
Abstract
BACKGROUND:
Obesity is a known risk factor for stroke, but its impact on functional recovery is less clear. Understanding the effect of obesity on functional recovery during inpatient rehabilitation will aid clinicians in patient counselling and help administrators with program planning.
OBJECTIVE:
To determine if obesity affects the functional outcomes of adults undergoing inpatient stroke rehabilitation.
METHODS:
MEDLINE, Embase, CINAHL, and Cochrane databases were searched using the subject headings and text word terms for stroke, rehabilitation, and obesity. Two independent reviewers screened the articles against pre-defined eligibility criteria and extracted the data. Outcomes of interest included FIM, mRS, Fugl-Meyer Assessment of Sensorimotor Recovery after Stroke, and Barthel Index.
RESULTS:
Seven studies from five countries with a total of 3070 participants were included. There was significant heterogeneity among the studies in the BMI cut-off points and functional outcome measures used. Two studies found a positive association between obesity and functional outcome, two studies found no association, and three studies reported a negative relationship.
CONCLUSIONS:
No conclusions could be drawn regarding whether the functional outcome of adults undergoing inpatient stroke rehabilitation differ between individuals with and without obesity.
Introduction
Stroke is a leading cause of disability world-wide (GBD 2016 DALYs and HALE Collaborators, 2017). In order to optimize functional recovery after stroke, patients often require inpatient rehabilitation (Herbert et al., 2016). There are a number of factors that can affect functional recovery and the identification of these features is important for prognostic counselling and rehabilitation planning. Given that obesity has been associated with functional impairment and disability in the general population (Alley and Chang, 2007), it is important to explore its potential impact on recovery after stroke.
Rationale
Obesity is a known risk factor for ischemic stroke (Strazzullo et al., 2010) and is associated with functional impairment in the general population (Alley and Chang, 2007). However, research examining the impact of obesity on functional recovery after stroke has produced conflicting results (Burke et al., 2014; Kalichman et al., 2007 & 2016; Nishioka et al., 2016). Given the increasing prevalence of obesity in the general population (Twells et al., 2014; Chooi et al., 2019), it is anticipated that an increased proportion of obese patients will also be seen in the inpatient rehabilitation setting. This systematic review will evaluate and summarize the results of studies investigating the effect of obesity on functional outcomes of patients participating in inpatient stroke rehabilitation. The results of this review will aid clinicians in providing patient counselling and will inform administrators regarding inpatient rehabilitation planning strategies. Furthermore, it may also direct future studies to address deficiencies in the rehabilitation literature.
Objective
To determine if the functional outcomes of adults undergoing inpatient stroke rehabilitation differ between individuals with obesity and those without obesity.
Methods
Study design
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used for reporting the study protocol (Moher et al., 2009).
Eligibility criteria
Participants
The review focused on adults age ≥18 years admitted to inpatient stroke rehabilitation. Studies of individuals with ischemic and/or hemorrhagic stroke were included. Data from participants with stroke only admitted to acute care, living in the community, or participating in outpatient rehabilitation programs were excluded. This ensured a more homogeneous population of stroke severity and time since stroke as most patients accessing inpatient rehabilitation have had a moderate severity stroke and are in the subacute phase at the time of admission. In addition, functional measures used in the inpatient rehabilitation setting tend to be universal between hospitals and are used internationally.
Prognostic factor and comparison
Studies examining the functional outcomes of individuals with obesity, classified by authors using Body Mass Index (BMI), were included.
Types of outcome measures
The outcomes of interest included measures of function commonly used in the stroke population. Specifically, the outcome measures included were the Functional Independence Measure (FIM) (Keith et al., 1987; Ring et al., 1997), Modified Rankin Scale (mRS) (Rankin, 1957), Fugl-Meyer Assessment of Sensorimotor Recovery after Stroke (Fugl-Meyer et al., 1975), and Barthel Index (Mahoney and Barthel, 1965).
Types of studies
Cohort studies, non-randomized experimental trials, and randomized controlled trials were eligible for inclusion. Case reports, case series, cross-sectional and case-control studies, and conference abstracts were excluded. Studies were also excluded if papers could not be obtained in English.
Information sources and search strategy
A professional librarian (EU) ran a search in MEDLINE, MEDLINE-in-Process, MEDLINE Epubs Ahead of Print, and Embase Classic + Embase databases (OvidSP); CINAHL (EBSCOHost); and Cochrane database (Wiley) on February 13, 2019. Both subject headings and text word terms for stroke and rehabilitation and obesity were used. We retrieved a total of 3214 references. All references were saved in an EndNote library and 449 duplicates were removed. The remaining 2765 unique references were reviewed against our inclusion criteria. Monthly auto alerts were set. These retrieved 121 additional references between February and August 2019. The complete search strategy is outlined in Table 1.
Search strategy for MEDLINE
Search strategy for MEDLINE
Search strategy for Medline-in-Process
Search strategy for Medline Epub Ahead of Print
Search strategy for EMBASE
Search strategy for CINAHL
Search strategy for Cochrane
One reviewer (SLM) screened the unique titles and excluded those that were unmistakably irrelevant. The references were then imported into the Covidence software program (Covidence, Veritas Health Innovation, Australia) and two unblinded, independent reviewers (SLM, WSJ) screened the titles and abstracts against the eligibility criteria. Where there was uncertainty or disagreement regarding the appropriateness of a study, the reference was included for full text review. The full texts of potentially eligible articles were again assessed against the eligibility criteria by the same two reviewers. Disagreements were resolved by discussion amongst the two reviewers. The reason for excluding articles after full text review was documented.
Data extraction
A data extraction form was developed and piloted using three articles. Based on the pilot results, adjustments were made prior to proceeding to the full data extraction phase. Extracted data included the location of the study; a description of the rehabilitation program (if available); patient demographics, including age and percent male; a definition of weight categories used (i.e. obese defined as BMI≥30 kg/m2); and the proportion of individuals in each weight category. The study designs, outcome measures, as well as a descriptive summary of the outcome stratified by BMI category were recorded. For the analysis and results, the following items were extracted: the statistical model used, the potential confounders adjusted for, the test statistic (if available), p-values, and overall conclusions.
Two independent reviewers extracted the data and the results were collated. Discrepancies were resolved by discussion between the two reviewers. Study authors were contacted by email for further information, where applicable.
Risk of bias
The Joanna Briggs Institute Critical Appraisal tool for use in JBI Systematic Reviews: Checklist for cohort studies was applied to each study (Joanna Briggs Institute, 2017). The reviewers completed the checklists independently and disagreements were resolved through discussion. No studies were excluded based on the risk of bias assessment.
Data synthesis
Data were presented using a narrative synthesis. As discussed below, a meta-analysis was planned but was unable to be performed due to lack of study homogeneity.
Results
Study selection
A total of 2,765 titles and abstracts were screened for eligibility. Full text reviews were performed on 64 articles. As the manuscript was in preparation, an additional 121 papers were retrieved using Auto-alerts with one of these studies meeting the inclusion criteria for the systematic review. Reasons for exclusion can be found in Fig. 1. Where articles were excluded for more than one reason, only one reason for exclusion was recorded. Emails were written to the corresponding authors of two studies. We received a response from one author confirming that their outcome measure was recorded at the end of inpatient rehabilitation and this study was included (Karaahmet et al., 2018). For the second study, it was unclear whether the patients were admitted to an inpatient rehabilitation facility (Kawase et al., 2017). Several attempts were made to reach the corresponding as well as co-authors but were unsuccessful. This study was excluded from the review.
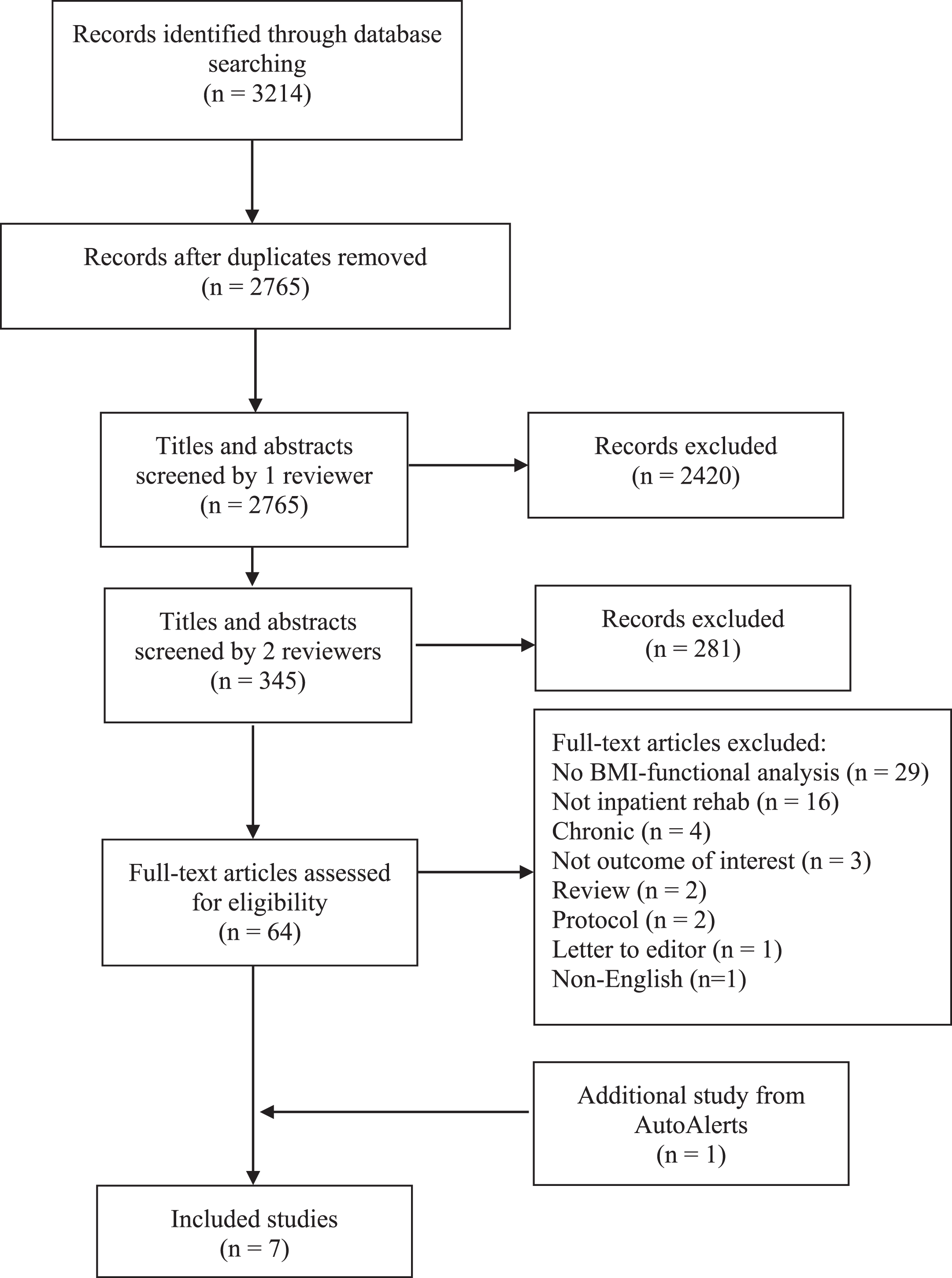
PRISMA flow diagram.
A total of seven studies, with a total of 3070 participants, met the inclusion criteria (Table 2). The seven studies originated from five countries, including two from Japan (Nishioka et al., 2016; Hagii et al., 2018), two from Israel (Kalichman et al., 2007 & 2016), one from the USA (Burke et al., 2014), one from Turkey (Karaahmet et al., 2018), and one from Italy (Morone et al., 2019). Of note, the Israeli studies were by the same author. With the exception of one study published in 2007, the rest were recent, published between 2014 and 2019. The smallest study included 84 individuals and the largest 897. The total mean age was not presented for one study, however, when average age by weight category was included, the mean age across studies ranged from 63 to 82. In general, patients who were underweight tended to be older and individuals who were obese were younger. Furthermore, there was a lower percentage of males in the underweight and obese categories.
Description of studies
Description of studies
Most studies did not describe their rehabilitation programs in detail. Rehabilitation length of stay (LOS) differed significantly between studies, ranging from 27 days in the Burke et al. (2014) study from the USA to 122 days in the Nishioka et al. (2016) study from Japan.
All studies utilized BMI to define their weight categories; however, there was some variability in the BMI ranges used between studies. For example, Nishioka et al. (2016) used BMI categories in accordance with the World Health Organization BMI for Asian Populations where obesity is defined as greater than 27.5 kg/m2. In the Burke et al. (2014) study, obesity was defined as a BMI of 30 kg/m2, which is consistent with most North American classifications. Others created a category to include all overweight patients (BMI > 25 kg/m2) (Hagii et al., 2018; Karaahmet et al., 2018). Morone et al. (2019) did not specify the BMI ranges used for their underweight, normal, overweight, and obese categories. Furthermore, although many of these studies treated BMI as a categorical variable, Kalichman et al. (2007;2016) used BMI as a continuous variable.
Five of the seven studies used FIM as their outcome measure, however, the manner in which they presented the FIM data was variable. Three studies presented FIM change (discharge –admission FIM) (Kalichman et al., 2016; Nishioka et al., 2016; Karaahmet et al., 2018), one used FIM efficiency (discharge –admission FIM/LOS) (Burke et al., 2014), and one presented relative improvement of FIM (Kalichman et al., 2007). Relative improvement of FIM is not a standard method of reporting FIM in the rehabilitation literature. The authors defined this as: (FIM at discharge –FIM at admission)×100/FIM at admission. One study used mRS as their outcome measure with a mRS≥3 considered an unfavourable functional outcome (Hagii et al., 2018). Of note, because mRS was not recorded at admission, functional change during inpatient rehabilitation was not captured. Morone et al. (2019) was the only study to utilize the Barthel Index as their outcome measure.
Many of the baseline characteristics were dissimilar between BMI groups in these retrospective cohort studies. Furthermore, some studies did not present comparisons of baseline factors making it unclear whether there were statistically significant differences between groups in addition to BMI. Baseline differences could be controlled for by a regression analysis. However, one study only performed a univariate analysis (Karaahmet et al., 2018) and another a correlation (Kalichman et al., 2007), which does not account for potential confounders. Morone et al. (2019), did not control for confounders in their analyses either. The Burke et al. (2014) study did account for age and sex by using an ANCOVA. Risk of bias assessment was completed by both reviewers and these data are presented in Table 3. The items with the highest risk of bias included the reporting of baseline characteristics, dealing with confounders, and appropriate statistical analysis.
Risk of bias assessment
Risk of bias assessment
Main results
Of the seven studies, two reported a positive association between obesity and functional outcome (Nishioka et al., 2016; Morone et al., 2019), two did not find an association between increased BMI and functional outcome (Hagii et al., 2018; Karaahmet et al. 2018), and three demonstrated a negative association (Burke et al., 2014; Kalichman et al., 2007 & 2016).
Nishioka et al. (2016) demonstrated a positive effect of obesity (BMI≥27.5 kg/m2) on FIM change. This was the largest study and included 897 participants. Overall, the study had a low risk of bias and used strategies to deal with confounders. In a prospective study of 664 participants, Morone et al. (2019), also found that increased BMI was correlated with improved rehabilitation effectiveness as reflected by the Barthel Index.
The two studies that did not find an association between increased BMI and functional outcome did not use a specific obesity category and instead examined all individuals who were classified as overweight (BMI≥25 kg/m2) (Hagii et al., 2018; Karaahmet et al., 2018). They each used different outcome measures; with one paper reporting mRS (Hagii et al., 2018) and the other reporting FIM change (Karaahmet et al., 2018). The study that reported FIM change performed univariate statistics only and was one of the smaller studies, including only 85 participants (Karaahmet et al., 2018). The second study, by Hagii et al. (2018), reported statistically significant differences between BMI categories for mRS score at discharge in their univariate analysis. A BMI of <18.5 kg/m2 was associated with the worst outcome (median mRS 5), a BMI between 18.5 and 24.9 kg/m2 was associated with a median mRS score of 3, and a BMI≥25 kg/m2 had the most favourable outcome (median mRS 2) (p = 0.001). However, in their adjusted analysis, using a normal BMI of 18.5 to 24.9 kg/m2 as a reference, there was no association between a BMI of≥25 kg/m2 and a discharge mRS score ≥3.
Finally, for the three studies that reported a negative association between BMI and functional outcome (Burke et al., 2014; Kalichman et al., 2007 & 2016), two were from the same author and included BMI as a continuous variable (Kalichman et al., 2007 & 2016). The 2007 study used a non-standard form of FIM as their outcome measure whereas the 2016 study used FIM change and accounted for potential confounders. In their 2016 study, Kalichman et al. reported mean FIM change for individuals who were normal weight, overweight, moderately obese, and severely obese and showed a consistent decline in FIM change with increasing weight category (Kalichman et al., 2016). The Burke et al. (2014) study, however, did not demonstrate a linear relationship. They reported that overweight individuals (BMI of 25.1–30 kg/m2) achieved the highest mean FIM efficiency (1.38), but found that obese individuals (>30 kg/m2) had a lower mean FIM efficiency (1.03), which was similar to underweight (<18.5 kg/m2) persons (1.01).
A meta-analysis was not possible as a result of study heterogeneity. As described above, even though five of the seven studies reported FIM as the outcome measure, they used different aspects of the FIM (FIM efficiency, FIM change, and relative improvement of FIM). Although three studies used FIM change as their outcome, they treated BMI differently in their model –one as a continuous variable (Kalichman et al., 2016), one as a 3-level categorical variable (Karaahmet et al., 2018), and one as a 2-level categorical variable (obesity –yes/no) (Nishioka et al., 2016). Furthermore, two of the studies presented means (SD) (Kalichman et al., 2016; Karaahmet et al., 2018), and another study presented medians (25th–75th percentiles) (Nishioka et al., 2016). These factors precluded a meta-analysis.
Discussion
Search process
Our search retrieved a total of seven studies that investigated the impact of obesity in stroke inpatient rehabilitation functional outcomes. The papers retrieved were international, which likely contributed to the significant variability in study definitions of BMI, delivery of rehabilitation services, and functional outcome measures used.
Quality assessment
The greatest risk of bias was in the reporting of baseline characteristics, identifying strategies to deal with confounders, and the statistical methodology (Table 3). Given that factors such as age, sex, and stroke severity have previously been shown to impact outcome after stroke, future studies should attempt to reduce the potential impact of confounding by adjusting for these variables (Di Carlo et al., 2003; Burton et al., 2018).
Furthermore, the considerable variation in the BMI cut-off points and the different functional outcome measures used in the studies made between-study comparisons difficult. Other authors have also noted that North American stroke rehabilitation studies are more likely to use the FIM whereas European studies more frequently utilize the Barthel Index (Sangha et al., 2005).
Inpatient rehabilitation approaches and outcomes may also vary internationally. For example, in Canada many patients are transferred to rehabilitation units either within or outside of acute care hospitals as soon as possible. Furthermore, the median inpatient rehabilitation length of stay in Canada is 31 days (CIHI, 2016). Nishioka et al. (2016) reported a median LOS of 122 days, which is almost four times longer. This increased LOS allows more time for potential functional improvements.
Summary of evidence
Obesity is known to contribute to functional impairment in the general population and specifically can lead to bone, joint, and mobility dysfunction (Alley and Chang, 2007). In the stroke inpatient rehabilitation environment, patients often present with motor dysfunction and medical consequences of immobility. Therefore, a reasonable hypothesis is that obesity may influence functional recovery, particularly mobility outcomes.
With the exception of the papers by Nishioka et al. (2016) and Morone et al., (2019), the overall trend was for obesity (not merely being overweight) to have either no association or a negative impact on functional outcomes. However, the studies have varied significantly in their methodologies, outcomes, and conclusions making it difficult to generalize the findings.
Notably, four studies suggested that a BMI < 18.5 kg/m2 is associated with a worse functional outcome (Burke et al., 2014; Hagii et al., 2018; Karaahmet et al., 2018; Morone et al., 2019). Papers by Burke et al. (2014) and Hagii et al. (2018) indicated that the individuals with the poorest functional outcomes had a BMI < 18.5 kg/m2. As a result, when examining the impact of obesity on functional outcome, it is important to clearly distinguish the comparator group. That is, to differentiate between comparators who have a normal BMI and those comparators who are “non-obese” and include persons who are underweight. Nishioka et al. (2016) demonstrated a functional benefit in individuals who were obese when they compared individuals with obesity (BMI≥27.5 kg/m2) to all other individuals with a BMI < 27.5 kg/m2. In this study, however, the comparator, BMI < 27.5 kg/m2, was likely acceptable as median FIM change for persons who were underweight was similar to those who were normal and overweight. Morone et al., (2019) also demonstrated a relationship of increased BMI with rehabilitation effectiveness, however, the BMI ranges used were not defined in their methods.
Although understanding the impact of obesity on functional outcomes is important in order to aid clinicians in providing patient counselling and to inform administrators regarding inpatient rehabilitation planning strategies, this systematic review was unable to draw any definitive or generalizable conclusions.
Limitations
We did not search the grey literature, include conference abstracts, or non-English literature in this review. Therefore, it is possible that there is further evidence that may contribute to our understanding of the impact of obesity on functional recovery in the inpatient rehabilitation setting that was not identified using our methods. Moreover, the specific manner in which stroke rehabilitation services are delivered internationally may also impact outcomes and, therefore, the relationship between obesity and functional recovery after stroke.
Conclusions
Based on the current evidence, it is unclear whether functional outcomes of adults undergoing inpatient stroke rehabilitation are affected by obesity. Future research should consider following the WHO classification system and categorize individuals as underweight, normal weight, overweight, and obese (using categorical variables). Furthermore, consideration should be given to individuals who are underweight when planning the analysis given that the relationship between obesity and functional outcomes may not be linear. Additional factors to consider include the use of FIM change or FIM efficiency as the outcome measure and the utilization of regression analyses to adjust for potential confounders.
Conflict of interest
The authors declare that there are no conflicts of interest for the publication of this paper.
Dr. Shannon MacDonald receives funding from the Dr. Eliot A. Phillipson Department of Medicine Fellowship.
Footnotes
Acknowledgments
We would like to thank Lusine Abrahamyan and Petros Pechlivanoglou for their guidance and comments on this project.