
Abstract
BACKGROUND:
With the recent developments in science, full-immersion virtual reality devices have been developed, which may have feasibility for stroke rehabilitation.
OBJECTIVE:
This case report investigated the feasibility of training using a full-immersion virtual reality video game for improving motor function, balance, and gait in a young stroke survivor.
METHOD:
The case was a 27-year-old woman with stroke. A training using full-immersion virtual reality video game (Sony PlayStation®VR) was performed for 30 minutes per session, 3 sessions per week, for 6 weeks, with a total of 18 sessions. Before training and at each training for 6 weeks, with a total of 19 times, the motor function, balance, and gait were assessed using the Motor Assessment Scale (MAS), Berg Balance Scale (BBS), Timed Up and Go (TUG) Test, and Tinetti Balance Assessment, 10 Meter Walk Test (10MWT), Tinetti Gait Assessment, and Dynamic Gait Index (DGI).
RESULTS:
During the training, there were no adverse events reported. The case achieved 14 points higher than the pre-assessment with 34 points on the MAS, 16 points higher than the pre-assessment with 48 points on BBS, 6.85 sec lower than the pre-assessment, with 13.58 sec on TUG, 5 points higher than the pre-assessment with 13 points on the Tinetti Balance Assessment, 5.36 sec lower than the pre-assessment, with 8.15 sec on the 10MWT, 4 points higher than the pre-assessment with 10 points on the Tinetti Gait Assessment, and 10 points higher than the pre-assessment with 21 points on the DGI.
CONCLUSION:
This case report suggests that training using a full-immersion virtual reality video game may be a safe and effective method to improve motor function, balance, and gait in a young stroke survivor.
Introduction
Impairments resulting from strokes can include a decrease of level of consciousness, cognition, and perception, sensory functions impairments, muscle weakness, abnormal muscle tone, postural control and balance impairments, and abnormal gait pattern (Liston & Brouwer, 1996; de Haart et al., 2004; Sharp & Brouwer, 1997). Recovery of these functions are important goals in rehabilitation, and various interventions are needed to improve these functions.
Virtual reality training is considered as an interesting approach in rehabilitation for functional recovery, having the advantages of motivation and independence (Massetti et al., 2018). If one wears a virtual reality headset, one is provided with a virtual environment from a device producing 3D graphic or image and operates motions through a motion recognition camera and controller, in which one can feel immersion and reality as if one were actually there (Lledo et al., 2016).
Virtual reality is classified broadly into non-immersion, semi-immersion, and full-immersion virtual reality. According to the degree of sensory immersion, full-immersion virtual reality can display a variety of sensory information in virtual reality, significantly limiting the perception of the real world. However, non-immersion or semi-immersion virtual reality is used to provide virtual reality information and yet allow maintaining flexibility of operation and recognition of the real world (Salazar, 2011). With the availability of virtual reality devices, video games on devices such as the Nintendo Wii and Kinect Xbox are often used at home. These video games use a virtual reality device comprising 2D or simple 3D graphics or images (Sin and Lee, 2013; Chow et al., 2013; Manlapaz et al., 2011; Adie et al., 2017); this is semi-immersion virtual reality, and since these video games cannot provide complete immersion and reality experience as done by full-immersion virtual reality, there is a limitation in displaying the sensory ability to the maximum.
With the recent developments in science, full-immersion virtual reality devices have been developed that can resolve the limitation of non-immersion and semi-immersion virtual reality devices (Leem & Woo, 2016). Full-immersion virtual reality devices produce vivid complete 3D images, and are much more enhanced compared to the existing non-immersion or semi-immersion virtual reality devices. Thus, a full-immersion virtual reality device can be a better rehabilitation tool than the existing non-immersion or semi-immersion virtual reality devices. However, few studies implementing full-immersion virtual reality devices have been conducted. Moreover, a study investigating the feasibility of training using video games implementing full-immersion virtual reality on stroke survivors has not yet been conducted. It was reported that the training using virtual reality could cause a side effect called visually induced motion sickness (VIMS) (Keshavarz et al., 2015), and the symptoms of VIMS are considered similar to those of general motion sickness, including nausea, vomiting, drowsiness, dizziness, fatigue, cold sweat, and eye movement discomfort (Lawson, 2001). Hence, careful monitoring must be done when applying the training using full immersive virtual reality in rehabilitation. We therefore tried to investigate the feasibility of training using a full-immersion virtual reality video game in a stroke survivor. This study aimed to investigate an adverse side effects of full immersive virtual reality training and effects on motor function, balance, and gait in a young stroke survivor.
Methods
Participant
The participant was a 27-year-old female hemiplegic stroke survivor (height, 158.20 cm; weight, 56.20 kg). The case was diagnosed with left hemiplegia that occurred 21 months earlier. At that time, the participant was transported to an acute care hospital due to sudden loss of strength in the body and was subsequently diagnosed with cerebral infarction. She underwent medical care and rehabilitation and was referred to an outpatient rehabilitation hospital. The participant did not have any disease other than stroke. She had neither taken medications nor had had surgery for a long time. Her rehabilitation goal was to be able to achieve functional recovery to the pre-disease level and subsequently resume her job as a nutritionist.
Outcome measures
The motor function, balance, and gait before training using full immersive virtual reality and at each training for 6 weeks, with a total of 19 times. The Motor Assessment Scale (MAS) was used to assess motor functions; Berg Balance Scale (BBS), Timed Up and Go (TUG) Test, and Tinetti Balance Assessment were used to assess balance; and 10 Meter Walk Test (10MWT), Tinetti Gait Assessment, and Dynamic Gait Index (DGI) were used to assess gait. The MAS is a tool developed by Carr et al. (1985) to evaluate functional task performance ability of stroke patient, which comprises a total of eight subitems, and each item is scored between 0 (not being able to perform) and 6 points (perform completely). The BBS is used to test the balance and comprises 14 items with 56 points maximally, applying daily life activities including sitting, standing, weight shifting, and etc. (Blum & Korner-Bitensky, 2008). The TUG is a tool to assess functional mobility and balance, and measures the time taken by the subject to do the following: sit on a chair with armrests, rise from the chair at the start signal, walk 3 meters, come back, and sit on the chair (Flansbjer et al., 2005). The Tinetti Balance Assessment is a tool developed by Tinetti to determine the fall risk of an older individual and assess their balance (Tinetti & Ginter, 1988). The 10MWT is a tool to calculate gait velocity, and measures the time taken to perform the task of walking 10 meters at a safe speed (Salbach et al., 2001). The Tinetti Gait Assessment has usually been used to evaluate mobility and fall risk of older individuals, and comprises eight tasks, on a 2- to 3-point scale (Canbek et al., 2013). The DGI is a tool used to examine the gait ability (Jonsdottir & Cattaneo, 2007).
Clinical impressions
The MAS, which was used to evaluate motor function, was 20 points, and her gait, upper extremity function, hand movement, and delicate hand activity were limited. The BBS was 32 points. She had moderate fall risk, and the TUG was 20.43 sec, which was slower than that of healthy older individuals. The Tinetti Balance Assessment was 8 points, and she had limitations when turning 360° and sitting with her eyes closed. The 10MWT was 13.51 sec, which is considered as a limitation in a group activity. The Tinetti Gait Assessment was 6 points, and her symmetry of step, continuity of walking, and trunk stability were poor. Moreover, the DGI was 11 points, and she had limitations in walking on and around an obstacles and climbing stairs, and had a high fall risk. She could relatively move her shoulder and elbow on the more affected upper extremity, but her wrist movement was limited. In addition, she could independently perform the outdoor gait activity but had a limitation in slope walk.
Intervention
Training using a full-immersive virtual reality video game was conducted with Sony PlayStation®VR (Sony Interactive Entertainment Inc., Tokyo, Japan). This video game comprises the system unit, headset, controller, and motion recognition camera (Fig. 1). It can be recognized as the user’s location and movement through the headset with two handheld controllers and a motion recognition camera. For the training with this full-immersion virtual reality video game, two games included in Sony PlayStation®VR were used. The first game was Fruit Ninja (Fig. 2), in which the surrounding background is stationary. In the fixed background, fruits keep coming up from the bottom up to the player, and the player performs the motion of cutting them with the sword, top to bottom, and left to right, using both hands. The second game was Everybody’s Golf, a game in which the player plays golf, holding one controller in a realistic virtual reality environment experiencing the feeling of being on a real golf range (Fig. 2). Fruit Ninja is a game in which the player cuts fruits, using the controller with both hands. However, in this study, the participant was instructed to perform the following: alternating the motion of cutting with both hands and using only the hand on the more affected side to increase the frequency of the use of the more affected side. Everybody’s Golf VR is a game in which the player performs golf swing motions using one controller. In this study, the participant was instructed to swing so that she held the controller on the more affected side, and swung from the more affected side toward the less affected side; she was instructed to perform delicate putting motions to put the ball into the hall, performing swing motions to fly the ball far away and putting motions alternately. Each game was played for 15 minutes, and an approximately 5 min break was provided while the game was changed and the device was set up. The training using full-immersive virtual reality video game was performed for 30 min per session, 3 sessions per week, for 6 weeks, with a total of 18 sessions.

Full immersive virtual reality video game.

Fruit Ninja and Everybody’s Golf games.
The results are summarized in Tables 1, 2, 3 and Figs. 3, 4, 5.
Changes of motor function
Changes of motor function
Abbreviation: Motor Assessment Scale, MAS.
Changes of balance
Abbreviations: Berg Balance Scale, BBS; Timed Up and Go test, TUG; Tinetti Balance Scale, TBS.
Changes of gait
Abbreviations: 10 Meter Walk Test, 10MWT; Dynamic Gait Index, DGI; Tinetti Gait Scale, TGS.
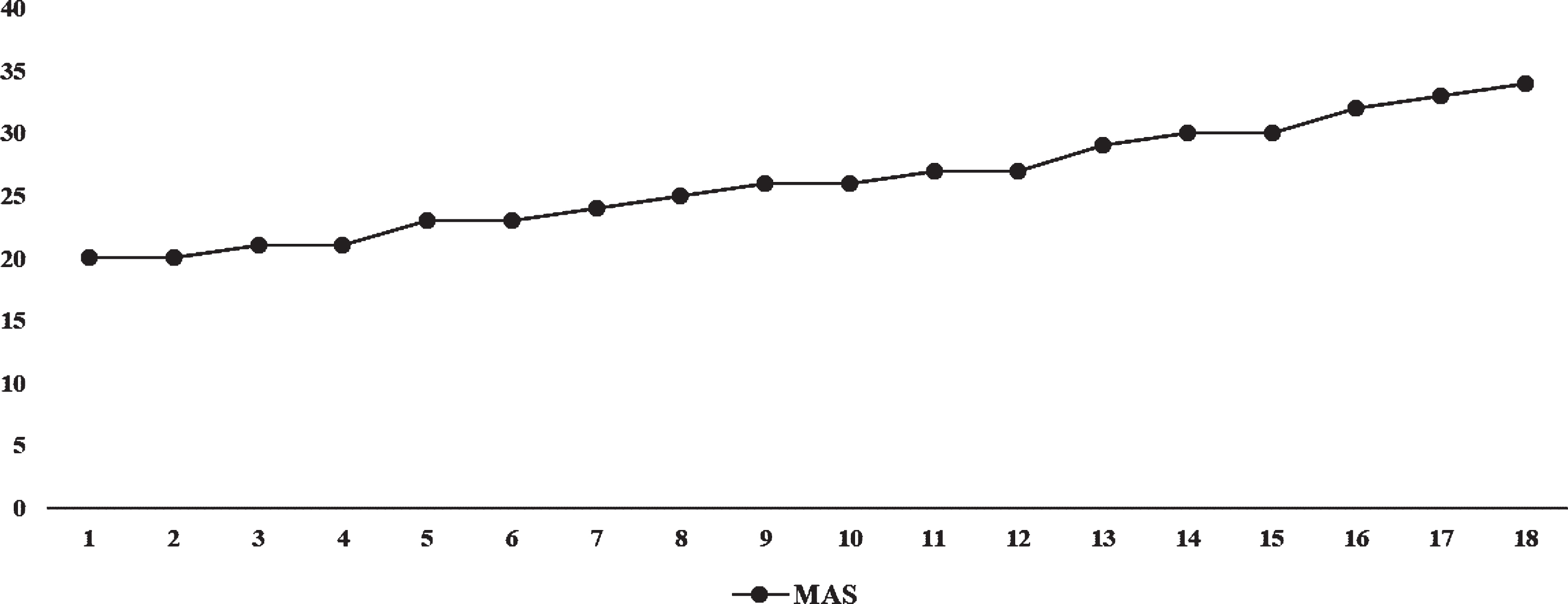
Changes of motor function.
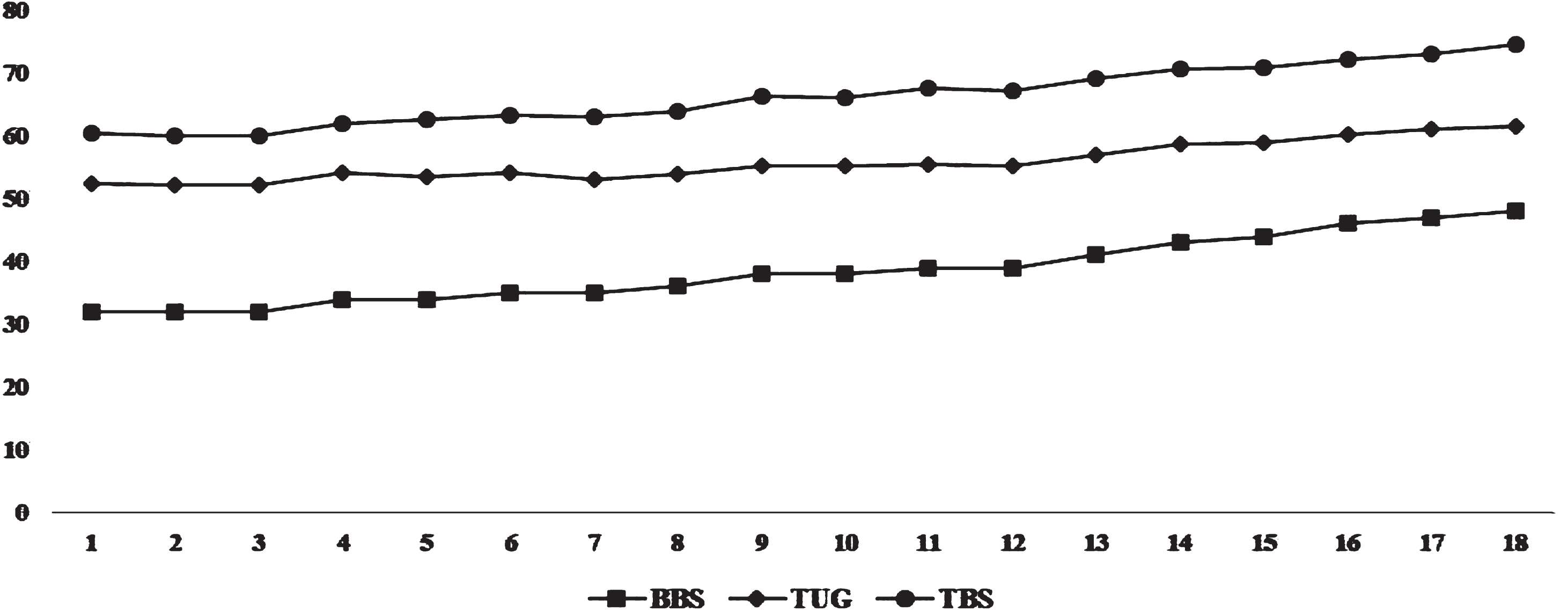
Changes of balance.
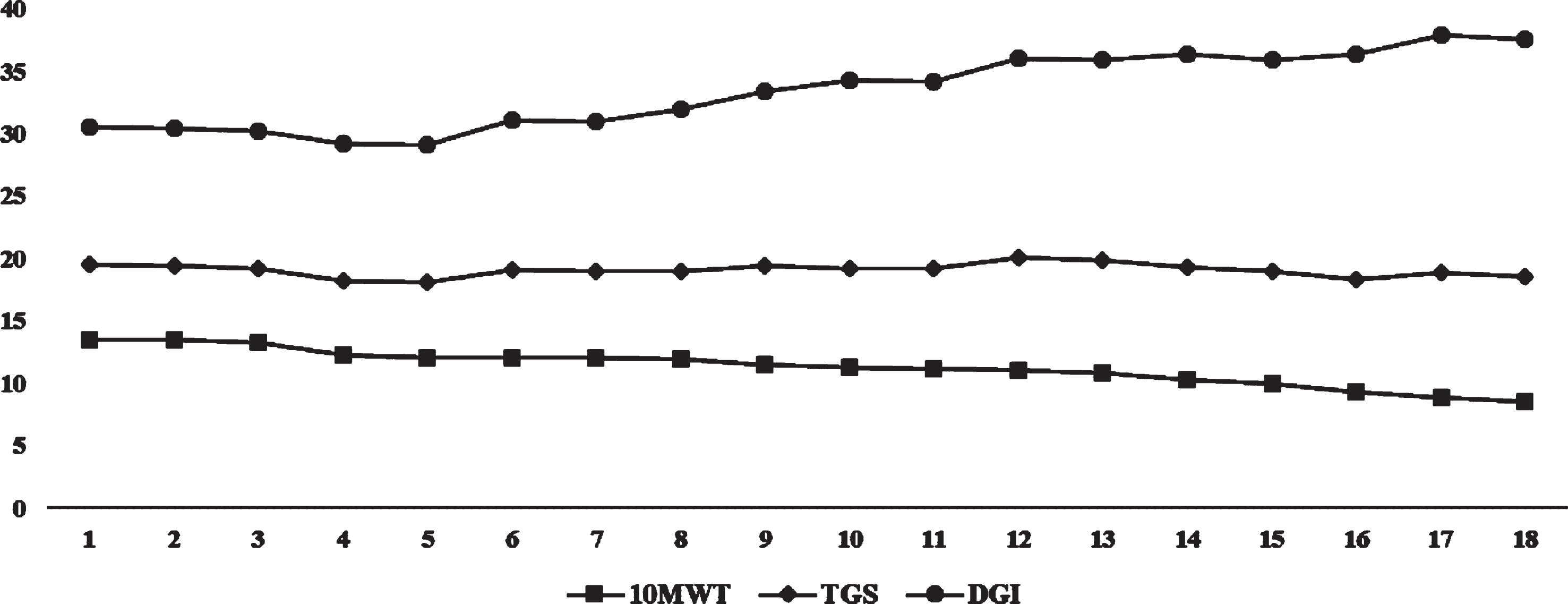
Changes of gait.
During the training using a full-immersive virtual reality video game, there were no significantly adverse events reported. However, occasionally, the participant briefly complained of dizziness and motion sickness.
Regarding motor function, the participant achieved 20 points in the MAS before the first training and 34 points after the final training, with a 14-point (70%) increase (Table 1 and Fig. 3). Regarding balance, the participant achieved 32 points and 48 points in the BBS before the first and after the final training, respectively. It increased by 16 (50%) points. Regarding the TUG, the participant achieved 20.43 sec and 13.58 sec before the first and after the final training, respectively, which was 6.85 sec (33.53%) decrease. Using the Tinetti Balance Assessment, the participant achieved 8 points before the first and 13 points after the final training, which was 5 (62.5%) points higher than before the first training (Table 2 and Fig. 4). Regarding gait, the 10MWT took 13.51 sec before the first and 8.15 sec after the final training, which was 5.36 (39.67%) sec decrease. Using the Tinetti Gait Assessment, the participant achieved 6 points before the first and 10 points in the final training, which was 4 (70%) points higher than before the training. Furthermore, using the DGI, the participant achieved 11 points before the first and 21 points after the final training, which was 10 (70%) points higher than before the first training (Table 3 and Fig. 5).
This case study investigated an adverse side effects of full immersive virtual reality training and effects on motor function, balance, and gait in a young stroke survivor. As a result of the training using the full-immersion video game, which was conducted for a total of 18 times for 6 weeks, improvements in motor function, balance, and gait were observed.
Kim et al. (2012) applied the video game training using Nintendo Wii (Tennis and Boxing Games) on 20 stroke patients for 30 minutes per time, three times a week, for 3 weeks. As a result, it was reported that the MAS, which was used to evaluate motor function, significantly improved, and there was also a significant improvement in modified Postural Assessment Scale (Kim et al., 2012). In the present study, the MAS also was also increased by 70% after the final training compared to before the first training. This result is similar with previous study (Kim et al., 2012). The Nintendo Wii is a simple 3D video game and a device different from that of the full-immersion video game used in the present study. However, Fruit Ninja as the full-immersion video game used in the present study, requires the fast movements of the upper extremity and the trunk to cut the fruits appearing suddenly. To achieve a higher score, such as the player’s motion of cutting from left to right, instead of from top to bottom and using items, and even if the interest increases, various motions are required. Furthermore, since the participant can get feedback for her movements visually while playing the game she can correct the movements herself and get immediate feedback. Hence, the motor function could improve further. According to Zijlstra et al. (2010), the feedback by vision, auditory sense, and tactile sensation promotes the functional recovery of the upper motor neuron injury patients.
In the present study, an increase of 50% in BBS, an increase of 62.5% in Tinetti Balance Assessment, and an increase of 33.53% in TUG after the final training compared to before the first training were observed. These results are similar to the study by van Duijnhoven et al. (2016), who reported through a systematic review and meta-analysis that training using home video games, such as Nintendo Wii and Kinect Xbox, was effective for the improvement in stroke patients. Additionally, it was reported that trainings including balance training, center of gravity movement training, and gait training can be effective to improve balance ability (van Duijnhoven et al., 2016). In the present study, a full 3D device was used, instead of simple 3D devices, such as Nintendo Wii or Kinect Xbox. However, Everybody’s Golf game induces fast and accurate movements, since the player should hit the ball quickly and accurately to send it farther, trunk stability and lower extremity weight shift should be simultaneously considered, and since the participant in the present study should control the trunk herself and be induced to shift the weight for the accurate golf swing, balance ability might improve. Schachten and Jansen (2015) applied golf training to 14 stroke patients––a total of 20 times one hour each time, twice a week, for 10 weeks, and reported that there was an improvement of balance in the experimental group that had the golf training compared to the control group.
In the present study, in the 10MWT, there was improvement by 39.67% on after the final training than before the first training. The Tinetti Gait Assessment and DGI both increased by 70% in the final training. According to Mirelman et al. (2009), training using a virtual reality device (Rutgers Ankle Rehabilitation System and software) and robot for lower extremity was performed with the stroke patients for 4 weeks, and an improvement in walking ability was observed after the training. Specifically, it was reported that a significant improvement in gait velocity was observed in the experimental group that performed virtual reality training with robot for lower extremity compared to the control group using a robot for lower extremity alone. According to de Rooij et al. (2016), the effects of virtual reality training on the balance and walking ability of stroke patients were reported through a systematic review and meta-analysis, and significant improvements in the balance ability of patients who underwent training using virtual reality were observed compared to the control group. Gait is one of the important elements in returning to society and the faster the gait velocity, greater the opportunities for participation in social activities, thus, promoting their quality of life. Particularly, gait in stroke patients is closely associated with balance, and if balance ability improves, walking ability can also improve (An et al., 2017). In the present study, there was an improvement of walking ability along with improvement of balance ability after the training. The training inducing direct gait was not performed and instead training using the full-immersion video game including control of the trunk and the lower extremities to maintain balance in performing movements using the upper extremities was used. In addition, since weight shift training was performed through the Everybody’s Golf game, an improved balance ability was observed. Since instability while walking decreased, consequently, improved walking ability was observed.
As a new rehabilitation method of chronic stroke survivors, this case study suggests that additional studies using a full-immersion video game in the future should be conducted. The full-immersion virtual reality video game was set at a hospital that the participant visited as an outpatient and was operated during conducted the present study without any problems. However, occasionally, the participant complained of dizziness and motion sickness briefly during play the games. Overall, the participant was satisfied with the training.
This study is a case report, thus it is impossible to generalize the results of this study due to the limitation of the study design and the small number of participants. Moreover, long-term follow-up for investigating a feasibility of the training was not performed. Thus, future studies should continuously verify the effects of training using a full-immersion video game through a high quality study.
Author Contributions
Conceptualization, S.H.P. and G.G.L.; methodology, S.H.P. and G.G.L.; formal analysis, D.G.L.; writing—original draft preparation, S.H.P., K.H.C., and S.K.H. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
The authors declare no conflict of interest.