
Abstract
BACKGROUND:
Latin America has exceptionally high rates of traumatic brain injury (TBI), but very little research has been conducted on longitudinal TBI outcomes in this global region.
OBJECTIVE:
This study examined whether cognitive dysfunction and social disadaptation in individuals with TBI in Latin America at hospital discharge predict longitudinal trajectories of depression at baseline, 2 months, and 4 months.
METHODS:
A sample of 109 people with a new TBI was recruited from three hospitals: Mexico City, Mexico, Cali, Colombia and Neiva, Colombia. Participants completed measures of cognitive dysfunction and social disadaptation before hospital discharge and measures of depression at baseline, 2 months, and 4 months.
RESULTS:
Results suggested that depression scores were found to decrease over time in a quadratic (or U-shaped) fashion, and more significant cognitive dysfunction at hospital discharge was associated with higher longitudinal depression trajectories. Social disadaptation did not exert a unique effect on depression trajectories after controlling for cognitive dysfunction. Depression trajectories changed differentially over time as a function of baseline cognitive dysfunction, such that for those with high cognitive impairment, depression scores started high and then dropped to a moderated range and plateaued, but for individuals with low cognitive dysfunction, depression scores started lower and decreased linearly but moderately.
CONCLUSIONS:
The results suggest a strong need for neuropsychological assessments and evidence-based cognitive rehabilitation strategies to be implemented immediately after TBI in Latin America, which could exert salubrious effects on depression trajectories over time.
Introduction
Traumatic brain injury (TBI) annually affects over 50 million people worldwide (Maas et al., 2017) and involves an alteration in brain functioning or pathology due to an externally induced head trauma, often resulting in long-lasting disability (Menon, Schwab, Wright, & Maas, 2010). Approximately 60% of all TBIs worldwide result from road traffic accidents, 20–30% from falls, 10% from workplace/sports-related injuries, and 10% from violence (Gururaj, 1995). TBI is a chronic disease that reduces life expectancy (Masel & DeWitt, 2010), and the burden of TBI disproportionally affects low- and middle-income countries, leading to high fatality rates in those global regions (Puvanachandra & Hyder, 2008). Latin American TBI incident rates are the highest globally due to high rates of violence and road traffic injuries (Hyder et al., 2007). Due to injuries resulting from landmine explosions and hostile guerillas, TBI prevalence in Colombia is approximately 6.4 per 1,000 individuals (Pradilla, Vesga, Boris, & León-Sarmiento, 2003), and TBI is the third leading cause of death in Mexico (Julio César, Torres Norma, Lozano, & Zúniga Carrasco, 2008). People with TBI can experience a substantial burden of impairments including cognitive, emotional, physical, and psychiatric issues, as well as familial disruption (Draper & Ponsford, 2008; Maas et al., 2017). Long-term consequences of these impairments include reduced quality of life (Coronado et al., 2012), although the impact of TBI-related impairments on mental health outcomes in Latin America is not well understood.
One of the most significant sequelae of TBI is cognitive impairment. Cognitive dysfunction following TBI includes impairments in attention, executive functioning, memory acquisition, delayed memory, language, visuospatial skills, and motor functioning, all impacting long-term quality of life post-injury (Belanger et al., 2005). Konrad and colleagues (2010) specifically found that people with TBI often have significant impairments in learning, recall, working memory, attention, and executive functioning. People with TBI also often experience deficits in processing speed years after injury (Draper & Ponsford, 2008). Frequently, complex cognitive functioning is impaired in TBI, resulting in difficulty with problem-solving, self-direction, planning, and organizing cognition and behavior (Arciniegas, Held, & Wagner, 2002).
In addition to cognitive functioning, social functioning can be impaired post-TBI, manifesting in disinhibition and social inappropriateness (Silver, Yudofsky, & Anderson, 2005). Social behavior changes are often expressed in emotional lability, poor social judgment, and indifference (Kendall, 1996). Due in part to these changes, many people with TBI are unable to return to work or maintain meaningful social relationships (Malia, Powell & Torode 1995). For caregivers, social and cognitive changes tend to be a greater burden than physical impairments (Kinsella, Parker, & Olver 1991).
Mental health concerns are long-term problems following TBI, with major depression rates ranging from 14–77% and generalized anxiety disorder ranging between 3–28% (Koponen et al., 2002). Depression after TBI has been associated with psychosocial (Gomez-Hernandez, 1997) and cognitive dysfunction (Rapoport, McCullagh, Shammi, & Feinstein, 2005). Mental health problems after TBI are particularly detrimental because they interfere with both recovery and rehabilitation (Arciniegas, Held, & Wagner, 2002).
The effects of TBI are more pronounced in Latinos compared to other populations (Perrin et al., 2013). Latinos with TBI experience more neurobehavioral concerns (Arango-Lasprilla et al., 2012), poorer quality of life (Arango-Lasprilla, Krch, Drew, de Los Reyes Aragon, & Stevens, 2012), and higher rates of severe disability (de la Plata et al., 2007). TBI impairments can last for many years due to a combination of wide-ranging impairments and lack of rehabilitation resources in Latin America that may result in increased rates of mental health problems post-injury (Arango-Lasprilla et al., 2012). Due to high costs associated with TBI-related impairments, identification of cognitive, emotional, or psychosocial factors that may impact poorer outcomes is imperative, particularly in Latin America. Identification of the impairments at discharge from acute rehabilitation that predicts longitudinal trajectories of mental health in this region may help identify individuals at risk for poorer outcomes and therefore reduce the burden on people with TBI, their families, and health care systems. Ottowitz, Tondo, and Dougherty (2002) found that cognitive dysfunction at the time of injury was positively associated with depression, yet no research has examined whether cognitive and social dysfunction immediately after TBI predicts longitudinal trajectories of mental health in Latin America. As a result, this study aims to examine whether cognitive dysfunction and social disadaptation in individuals with TBI in Latin America at hospital discharge predict longitudinal trajectories of depression at baseline, 2 months, and 4 months.
Method
Participants and procedure
A sample of 109 people with a new TBI was recruited from three hospitals in Mexico City, Mexico (n = 68), and in Cali (n = 21) and Neiva (n = 20), Colombia. These hospitals have high volumes of TBI treatment that aided in recruitment for the study. There were several inclusion criteria: participants must have (a) had a diagnosis of TBI, (b) been be over the age of 18 at enrollment, and (c) been able to read and write in Spanish. To ensure participants met these criteria, they were pre-screened before beginning the study. Participants were asked for informed consent to participate under ethics committee approval at each site, and then they completed all measures orally due to potential issues with literacy. Participants’ mean age was 35.87 (SD = 14.08), and 82.6% were men. Participants’ had an average number of years of education of 9.99 (SD = 3.55), and they had spent on average, 20.78 (SD = 28.95) days in the hospital for their TBI. The following were the causes of TBI: automobile accident (11.0%), motorcycle accident (37.6%), bicycle accident (2.8%), pedestrian accident (6.4%), firearm (1.8%), act of violence (15.6%), sports accident (.9%), fall (21.1%), and other (2.8%).
Measures
European brain injury questionnaire (EBIQ)
The Spanish EBIQ was designed to measure broad aspects of life for individuals with brain injuries. The EBIQ is a 63-item questionnaire covering 8 domains of everyday life: somatic, cognitive, motivation, impulsivity, depression, isolation, physical, and communication (Teasdale et al., 1997). Participants rate each item on a 3-point Likert-type scale: (1) “not at all,” (2) “a little,” and (3) “a lot.” Further factor analyses of the EBIQ found the existence of three subscales: Cognitive Dysfunction, Depression, and Social Disadaptation symptoms (Bateman, Teasdale, & Willmes, 2009) which incorporated cultural context and expression lending to higher levels of adaptation of the EBIQ across cultures (Caracuel et al., 2011). Higher scores on these subscales reflect greater impairment. The current study utilized the two subscales Cognitive Dysfunction and Social Disadaptation to avoid the multicollinearity of using the EBIQ Depression subscale to predict depression outcomes. The EBIQ is a clinically reliable measure that has been found to assess change over time (Sopena et al., 2007).
Patient health questionnaire-9 (PHQ-9)
The Spanish PHQ-9 is a depression module based on the 9-item DSM-IV criteria (Arrieta et al., 2017; Muñoz-Navarro et al., 2017). The PHQ-9 was designed for use in clinical practice and research. The depression module scores each of the 9-item DSM-IV criteria as “0” (not at all) to “3” (nearly every day). Scoring used the mean of all items such that higher mean scores indicate higher levels of depression. The PHQ-9 has good internal reliability with a Cronbach’s alpha = .89, good test-retest reliability, sensitivity of 88% and specificity of 80% (Arrieta et al., 2017; Muñoz-Navarro et al., 2017).
Results
Both the EBIQ and PHQ-9 had complete data at baseline, and the PHQ-9 had missing data from one participant at 2 months and four participants at 4 months. Full information maximum likelihood (FIML) estimation was used to account for these missing data.
Hierarchical linear modeling (HLM) was used to examine baseline predictors of depression trajectories across baseline, 2 months, and 4 months. Unconditional growth linear (straight line) and quadratic (U-shaped) models were run with no predictors to determine the most accurate model for linear or polynomial curvature of depression scores over time. The -2 log likelihood (-2LL) of the unconditional growth model with linear time was 1894.34, whereas the -2LL of the unconditional growth model with the addition of quadratic time was 1889.88, which represented a drop of 4.46 that surpassed the critical χ2 value of 3.84 for statistical significance (p < .05). As a result, the movement of depression trajectories overtime was best-modeled as quadratic, or U-shaped, across the full sample.
In a main effects HLM predicting quadratic depression trajectories, time, time*time, cognitive dysfunction, and social disadaptation were entered simultaneously as fixed effects after being centered. All statistically significant and non-significant fixed effects from the HLM and their b-weights, p-values, standard errors (SEs) and 95% confidence intervals appear in Table 1. In the HLM, time, time*time, and cognitive dysfunction yielded statistically significant effects. Across the three time points, depression scores significantly decreased (p = .001). Individuals with higher cognitive dysfunction had higher overall depression trajectories than those with lower cognitive dysfunction (p < .001, Fig. 1). However, social disadaptation was not a significant predictor of depression trajectories.
Predictors of depression trajectories at baseline, 2 months and 4 months after TBI
Predictors of depression trajectories at baseline, 2 months and 4 months after TBI
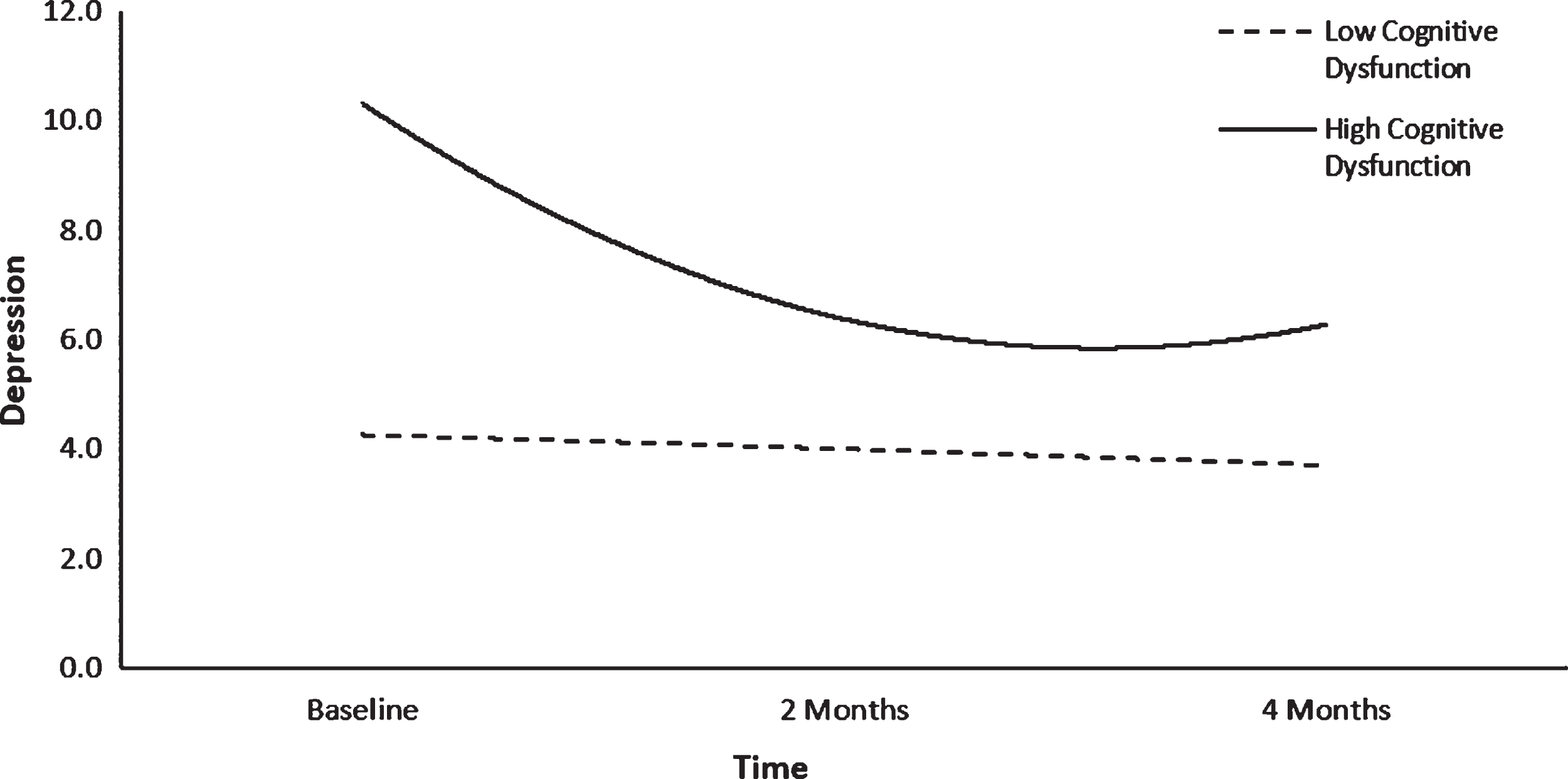
Depression trajectories over time as a function of cognitive dysfunction.
HLM predicting quadratic depression trajectories, time, time*time, cognitive dysfunction, and social disadaptation were entered simultaneously as fixed effects after being centered. All statistically significant and non-significant fixed effects from the HLM and their b-weights, p-values, standard errors (SEs) and 95% confidence intervals appear in Table 1. In the HLM, time, time*time, and cognitive dysfunction yielded statistically significant effects. Across the three time points, depression scores significantly decreased (p = .001). Individuals with higher cognitive dysfunction had higher overall depression trajectories than those with lower cognitive dysfunction (p < .001, Fig. 1). However, social disadaptation was not a significant predictor of depression trajectories.
To examine whether the statistically significant fixed effect of cognitive dysfunction interacted with quadratic time in the prediction of participants’ depression trajectories, an interaction effects HLM was run. In this model, the fixed effects were time, time*time, cognitive dysfunction, time*cognitive dysfunction, and time*time*cognitive dysfunction (Table 1). The time*time*cognitive dysfunction interaction term was statistically significant (p = .010), suggesting that the slopes of participants’ depression trajectories differed over time as a function of cognitive dysfunction. Figure 1 suggested that for individuals with high cognitive dysfunction at baseline, depression scores started high and then dropped to a moderated range at 2 months, plateauing at 4 months. For individuals with low cognitive dysfunction at baseline, depression scores started lower and decreased linearly but moderately across 2 and 4 months.
This study examined whether cognitive dysfunction and social disadaptation in individuals with TBI at hospital discharge in Latin America predict longitudinal trajectories of depression at baseline, 2 months, and 4 months. Depression scores were found to decrease over time, and greater cognitive dysfunction at hospital discharge was associated with higher longitudinal depression trajectories. Social disadaptation did not exert a unique effect on depression trajectories after controlling for cognitive dysfunction. Depression trajectories changed differentially over time as a function of baseline cognitive dysfunction, such that for those with high cognitive impairment, depression scores started high and then dropped to a moderated range and plateaued, but for individuals with low cognitive dysfunction, depression scores started lower and decreased linearly but moderately.
The current finding of depression trajectories decreasing during the first year of TBI is congruent with findings in the United States. Bombardier, Hoekstra, Dikman, and Fann (2016) investigated depression scores at four times points within the first year of TBI and found depression scores decreased over time. In another study, depression rates were found to decrease from an initial rate of 41% at hospital discharge after TBI to 3% at a 1-year follow up in a sample of TBI patients (Taino, Jorge, & Robinson, 2003). The decrease in depression scores across time found in the current study may be paralleling findings in the United States as individuals with TBI adjust to their new impairments and experience some return of functioning. In the United States, rehabilitation services after TBI have been associated with improved mood over time (Seel et al., 2003), but the current sample from Latin America received minimal rehabilitation services so that gains can be attributed in part to spontaneous recovery. Additionally, the change in patients’ mood over time may be due to returning home to the family environment, as inpatient hospital visits are restricted in terms of time and the number of family members allowed, which can isolate patients from family contact. Family proximity and affiliation is very important in a Latin American context.
The current study’s findings of higher depression trajectories among individuals with greater cognitive dysfunction at discharge is congruent with outcomes in the United States. Satz et al. (1998) found a strong association between depressive symptomatology and cognitive functioning in TBI patients. Major depression has been found to be associated with cognitive dysfunction at 6 months after TBI, with executive functioning being the most consistent deficit (Ottowitz, Tondo, Dougherty, & Savage, 2002). Additionally, Ponsford, Draper, and Schonberger (2008) found that depression and anxiety, as well as difficulties in cognitive deficits (executive functioning and attention), predicted poorer outcomes at 10 years following TBI. Cognitive impairment may magnify the development and severity of major depression across time (Rapoport, McCullagh, Shammi, & Feinstein, 2005), and the findings from the current study suggest that this same process is operating after TBI Latin America.
The current study found that social disadaptation at hospital discharge did not predict depression trajectories after TBI in Latin America, contrary to findings in the United States. Gomez-Hernandez and colleagues (1997) found that social functioning impacted depression during the first year after TBI and recommended targeted social interventions to improve rehabilitation outcomes. Similarly, psychosocial functioning has been found to be associated with depression for five years after TBI (Hibbard, et al., 2004) in the United States. There are two possible explanations for the difference in the current study to the previous studies. First, cognitive dysfunction and social disadaptation could be multicollinear, such that the overlapping variance between the two constructs caused the predictive effect of social disadaptation to not reach statistical significance. A second possible explanation for the difference is that Latin America has cultural values rooted in familism. Familism or familismo is the mutual support between family members emphasizing family honor and interconnectedness (Calzada, Huang, & Brotman, 2012). Family or group needs are placed over that of the individual (Ting-Toomey et al., 2000), such that individuals with TBI may be receiving continued support from family and friends no matter their level of social adaptation and this support could buffer the development of depression over time. Future researchers are encouraged to investigate possible cultural strengths, including familism that may be buffering the impact of social disadaptation on depression trajectories among individuals with TBI in Latin America.
Clinical implications
The current findings have several implications for clinical services after TBI in Latin America. As individuals with higher cognitive dysfunction were found to have elevated depression trajectories, neuropsychological assessment of cognitive functioning at hospital discharge is imperative for understanding longitudinal trajectories of mental health. The implementation of even brief neuropsychological screeners in Latin America, similar to those used in the current study, when resources for full comprehensive batteries are unavailable, can aid in detecting individuals with TBI who are at risk for poor trajectories of quality of life indices over time. Individuals shown to have elevated cognitive dysfunction immediately after TBI can be presented with culturally tailored cognitive rehabilitation strategies. These include a myriad of activities including “direct attention training; selection and training of external memory/ organizational aids; training in internal memory strategies; metacognitive strategy training; social pragmatics training; environmental modification; brain injury education for patients, family, and employers; and aggressive support during gradual reentry into community and vocational/educational activities” (Helmick, 2010, p. 243). The findings from the current study suggest that these evidence-based strategies should be culturally tailored and implemented before and after hospital discharge, as well as become part of the standard of rehabilitation care for TBI in Latin America.
The findings from the current study also highlight the importance of identifying individuals with cognitive impairment and immediate implementation of mental health services to improve the quality of life over time. Cognitive-behavioral therapy (CBT) has been adapted to treat depression and other mental health issues in individuals with TBI (Hsieh, Ponsford, Wong, & McKay, 2012). As CBT targets disturbances in behavior, emotions, and cognitions, it is well suited to address various combinations of possible TBI impairments (Yody et al., 2000). In addition, relational approaches rooted in peer-mentoring programs wherein the family and friends of the person with TBI adjust their behavior have been found to decrease misunderstanding and improve relationships (Hanks, Rapport, Wertheimer & Kviak, 2012). Such approaches, particularly given the cultural value of familism in Latin America, should be tailored and adapted for this population.
Limitations and future directions
The current findings should be considered in the context of several limitations. First, participants were recruited from two countries, Mexico and Colombia, and although this is the first longitudinal study of depression trajectories after TBI in Latin America, caution is recommended when generalizing the study’s findings to other countries in Central and South America. Future studies are encouraged to recruit from additional sites and countries to improve generalizability of the findings. Second, the current study assessed depression symptomology at hospital discharge, 2 months, and 4 months. As depression trajectories may shift later in the first year due to the chronic nature of behavioral and psychosocial disturbances, future studies should investigate depression trajectories for more extended follow-up periods after TBI in Latin America. Third, the current study investigated cognitive dysfunction globally with a single total score. Future studies should investigate what specific aspects of cognitive dysfunction (e.g., memory, attention, executive functioning) may be impacting depression trajectories in Latin American.
Conclusion
TBI disproportionally affects Latin American countries, reflected in higher injury and fatality rates, as well as reduced rehabilitation outcomes. The current study provides evidence that cognitive dysfunction at hospital discharge after TBI predicts longitudinal depression trajectories. These findings suggest the importance of neurological assessments at injury to identify individuals with higher cognitive dysfunction. This practice would allow the targeted implementation of evidence-based cognitive rehabilitation strategies and mental health treatment, which together may have the potential to impact depression trajectories over time. Future studies may also investigate unique cultural strengths or buffers that protect against depression among individuals with TBI in Latin America.
Funding
This study was funded by grant #R21TW009746 from Fogarty International Center of the National Institutes of Health.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors wish to acknowledge Clínica Medilaser sucursal Neiva and Clínica Uros.