysis.
Although this study provides preliminary evidence of the effectiveness of MI training in children with HCP, some points can be improved to get better results. For future studies, we believe that the protocol of MI activities should be individualized, i.e., defined based on the needs of each child. In the current study, although the protocol has been defined based on the functional limitations presented by the children, all participants were trained for the same activities that were frequent difficulties commonly faced by the group.
Finally, increasing the sample size and using a randomized allocation design is necessary for improving study.
Clinical implications
Considering the results of the present study, we believe that MI training can be applied to clinical practice. We believe that MI is potentially less invasive and intense than other additional methods of treatment. Moreover, for many individuals with lesions in the central nervous system, the execution of certain movements is very difficult, sometimes impossible, which complicates their active participation in the rehabilitation process. Thus, an additional advantage of this training is that it will include participants who are usually excluded from physical training programs owing to their limited physical ability. Another advantage of the application of MI is that it can be used safely, it does not require special equipment or facilities, and it is a simple and low-cost resource (Sharma et al., 2006). Finally, MI can be used at home without professional supervision (or with parental supervision).
Conclusion
Further development of techniques for the recovery of functionality in HCP patients is essential to promote functional independence and to improve quality of life. MI has emerged as a potential alternative for functional rehabilitation and has been known to reduce motor deficits in this population. With this study, we observed that MI training combined with physical practice appears to be a useful and effective method that presents significant results in improving functional performance in children and adolescents with HCP. However, this study only provides preliminary evidence because there is a lack of clinical trials about the use of this therapeutic approach in children with HCP, and established rehabilitation protocols using MI are not yet available. Thus, future studies are needed to establish training protocols that allow consistency in the results.
Conflict of interest
The authors report no conflicts of interest.
Footnotes
Acknowledgments
The authors thank the children, their parents, and the rehabilitation centers for participating in this research. This work was supported by grants from the Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG, APQ-02755-SHA, APQ-03289-10, APQ-02953-14, APQ-03642-12). VGH is supported by the CNPq excellence in research fellowship (308157/2011-7, 308267/2014-1).