
Abstract
BACKGROUND:
An intensive task-oriented circuit training (TOCT) provides a valid approach in improving motor function in Multiple Sclerosis (MS).
OBJECTIVE:
We aimed at testing the efficacy of TOCT on gait kinematics in MS patients with mild-moderate disability.
METHODS:
Nineteen MS patients able of independent walking performed 3-D Gait Analysis before (T0) and after (T1) a two-week TOCT program. Patients were clustered in two different subgroups, according to clinical neurological impairments assessed with specific functional system of Expanded Disability Status Scale (EDSS): pyramidal (Group 1) and cerebellar (Group 2) subjects. Spatio-temporal and kinematic data were compared before and after the TOCT intervention in the total sample of patients and in the two selected subgroups at two time intervals.
RESULTS:
Data obtained revealed increased dynamic ROM at knee joint after training in the whole study sample. Of note, knee dynamic excursion improved significantly in Group 1 but not in Group 2 patients after TOCT. Moreover, sagittal plane kinematics revealed significant modifications on knee and ankle biomechanics in Group 1 after rehabilitation.
CONCLUSIONS:
These data point out the benefits of the task specific training on gait dynamics in mild impaired MS subjects, linking to treatment opportunity in patients with a prevalent pyramidal impairment.
Introduction
Multiple sclerosis (MS) is a demyelinating disease characterized by progressive clinical impairment, resulting in muscle weakness, sensory disturbances, spasticity, gait ataxia, visual deficits and cognitive impairment (Karussis et al. 2014). Disease progression has a variable course, finally leading to severe functional disabilities with an important impact on health, independence and quality of life (Compston et al. 2008). MS structural damage can impair a huge variety of subsystems involved in the collection and integration of sensory information towards the selection of appropriate motor responses (Heesen et al. 2008): slow ambulation, difficulty in response to postural adjustments and postural instability represent the subsequent dysfunctions (Cattaneo et al. 2014). Gait disturbances frequently appear along disease progression, and almost 85% of patients report ambulatory dysfunctions as their main complaint (Comber et al. 2017): reduced walking speed, step length, cadence, increased step width and stride variability and reduced dynamic excursion at all lower-extremity joints represent the most common features (Comber et al. 2017). Abnormal gait pattern, along with static and dynamic balance impairment (Peebles et al. 2018), contributes to reduce mobility and functional abilities and increases risk of falls (Giannì et al. 2014). Indeed, fall rates in this population is considerably high, with recent literature indicating that a percentage between 52% and 63% of patients will experience a fall in a 2–6 months period (Mazumder et al. 2015). Everyday life activity is the most frequent involved situation (Gunn et al. 2014), with almost 80% of falls occurring during postural transfers and 60% during gait tasks (Sosnoff et al. 2011). Then, the critical loop between postural instability, gait abnormalities, falls and risk of falls suggests that these are key factors to be addressed while prescribing training interventions.
As currently known, updated reviews and international guidelines recommend physical activity in MS people (Sà et al. 2014), stating its positive effects on cardiovascular fitness, fatigue, walking capacities and quality of life (Dettmers et al. 2009, Rampello et al. 2007). In fact, stating that ambulatory function is necessary for daily activity, promoting customized strategies addressing patients’ walking abilities may have significant clinical impact. The rehabilitation of gait disorders primarily involves aerobic exercise, resistance training and gait training to enhance gait efficiency and safety and to correct abnormal gait patterns. Gait training, such as conventional treadmill training, body weight-supported treadmill training or robotic-assisted treadmill training, has been used in MS with positive results on walking performance (Bethoux 2013). Recently, a two weeks high-intensity task-oriented rehabilitation training (TOCT) has revealed feasible and safe in MS people with moderate mobility impairments, with benefits on motor function, walking abilities and quality of life (Chisari et al. 2014).
On this panorama, despite the growing literature about rehabilitation in MS, only few studies focused on quantitatively assessing gait biomechanics changes induced by training interventions (Rodgers et al. 1999, Pau et al. 2017, Gutierrez et al. 2005). Recently, the most benefical effects of rehabilitation strategies were revealed on spatio-temporal parameters assessed with gait analysis (Pau et al. 2017, Guner et al. 2015), while kinematic evaluations evidenced improvement restricted to dynamic range of movement (ROM). Interestingly, Gutierrez et al. (2005) pointed out the normalization of stride parameters and symmetrisation of toe clearance between two lower limbs induced by a lower-limb resistance training. Anyway, to our knowledge, no one of the aforementioned studies focused on specific association between clinical assessment of neurological impairment and the effects of training interventions on ambulatory function in MS.
On this background, the aim of this study is to test the efficacy of a previously validated Task-Oriented Circuit Training (TOCT) on gait kinematics in MS patient with mild-moderate disability (Chisari et al. 2014). Since our previous investigations pointed out functional improvements during walking tests and increased quality of life, our hypothesis is that individuals with MS who underwent the TOCT program would exhibit positive modifications in gait biomechanics. Moreover, we evaluate if patients with a specific neurological impairment, assessed with clinical scores, could reveal specific gait improvements after our training intervention. In particular, we hypothesized that the characterization of gait modifications on the basis of patients’ clinical features may help physicians to plan rehabilitation needs and target treatment options.
Materials and methods
Participants
We recruited 19 Multiple Sclerosis patients (12 female and 7 male, mean age 51,79±10,06 years), with either the relapsing-remitting, primary progressive or secondary progressive subtype.
Inclusion criteria were: males and females; age >18; diagnosis of MS according to McDonald Revised Criteria (relapsing-remitting, primary or secondary progressive), (Polman et al. 2005); clinical stability for at least three months (no relapses, no disability worsening and no other medical complications); motor impairment assessed with the Expanded Disability Status Scale (EDSS) score between 4 and 5.5 (Kurtzke 1983). preserved walking ability for a short distance (10 m) without use of devices.
Patients were excluded from the study if they had: rehabilitation since 1 month before the beginning of the study; impaired cognitive functioning (Mini Mental Status Examination score less than 24); other causes than MS which may affect motor function (orthopedic or other neurological diseases); unstable cardiovascular conditions; severe lower limb spasticity or contractures that may limit ranges of motion (Ashworth score >4 for hip, knee or ankle flexors/extensors).
All participants underwent comprehensive neurological examination and disability was scored according to the EDSS by an experienced clinician (Kurtzke 1983). The EDSS is an eight functional system scale that includes: motor, sensory, cerebellar, brain stem, visual, mental, sphincters, and others. Each domain is graded from 0 = no disability, to 5 or 6 = maximal disability based on history and physical examination. According to the score in each functional system, an integrated score between 0 = normal examination and 10 = death from MS, is derived. Demographic variables including age and gender along with MS phenotype, clinical impairment and disease modifying therapy were collected. According to the dominant functional system involved, assessed with the EDSS, all participants were divided in two subgroups (Givon et al. 2009): group 1, including 11 patients with prevalent pyramidal impairment (mean age 52,5±8,2 years); group 2, including 8 patients with prevalent cerebellar dysfunction (mean age 50,7±13 years). Group 1 presented clinical functional impairment in the pyramidal system, ranging from abnormal signs without disability, minimal disability to mild or moderate hemiparesis. Group 2 showed clinical functional impairment in the cerebellar system, ranging from abnormal signs without disability, mild ataxia to moderate truncal or limb ataxia. A brief description of patients’ functional status is reported in Table 1. Participants received written and oral instructions about the intervention, test protocol and possible risks and benefits of the study. Written informed consent was obtained before any evaluation or treatment, and subjects received a copy of the consent form during the initial interview. Our study project was designed in accordance with the Declaration of Helsinki and was approved by the local Ethics Committee of Pisa (study protocol - Nr. 484, 2015-52984, approval number 52984). Outcome measures and gait analysis evaluation were assessed the week prior the treatment initiation (T0) and at the end of treatment (T1).
Characteristics of study sample
Characteristics of study sample
All patients underwent a rehabilitative treatment accounting for 10 sessions, 5 sessions per week; each session lasted 120 minutes overall and was organized as a circuit: 30 minutes of gait training with treadmill, 10 minutes of stretching, 30 minutes of task-oriented circuit, 10 minutes of rest, 30 minutes of task-oriented circuit and 10 minutes of muscle strengthening (Chisari et al. 2014). The task-oriented circuit was organized in several stations in which patients were asked to: overcome an obstacles course, made up with sticks placed on the ground, in a frontal and then lateral direction; achieve various targets placed at different heights sights on a mirror with the feet, walk along a 10 meter long line drawn on the ground, climb and descent stairs. This approach comprehended different working stations reflecting physical activities usually performed during daily living (walking, climbing stairs, maintain balance), with the aim to promote motor learning and retention. In addition to the choice of functional motor tasks, main characteristic of this rehabilitative intervention is the exercise intensity that, compared to a conventional outpatient approach, was closer to the number of repetitions needed to achieve and maintain motor learning of these movements. The circuit was conceived with a progressive evolution and intensity was defined by the time dedicated to a specific exercise. The choice of motor tasks and progression is specifically tailored on patients’ competencies and functions. Specifically for complexity progression, patients were encouraged to increase their level of functioning among sessions, according to their motor disabilities. Rests were used to discuss about difficulties and to provide further feedback.
Gait analysis evaluation
All subjects underwent 3-D Gait Analysis performed at Motion Analysis Laboratory of Neurorehabilitation Unit of the University Hospital of Pisa, using the ELITE System (BTS Bioengineering, Milan, Italy). Before the recordings, general and anthropometric data were collected. Then, spatio-temporal and kinematics data were acquired through six photogrammetric system infrared cameras acquiring at a sampling frequency of 100 Hz; 18 reflective markers were placed on definite anatomical landmarks for kinematic acquisitions, according to Davis protocol (Davis et al. 1991). Acquisitions were made in standing position and during barefoot walking at self-selected speed, recording at least three trials for each limb. The average value across all three trials for each leg was used for analysis.
Data analysis
Spatio-temporal and kinematic parameters analysis for the hip, knee, and ankle joints were performed by using BTS Elite Clinic software. The following spatio-temporal parameters were analyzed: walking velocity, cadence, stride time, stride length, step time, step length, step width, double limb support time and the percentages of stance and swing phases compared to the total duration of gait cycle. As regard the kinematic pattern, a body model accounting for each body segments was used to calculate articular angular excursions along the gait cycle. In the sagittal plane, the value of the maximum and the minimum angle reached in each joint (hip, knee, ankle) was calculated: peak ankle plantarflexion angle in early stance (PAPA_ES), peak ankle plantarflexion angle at toe-off (PAPA_TO), peak ankle dorsiflexion angle in terminal stance (PADA_TS), peak ankle dorsiflexion angle in swing (PADA_S), peak knee flexion angle (PKFA), peak knee extension angle (PKEA), peak hip flexion angle (PHFA), peak hip extension angle (PHEA). Furthermore, the dynamic range of motion (ROM) of each joint was determined.
Statistical analysis
Descriptive statistic (mean, median, standard deviation, percentiles and confidence interval) were used to describe sample at T0 and T1. Normality of data distribution was assessed through Shapiro-Wilk test. The non-parametric Wilcoxon signed-rank tests were used to determine if any changes in gait parameters occurred before (T0) and after (T1) the TOCT intervention in the whole sample of subjects.
The two subgroups were matched for anthropometric variables such as age, sex, height, weight as confirmed with Mann Whitney U-test test for non-parametric samples. Data were analyzed non-parametrically with the Mann-Whitney U-test for independent group comparisons at the two time intervals (T0 and T1). The non-parametric Wilcoxon signed-rank tests were used to determine if any changes in gait parameters occurred before (T0) and after (T1) the TOCT period in each subgroup of patients.
All reported p-values are results of two-tailed tests. Results are described in relation to the significance of p < 0,05. All statistical procedures were performed with SPSS/PC (version 20.0) software program.
Results
Spatio-temporal data
No significant difference was revealed in spatio-temporal parameters after rehabilitation treatment in the whole study sample (Table 2). Moreover, the analysis of spatio-temporal parameters in the two subgroups of subjects revealed no significant difference after training period (Table 3). Anyway, when considering the difference between the two groups, Group 2 showed increased walking velocity, reduced double limb support time and stance time duration compared to Group 1, after the two-week training period (Table 4).
Spatio-temporal parameters before (T0) and after (T1) training in the whole study sample
Spatio-temporal parameters before (T0) and after (T1) training in the whole study sample
Note. Values are mean±standard deviation (SD). Abbreviations: GC, gait cycle. *Significant at p < 0.05.
Spatio-temporal and kinematic parameters in Group 1 and Group 2 before (T0) and after (T1) training intervention
Note. Values are mean±standard deviation (SD). Group 1, pyramidal positive patients; Group 2, cerebellar positive patients. Abbreviations: GC, gait cycle. *Significant at p < 0.05.
Differences in spatio-temporal and kinematic parameters between two subgroups of patients, Group 1 and Group 2, before (T0) and after (T1) training intervention
Note. Values are mean±standard deviation (SD). Group 1, pyramidal positive patients; Group 2, cerebellar positive patients. Abbreviations: GC, gait cycle. **Significant at p < 0.01.
As regard knee biomechanics, we observed a statistically significant increase in angular excursion (45,63±8,9 at T0 vs 49,26±8,68 at T1) after rehabilitation treatment in the whole study sample (Fig. 1a, b). No significant difference was revealed in hip and ankle angular excursions after TOCT in the whole study sample (Fig. 1a, b).
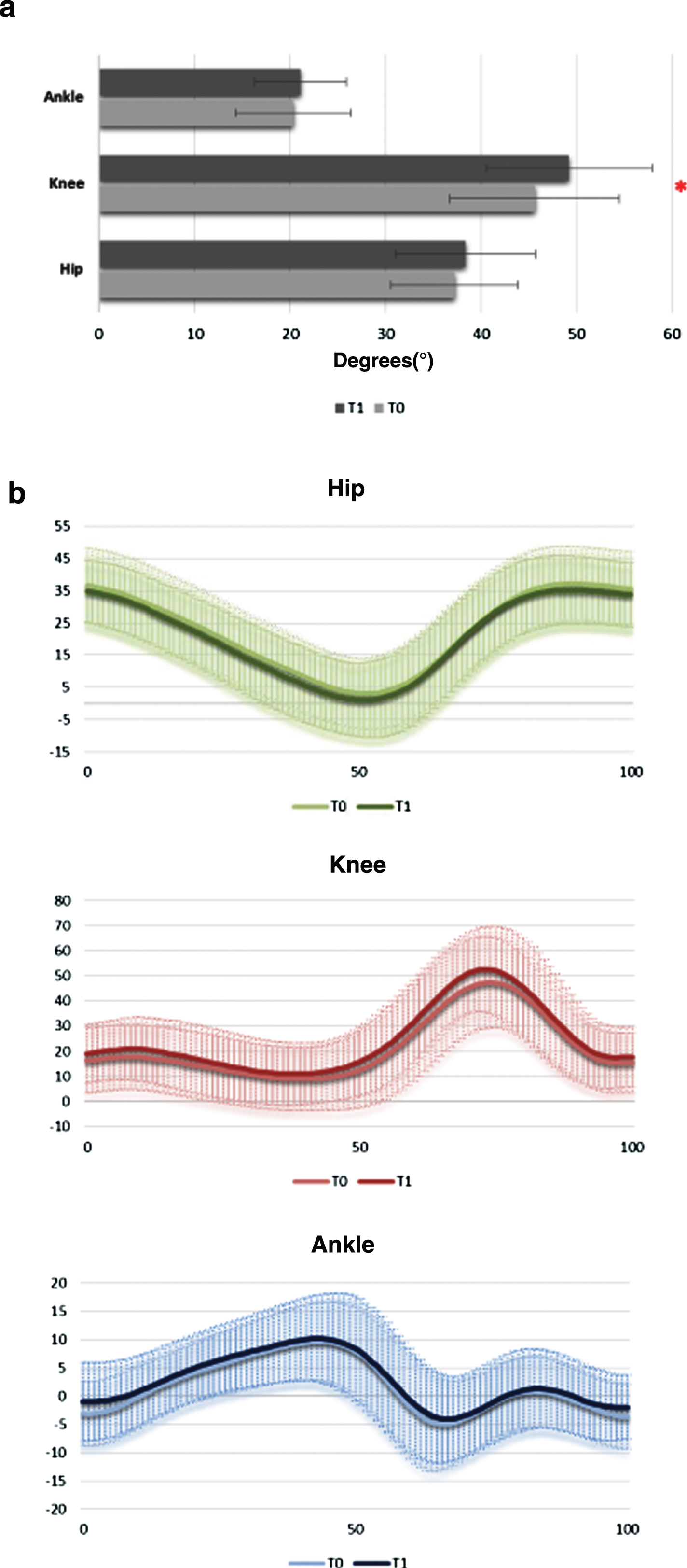
Hip, Knee and Ankle ROM (a) and kinematics (b) before (T0) and after (T1) training in the all study sample. *Significant at p < 0.05.
When considering the two subgroups of subjects, we observed, after training, a statistically significant increase in knee dynamic excursion in Group 1 (43,27±10,34 at T0 vs 48,03±10,40 at T1) but not in Group 2 (48,87±5,43 at T0 vs 50,96±5,77) (Table 3). While, ROMs at all lower extremity joints did not significantly modify between Group 1 and Group 2 after (T1) training intervention (Table 4).
As regard sagittal plane kinematics, we found that at T1 Group 1 patients presented a peak ankle plantarflexion angle (PAPA_ES) in the early stance (PAPA_ES = –5,28±5,03 at T0 vs PAPA_ES = –1,66±5,3 at T1; p = 0.026) and a peak ankle dorsiflexion angle (PADA_TS) in terminal stance significantly higher (PADA_TS = 9,60±3,64 at T0 vs PADA_TS = 12,37±5,19 at T1, p = 0.008), (Table 5). As regard knee dynamics, we found a significant increase in peak knee flexion angle (PKFA) after TOCT training (PKFA = 53±12,40 at T0 vs PKFA = 58,81±10,45 at T1; p = 0.021). While, when considering Group 2 patients, sagittal plane kinematics revealed no significant changes in ankle, knee and hip biomechanics (Table 5, Fig. 2).
Ankle, knee and hip biomechanics in Group 1 and Group 2 before (T0) and after (T1) training intervention
Note. Values are mean±standard deviation (SD). Group 1, pyramidal positive patients; Group 2, cerebellar positive patients. Abbreviations: PAPA_ES, peak ankle plantarflexion angle in early stance; PADA_TS, peak ankle dorsiflexion angle in terminal stance; PAPA_TO, peak ankle plantarflexion angle at toe-off; PADA_S, peak ankle dorsiflexion angle in swing; PKEA, peak knee extension angle; PKFA, peak knee flexion angle; PHEA, peak hip extension angle; PHFA, peak hip flexion angle; *Significant at p < 0.05.
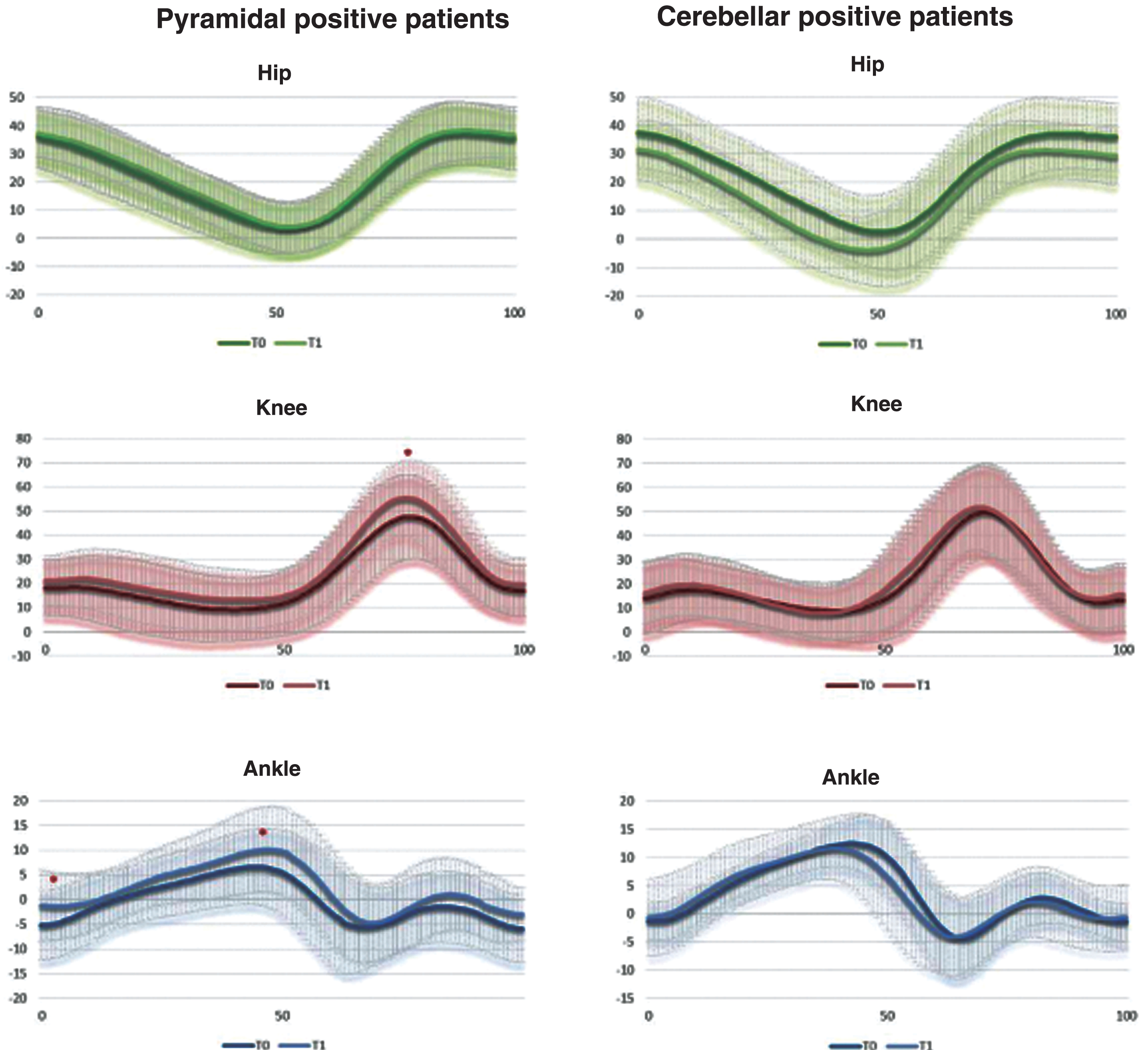
Hip, knee and ankle kinematics in Group 1 and Group 2 before (T0) and after (T1) training intervention. *Significant at p < 0.05.
Moreover, when comparing ankle kinematics in the two subgroups of participants, we found that peak ankle dorsiflexion angle in terminal stance (PADA_TS = 9,60±3,64 in Group 1 vs PADA_TS = 14,17±3,14 in Group 2; p = 0.01) and peak ankle dorsiflexion angle in the swing time (PADA_S = 1,93±3,99 in Group 1 vs PADA_S = 7,73±4,33 in Group 2; p = 0.01) were significantly lower in Group 1 before TOCT training (Fig. 3). While, after TOCT training, peak ankle dorsiflexion angle in terminal stance (PADA_TS = 12,37±5,19 in Group 1 vs PADA_TS = 13,68±5,21 in Group 2; p = 0.45) and peak ankle dorsiflexion angle in the swing time (PADA_S = 2,80±6,08 in Group 1 vs PADA_S = 5,54±6,12 in Group 2; p = 0.41) were not significantly different between the two subgroups of subjects (Fig. 3).
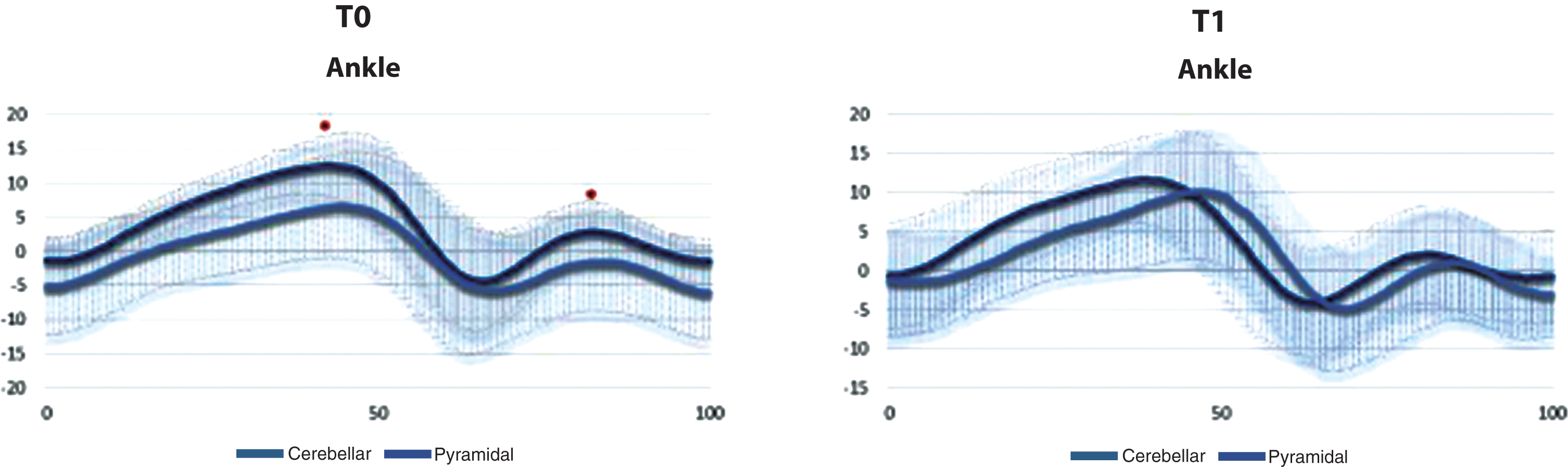
Sagittal plane ankle kinematics at two time intervals (T0 and T1) in the two subgroups of patients (Group 1 and Group 2). *Significant at p < 0.05.
The importance of addressing ambulatory function in people with MS is gaining interest, and different rehabilitative training programs have been proposed to improve motor performance and quality of life. Since our previous findings evidenced the efficacy of a gait specific training on functional abilities and health related quality of life in MS, we investigated gait characteristics changes induced by this rehabilitation treatment. In particular, we tested two main hypothesis: 1) motor improvement induced by the intervention may be associated to positive modifications in gait biomechanics; 2) patients with a specific neurological involvement, assessed with clinical scores, may reveal specific gait improvements after TOCT training intervention.
In the whole sample of patients, our findings confirmed the results reported in previous studies, i.e. decreased gait velocity, shorter steps, increased double limb support and step width and reduced dynamic excursion at all lower-extremity joints (Kabada et al. 1990, Severini et al. 2017).
As regard spatio-temporal parameters, we did not evidence any improvement in the whole study sample after rehabilitation intervention. Anyway, we found an increased walking velocity, reduced double limb support time and stance time duration in Group 2 compared to Group 1, after the two-week training period. As known, these parameters represent measures of walking stability: MS people usually increase double limb support time and stance duration time to compensate for fear of falling or postural instability (Sosnoff et al. 2012). Therefore, despite the fact that no relative improvement was evidenced in Group 2, we revealed that patients with prevalent cerebellar impairment displayed a less conservative gait strategy compared to patients with prevalent pyramidal impairment after training period.
The main findings of the present study are related to knee kinematics. In fact, we found that knee range of movement was significantly improved after the specific training approach in the whole study sample, moving its value towards normality parameters (Kabada et al. 1990). The novelty of our data is the fact that a two-week intensive program positively modified knee angular excursions in mild impaired MS subjects. It might be hypothesized that a combination of factors, such as treadmill training associated with repetitive task-specific goals in the TOCT program, contributed to changes in knee biomechanics. In fact, recently, it was discussed that treadmill training is capable of affecting the functional ROM of the lower limbs during walking in MS people and the gains in kinematics and kinetics of gait reflect improved functional abilities during motor performance (Peruzzi et al. 2017). In our study, task-specific repetitive exercises required the participants to a more coordinated and forceful moving, reaching higher degrees of joint excursions. From a rehabilitative point of view, previous studies pointed out the main effect of rehabilitation interventions occurring on spatio-temporal parameters recorded with Gait Analysis (Guner et al. 2015, Gutierrez et al. 2005). To our knowledge, only a short-term yoga program, comprehending an aerobic training on bicycle, induced a trend in improvement in dynamic range of movement of lower limb joints (Pau et al. 2017). In summary, our advice is that including a relevant amount of treadmill training, along with task-specific exercises in a rehabilitation intervention, may have clearly identifiable benefits on gait biomechanics in mild-moderate impaired MS people.
The second part of our study focused on identifying differences in ambulatory pattern induced by the specific training in two subgroups of patients, divided on the basis of clinical functional examination.
Interestingly, these data point out that patients with prevalent pyramidal impairment could gain more profit by the intensive task-specific training, presenting a better knee dynamic excursion, supported by an improved knee and ankle kinematics during normal walking. In particular, during early stance, we found a reduced plantarflexion at the beginning of single limb stance. Thus, this subgroup of patients exhibited a gait pattern with the foot landing on the ground in a less plantar-flexed position. Overall, this joint position could reduce the requirement of the ankle dorsiflexors to control the plantar flexion movement during early stance (Huisinga et al. 2013). While peak plantar flexion at toe-off did not change after the two-week training period, peak dorsiflexion angle during late stance increased after training period, so we might suppose that the angular distance traveled by the ankle was higher and the amount of torque generated could be increased. Consequently, knee biomechanics revealed an improved peak flexion during the swing time of gait cycle, which turned in increased knee dynamic excursion during normal walking. Of note, when comparing ankle biomechanics between two subgroups of subjects, we found greater peak ankle dorsiflexion angle during late stance and in the swing time of gait cycle in pyramidal positive subjects, thus supposing an improved toe-clearance.
These results may have important implications in the treatment approach of such patients. In the light to assist the decision making process on training intervention in MS, these findings suggest TOCT training as a treatment opportunity to improve gait kinematics and ambulatory pattern in MS patients with a prevalent pyramidal impairment. Indeed, the significant modifications in terms of knee and ankle kinematics represent clinically meaningful changes, stating current literature on minimum detectable differences of gait kinematics in MS population and healthy subjects (Andreopoulou et al. 2019, Bates et al. 2016). Therefore, these results point out the transferability of the training program to the ambulation function with potential benefits on clinical outcomes. As known, gait pattern in MS patients is affected by abnormal strategies for mechanical work generation to compensate neuromuscular impairments (Davies et al. 2016). In particular, the reduction of knee flexion pattern and ankle dorsiflexion in the swing phase of gait cycle represent two frequently altered dynamics in MS (Nogueira et al. 2013), exposing patients to increased risk of falling due to tripping or crossing obstacles (Cofrè et al. 2016). Indeed, abnormal foot kinematics, especially the lack of push-off power at the ankle, results in an inefficient knee flexion velocity and induce an increased energy cost leading to an inefficient gait pattern (Campanini et al. 2013). In this regard, gait analysis evaluation allow the identification of specific gait abnormalities in individual patients, and may help to plan goal-oriented physical therapy. Therefore, this kind of approach may help physicians to plan rehabilitation needs and target treatment options.
Some limitations of this study have to be acknowledged: first of all, the sample size may have played a role in limiting the significance of some of the statistical comparisons carried out. Of note, we carefully evaluated the possible presence of outliers, which are likely to affect statistical analyses when the number of patients is limited, and no evidence of outliers was found in our sample for quantitative data. Another limitation to consider is that recordings were made in a setting of short-medium dimensions. Probably, the inclusion of a fully comparable control group attending a conventional rehabilitative treatment could be useful in order to confirm that the obtained results are due to the specificity of our rehabilitative approach. Finally, future perspective will be to assess gait kinematics in a large cohort of patients with a longer follow-up in order to verify whether quantitative changes persist along time and to confirm the generalizability of such an approach.
Conclusions
In conclusion, results provide evidence that the intensive task-specific protocol can be an effective approach to positively modify lower limb kinematics in mild-moderate impaired MS patients. Moreover, kinematic data suggest TOCT training as a treatment opportunity to improve gait kinematics and ambulatory pattern in MS patients with a prevalent pyramidal impairment.
Authors’ contribution
CT performed patients’ recruitment, clinical evaluations and gait analysis procedure, contributed to data analysis, interpreted the results and drafted the manuscript; SDM contributed to clinical evaluations and gait analysis procedure; CC designed the study, was responsible for patients’ enrolment and clinical functional evaluations, contributed to analysis and interpretation of data and to manuscript supervision. The authors read and approved the final manuscript.
Conflict of interest
I declare that each author participated sufficiently in the work to take public responsibility for the content. I affirm that I had access to all data from the study, both what is reported and what is unreported, and also that I had complete freedom to direct its analysis and its reporting, without influence from sponsors. I also affirm that there was no editorial direction or censorship from the sponsors. No part of this work has been published. No conflict of interest exists.
Footnotes
Acknowledgments
We would like to thank the physiotherapists Alessandra Scolari who assisted the patients during the treatment.