
Abstract
BACGROUND:
Interventions addressing balance dysfunction after traumatic brain injury (TBI) only target compensatory aspects and do not investigate perceptual mechanisms such as sensory acuity.
OBJECTIVE:
To evaluate the efficacy of a novel intervention that integrates sensory acuity with a perturbation-based approach for improving the perception and functional balance after TBI.
METHODS:
A two-group design was implemented to evaluate the effect of a novel, perturbation-based balance intervention. The intervention group (n = 5) performed the intervention with the sinusoidal (0.33, 0.5, and 1 Hz) perturbations to the base of support with amplitudes derived using our novel outcome of sensory acuity - perturbation perception threshold (PPT). The efficacy is evaluated using changes in PPT and functional outcomes (Berg Balance Scale (BBS), Timed-up and Go (TUG), 5-meter walk test (5MWT), and 10-meter walk test (10MWT)).
RESULTS:
There was a significant post-intervention change in PPT for 0.33 Hz (p = 0.021). Additionally, clinically and statistically significant improvements in TUG (p = 0.03), 5MWT (p = 0.05), and 10MWT (p = 0.04) were observed.
CONCLUSIONS:
This study provides preliminary efficacy of a novel, near-sensory balance intervention for individuals with TBI. The use of PPT is suggested for a comprehensive understanding and treatment of balance dysfunction. The promising results support the investigation in a larger cohort.
Keywords
Introduction
Traumatic brain injury (TBI) negatively affects the pathophysiology of multiple systems resulting in balance dysfunction, – a significant motor challenge in everyday life after TBI (Grandhi et al., 2017; Zarshenas et al., 2019; Black et al., 2000). Specifically, TBI impairs the integration and organization of the visual, auditory, and somatosensory inputs and attention that facilitate self-awareness of body position relative to the environment, resulting in balance dysfunction (Allison, 1999). While individuals with TBI experience a broad spectrum of impairments, it is reported that about 83%of individuals with moderate/severe TBI experience impaired balance and altered coordination as well as motor function limitations (Peters et al., 2014). Deficits in balance and coordination, as well as a higher risk of falls, persist years after the diagnosis of brain injury as well and presents a challenge for individuals with TBI to return to independent living in the community (Peters et al., 2014). Poor control of balance after a TBI is characterized by an increased (more than double) postural sway even during quiet stance, which is often indicated by the increased movement of the center of pre-ssure (CoP), especially in the anterior-posterior (AP) direction compared to healthy individuals (Basford et al., 2003). In the functional domain, balance imp-airments translate to poor performance during functional assessments of static and dynamic balance and mobility.
Alleviating balance dysfunction through rehabilitation interventions is a significant challenge because it is generally not known what therapies are effective in individuals with TBI due to variability in the symptoms (Bland et al., 2011). Broadly, intervention strategies vary from physical therapy to exercise, traditional treadmill training to augmented reality (AR) and virtual reality (VR) interventions (Bland et al., 2011; Straudi S. et al., 2017; Tefertiller et al., 2019). A common link between different studies using different types of intervention techniques is their outcome metrics –most studies either use questionnaires, observation-based functional outcomes (e.g., berg balance scale (BBS)), or biomechanical outcomes (movement of the center of mass [CoM], CoP, etc.).
A common goal of balance interventions is to improve balance in individuals to enable functional independence and prevent falls in the community. However, falls due to balance dysfunction may oc-cur due to improper detection and correction of the CoM movement resulting from internal (self-init-iated) or external perturbations. Further, research shows that environmentally induced perturbations combined with attention deficits after TBI negatively affect balance control, putting individuals at a higher risk of falls (Perry et al., 2014). While most studies measure outcomes related to the ‘correction’ phase of falls, there is limited research on the sensory acuity and its relation to balance dysfunction in individuals with TBI. Sensory acuity refers to the ability to detect the body-sway during external perturbation (Fitzpatrick & McCloskey, 1994; Richerson et al., 2006). No literature exists on: 1) quantifying the sensory acuity; and 2) how sensory acuity can be quantifiably included in the balance training to improve postural control after TBI.
Perturbation-based training is a rehabilitation ap-proach that has shown promise to improve balance in older adults and individuals with neurological disorders (Mansfield et al., 2007; EsmaeiliMahani et al., 2018; Steib et al., 2017; Horak et al., 1997). It involves individuals receiving repeated perturbations that force the CoP outside the base of support and aims at producing rapid balance reactions (Mansfield et al., 2017). The perturbations are either induced by a physical therapist’s push/pull or through individuals standing or walking over a computerized platform or treadmill that produces sudden mechanical perturbations to the base of support (Mansfield et al., 2015). Perturbation-based balance interventions have shown promising results to reduce falls in the community, improve balance and individual’s confidence (EsmaeiliMahani et al., 2018; Steib et al., 2017). Perturbation-based interventions can improve gait patterns for individuals with neurological deficits and those whose balance is affected by aging (EsmaeiliMahani et al., 2018; Mansfield et al., 2007). However, investigating the effects and benefits of such a training approach on balance has been focused on individuals with stroke and Parkinson’s disease and such interventions have seldom evaluated individuals with a TBI.
The current investigation aims to provide preli-minary evidence by evaluating the efficacy of a com-puterized biofeedback-based intervention that uses the novel outcome of sensory acuity to present near-sensory perturbation-based intervention for impro-ving balance after TBI. The intervention particularly targets improving sensory acuity by providing near-sensory perturbations to the base of support while targeting lower-extremity efferents through the same perturbations. Sensory acuity is evaluated using a psychophysical outcome measure - perturbation perception threshold (PPT) (Fitzpatrick & McClo-skey, 1994; Richerson et al., 2003; Han et al., 2016). The PPT quantifies the level of external perturbation below which the perception of the stimulus is difficult (Fitzpatrick & McCloskey, 1994). It is reported that individuals with TBI show elevated values for PPT, indicating the diminished sensory acuity to the perturbations at the base of support (Pilkar et al., 2020). The primary outcome measure, PPT, was calculated following procedures similar to psychophysical studies related to the perception of whole-body motion stimuli (Pilkar et al., 2020; Kaernbach, 1990; Han et al., 2016). Additionally, the efficacy of the intervention was evaluated using well-recognized clinical outcome measures of static and dynamic balance and mobility (BBS, 5-meter walk test (5MWT), 10-meter walk test (10MWT) and timed-up and go (TUG)). We hypothesized that the near-sensory perturbations with computerized biofeedback would improve the sensory acuity and functional outcomes of static and dynamic balance in individuals with TBI.
Methods
Participants
Fourteen individuals diagnosed with TBI were randomly assigned to either the control group (TBI-C, n = 9) or the intervention group (TBI-I, n = 5) (Fig. 1). Participants with TBI were included in the study if they were: 1) between 18 and 60 years old; 2) diagnosed with a non-penetrating TBI (≥6 months); 3) able to stand unsupported for at least 5 minutes; and 4) willing and able to give informed consent. Participants with TBI were excluded from the study if they had: 1) a history of injury to their lower limbs in the past 90 days; 2) cardiac disease; or 3) a previous history of balance impairments prior to their TBI. The demographic information of all three groups is presented in Table 1. The Institutional Review Board approved all study procedures, and informed consent was obtained before study participation.

Study CONSORT flow diagram.
Demographics of participants within each group
At the baseline visit, all participants underwent PPT assessments and clinical assessments of static and dynamic balance. A follow-up visit took place approximately one month after the baseline visit and included the same procedures as the baseline visit. Immediately after the baseline visit, the TBI-I group underwent a computerized biofeedback based intervention that consisted of 4 sessions per week over a period of 4 weeks (16 sessions). During all clinical assessments of static and dynamic balance, a member of the study team provided non-contact guarding to all participants, and during all other assessments and intervention procedures, participants wore a safety harness that prevented the individual from falling without hindering their movement.
Sensory acuity assessments–perturbation perception threshold (PPT)
The NeuroCom Smart Equitest Clinical Research System (CRS) (Natus Medical Inc., Pleasanton, CA, USA) was used to provide perturbations to the base of support. Participants wore a body harness and stood on the NeoroCom platform. Participants wore shoes for all trials, and their feet were positioned on a moving platform that provided perturbations in the AP direction. While standing on the NeuroCom platform, participants experienced perturbations at three selected frequencies (0.33 Hz, 0.5 Hz, and 1 Hz). Th-ese frequencies were chosen to keep the perturbations within the range of natural healthy sway frequencies(<2Hz) (Soames & Atha, 1982). For each perturbation frequency, a total of 21 trials were per-formed, consisting of a randomized set of 14 perturbation trials and seven non-perturbation trials. Each trial lasted 15 seconds - consisting of 5 seconds of quiet standing (QS), followed by 5 seconds of sinusoidal translation in the AP direction at the selected perturbation frequency and amplitude (or 5 seconds of no movement for a non-perturbation trial), followed by an additional 5 seconds of QS. At the end of each trial, participants were asked to provide a yes or no response to the question of whether they had felt the platform move. Each trial’s response was classified as either a HIT: correct detection of the perturbation, MISS: failure to detect the perturbation, Correct Rejection: correctly reported the lack of perturbation, and False Alarm: perturbation reported when no perturbation occurred. Each trial’s response was used to adjust the perturbation amplitude of the next trial by utilizing the Single Interval Adjustment Matrix (SIAM) algorithm (Kaernbach, 1990; Pilkar et al., 2016). After completing all 21 trials for a given frequency, a sigmoid function was fit to the data, and a psychometric curve was plotted using the percentage of correctness (HIT and Correct Rejections) as a function of perturbation amplitude (Algom et al., 1992; Puntkattalee et al., 2016). Based on the sigmoid curve for each frequency, the perturbation amplitude (x-axis) that corresponded to a 75%probability of correct detection (y-axis) was chosen as the perceived perturbation threshold (PPT) (Algom et al., 1992; Puntkattalee et al., 2016). The PPT represents the perturbation amplitude at which the sinusoidal perturbation was perceived by the participant for the selected frequency. These procedures were repeated for each of the three perturbation frequencies (0.33 Hz, 0.5 Hz, and 1 Hz). The additional details on the PPT assessment are reported elsewhere (Pilkar et al., 2020).
Clinical assessments of static and dynamic balance
At baseline and follow-up visits, static and dyn-amic balance and mobility were assessed using the Berg Balance Scale (BBS), Timed-up and Go (TUG), 5-meter walk test (5MWT), and 10-meter walk test (10MWT) for all groups. The BBS is a 14-item ass-essment scale, with a maximum score of 56 points that quantitatively assesses balance during static and dynamic functional movements in adults. The 5MWT and 10MWT are the evaluations of walking speed over standard distances, and the TUG evaluates participant’s mobility through the task that includes a transition from sitting to brief locomotion and then return to a seated position.
Perturbation-based biofeedback intervention
Participants in the TBI-I group underwent a 4-week perturbation-based computerized biofeedback intervention that entailed task-oriented balance training during both QS and perturbed stance. The setup (Fig. 2) consisted of a translating platform (NeuroCom CRS) on which the participants stood, and a projector screen in front of the participant (approximately 6 ft away). Motion capture markers attached to anatomical locations of individuals were used to compute CoM (using Cortex, Motion Analysis Corporation, Santa Rosa, CA, USA) in real-time. During each trial, the computed participant’s CoM was projected on the screen in real-time (shown visually as a red dot). As a balance task during QS, the participant was asked to maintain the CoM within the targeted area (shown as a red circle). The diameter of the target area for the first trial was customized based on the QS sway area in both AP and medial-lateral directions, and the target area was reduced by 20%after each trial. For balance training during QS, the platform was kept at rest and participants were asked to maintain the projected CoM within the targeted area for a pre-programmed duration of 1 minute. A total of 10 QS trials were performed during each intervention session. The balance training during QS was followed by perturbation-based training. The platform perturbation frequencies used at baseline (0.33, 0.5, and 1 Hz) were used for perturbations during intervention training as well. Each frequency set consisted of 30 trials (with each trial lasting 15 seconds). The amplitudes for these trials were selected based on PPT obtained at baseline. Perturbation amplitudes for the trials were customized for each participant based on their baseline PPT values and were set at 15%above the PPT (10 trials), at PPT (10 trials) and 15%below PPT (10 trials). During each trial, the platform moved in the same manner as described in the PPT assessment section. The system had the ability to pause the intervention at any moment in order to allow participants to rest if requested or needed as well as in case of an adverse event. All the 30 trials for each frequency were executed continuously unless a pause/rest was requested or required by the participant. After completing 30 trials of each frequency, participants received a 2-minute rest before starting with the next frequency trial set. Participants were harnessed during each intervention session.
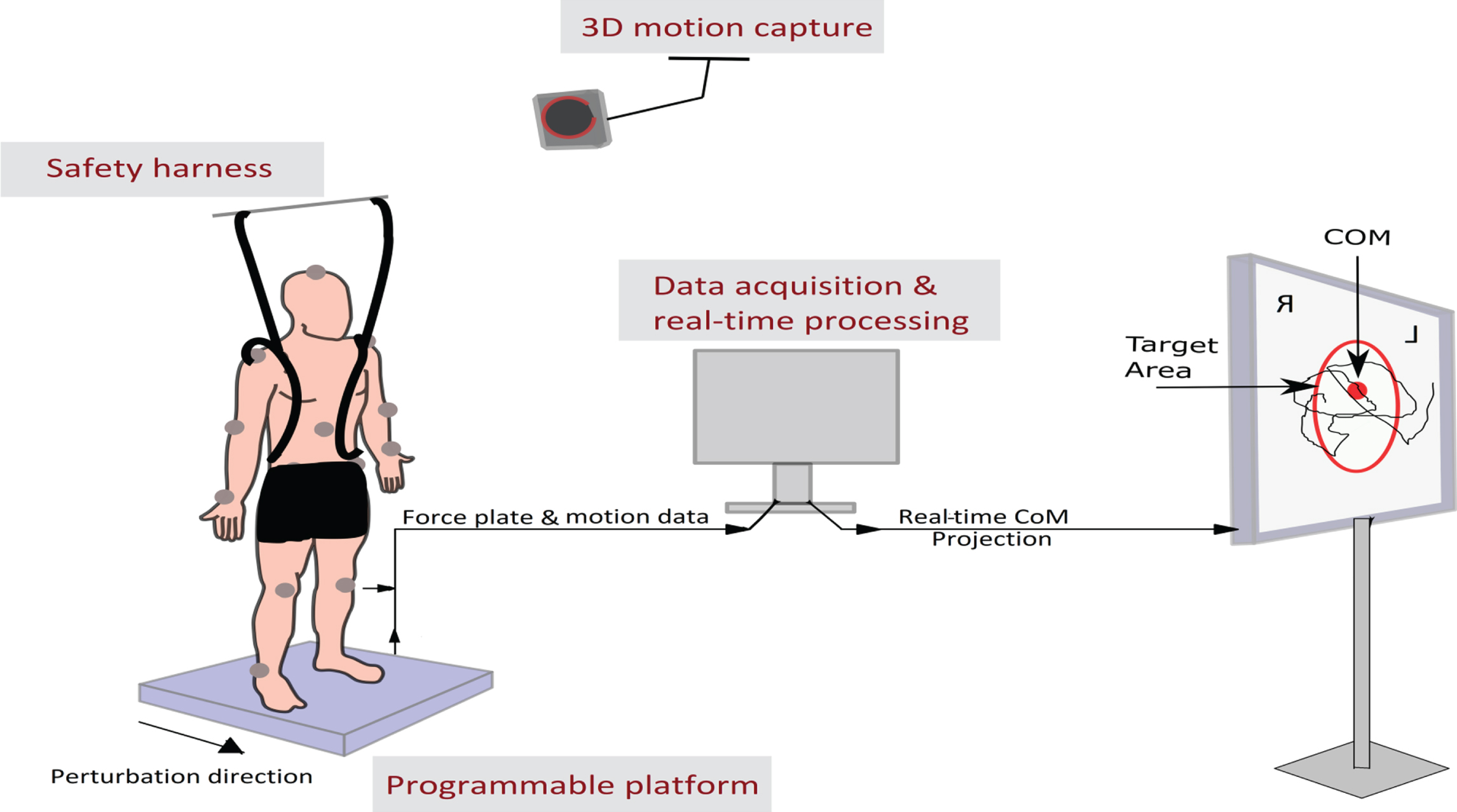
Set up for perturbation-based balance intervention with computerized biofeedback.
We hypothesized that the TBI-I group would show decreased PPT values at follow-up along with improved clinical assessments compared to their baseline values, while the TBI-C group will have no significant difference in PPT scores and clinical assessments at baseline and follow-up. Therefore the PPT data from baseline and follow-up assessments were analyzed using paired sample t-tests for each frequency (0.33 Hz, 0.5 Hz, and 1 Hz) among individuals within TBI groups. The clinical assessments of BBS, 5MWT, 10MWT, and TUG were also compared between baseline and follow-up assessments.
Results
Table 2 shows the results for the PPT assessme-nts performed at baseline and follow-up for both TBI groups. Paired samples t-tests showed a signi-ficant difference between the baseline PPT (mean =1.99, SD = 0.98) and follow-up PPT (mean = 1.41, SD = 0.77) at 0.33 Hz (t(4) = 3.69, p = 0.021) for the TBI-I group. For the TBI-I group, paired t-test to compare 0.33 Hz PPT data achieved the power of 80%(the effect size of 1.66 calculated using mean and SD of differences). No significant difference was observed between baseline PPT (mean = 1.85, SD = 0.85) and follow-up PPT (mean = 1.40, SD = 0.61) at 0.5 Hz (t(4) = 1.89, p = 0.13) and between baseline PPT (mean = 0.89, SD = 0.58) and follow-up PPT (mean =0.78, SD = 0.35) at 1 Hz (t(4) = 0.76, p = 0.49) for the TBI-I group. No significant difference was observed for the TBI-C group at any frequency (Table 2). Figure 3 shows the mean PPT values for the control and intervention groups at baseline and follow-up.
Functional measures of static and dynamic balance and mobility at baseline and follow-up
Functional measures of static and dynamic balance and mobility at baseline and follow-up

Mean PPT values for intervention and control groups at baseline and follow up visits.
Paired t-tests showed a significant improvement (t(4) =–3.35, p = 0.03) in speed for the 5MWT bet-ween baseline (mean = 1.15, SD = 0.32) and follow-up (mean = 1.35, SD = 0.39) for the TBI-I group. The paired t-tests showed that the speed of walking during 10MWT significantly improved (t(4) =–2.78, p = 0.05) between the baseline (mean = 1.22, SD = 0.37) and follow-up (mean = 1.40, SD = 0.38) assessments for the TBI-I group. A significant improvement (t(4) = 2.97, p = 0.04) was also measured in the TUG between the baseline (mean = 12.38, SD = 3.60) and follow-up (mean = 11.32, SD = 2.99) assessments for the TBI-I group. The improvements in 5MWT and 10MWT from baseline to follow-up assessments were also clinically significant as a change in gait speed of 0.1 m/sec to 0.2 m/sec is considered to be clinically significant for individuals with pathology (Bohannon et al., 2014). No statistically significant differences were observed between baseline and fol-low-up using paired t-tests for the BBS and TUG after the intervention. None of the clinical assessments were clinically or statistically different between baseline and follow-up for the TBI-C group. Table 2 provides results of the functional assessments of both the TBI-I and TBI-C groups at baseline and follow-up.
The primary objective of this investigation was to provide preliminary evidence on the effect of near-sensory perturbation-based intervention with biofeedback for individuals with chronic TBI. To our knowledge, this study is the first to examine the efficacy of perturbation-based balance intervention to improve sensory acuity and balance function for individuals with TBI. The 4-week intervention used in the current study resulted in a decrease in the PPT scores for individuals in the TBI-I group (Fig. 4). Improvement in the PPT scores (sensory acuity) at follow-up was seen for all TBI-I participants at 0.33 Hz, which is the lowest frequency tested. PPT also improved in 4 out of 5 intervention participants for the 0.5 Hz frequency. One participant who was assessed at the age of 35 with time since the injury of almost ten years at the time of assessment showed an increase in the PPT from 0.39 at baseline to 0.7 at follow-up. A lot of variability was observed in the baseline PPT scores, which could have resulted in the difference in improvements. Improvements in PPTs seen even in the small sample in this study show that this intervention may have a promising effect on improving the external perturbation detection abilities in individuals with TBI and that PPT as an outcome metric could provide a multi-dimensional understanding of balance in individuals. We also observed clinically significant changes in 3 out of 5 individuals for the 5MWT and 10 MWT assessments after the intervention (Bohannon et al., 2014). We also compared the improvement in the clinical assessments of each participant in the TBI-I group with the respective Minimal Detectable Change (MDC) (MDC for stroke was used for tests where MDC for TBI is unclear). 4 of the 5 participants had a change greater than MDC for the 5 MWT and 10 MWT. Three out of 5 participants also showed improvement greater than the MDC for BBS (Liston, & Brouwer, 1996). All participants had improvements in TUG that were less than the MDC (Flansbjer et al., 2005).
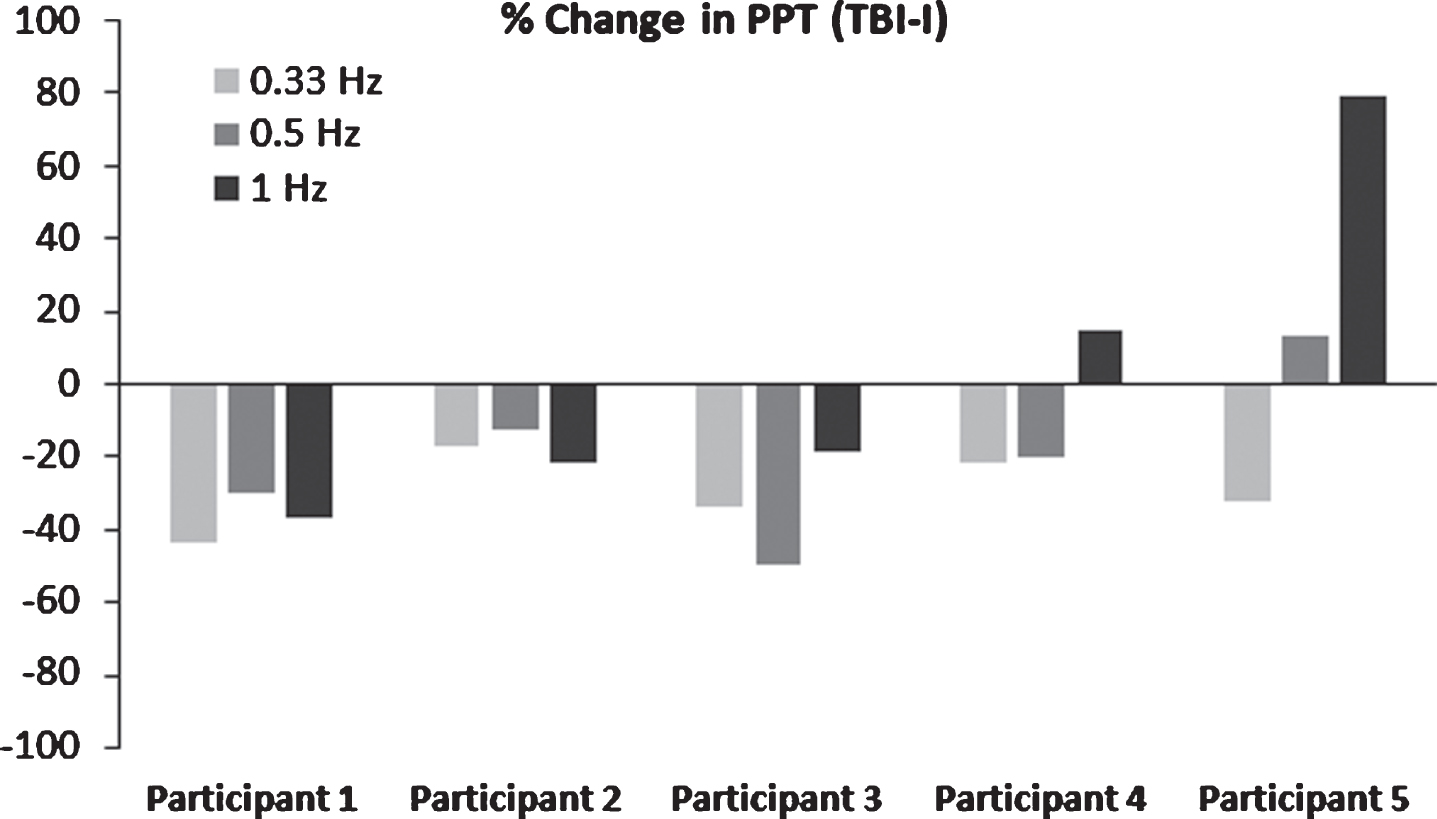
Change in PPT values from baseline to follow-up for each participant in the TBI-I group.
Although the perception of body-sway during self-initiated or externally-triggered movements is an inherent and assumed aspect of many balance interventions, systematic quantification of sensory acuity and its integration as an intervention parameter is missing, making these interventions more focused on the ‘compensation’ than the ‘detection’ of body-sway changes (McCulloch et al., 2010; Straudi S. et al., 2017; Tefertiller et al., 2019). Our intervention bridges this gap by integrating our novel outcome PPT (related to detection) with continuous sinusoidal perturbations (related to compensation). The outcome variable, PPT, quantifies the sensory acuity of individuals. Lower PPT for a set of perturbation frequency suggests a better perceptual ability to support surface perturbations during standing. PPT can either be incorporated into the intervention as done in the current study or used only as an outcome variable used to detect the effect of any intervention on the sensory acuity.
The current study differs from other studies that use perturbation-based balance training to improve balance in individuals with stroke, Parkinson’s or older adults in two ways: 1) The study quantified sensory acuity to perturbations in terms of a novel outcome variable (PPT); and 2) used perturbations with near-sensory amplitudes (<4 mm) and frequencies within the natural sway (<2 Hz) during the intervention. Studies that used perturbation-based balance interventions typically use large perturbation amplitudes and frequencies. For example, Mansfield et al. in their randomized clinical trial for fall prevention in community-dwelling older adults, used perturbations with accelerations of 2.0 m/sec2 and 3.0 m/sec2 with peak velocities of 0.6 m/sec and displacement of 0.18 m (Mansfield et al., 2010). Handelzalts, S. et al. in their randomized clinical trial studying perturbations based balance training in individuals with stroke, used perturbation amplitudes of 10.44 cm to 29.06 cm with velocities ranging from 17.62 cm/sec to 54.17 cm/sec in the AP direction (Handelzalts et al., 2019). In contrast, the maximum perturbation for PPT assessment and balance training used in the current study was 4 mm at the highest frequency of 1 Hz (i.e., a velocity of 4 mm/sec). Fitzpatrick et al., in their study, showed that the visual thresholds for perceiving movement are higher than the proprioceptive thresholds at slower velocities of the base of support movements in healthy individuals (Fitzpatrick & McCloskey, 1994). Perturbations with near-sensory amplitudes and lower frequencies may be difficult to perceive if only the visual system is used. Therefore using such perturbations to train individuals may force multi-sensory response characterized by increased utilization of somatosensory and vestibular afferents. However, the vestibular system is only known to be engaged at much greater postural disturbances and the visual system potentially possessing lower acuity at near-sway perturbations, the majority of the contributions towards perturbations with lower amplitudes and frequencies could be resulting from the proprioceptive afferents (Fitzpatrick & McCloskey, 1994; Richerson et al., 2006). Hence the choice of using small perturbation amplitudes with lower frequencies for both sensory acuity assessment as well as the intervention results in targeting the somatosensory system–the most utilized system for control of balance. As the majority of the balance impairments stem from somatosensory impairments, the near-sensory perturbation design becomes even more appropriate for individuals after a TBI (Allison, 1999).
Perturbation studies have shown that control of balance is not the result of reflexes, but a complex amalgamation of task and context-dependent strategies and rules learned and adopted by the central nervous system (Horak et al., 1997). Balance, like any other motor skill, can be learned and improved with continuous practice. Most of the perturbation-based intervention studies rely on this very insight into training patient populations with impaired mobility and balance. Our intervention uses sinusoidal perturbations to provide continuous, repetitive, cyclic training to proprioceptive inputs and neuromuscular efferents. The continuous sinusoidal perturbation-based approach may facilitate practicing and learning new balance strategies for CoM control in individuals with TBI, who may be biomechanically constrained (e.g., hemiplegia) and may not be able to apply standard bilateral strategies such as ankle and hip strategies to maintain balance (Horak et al., 1997). Repetitive perturbation training may also enable retraining of the neuromuscular system and reduction in response latencies, though such responses are not reported here and will be discussed in the future.
The study is limited by its small sample size and heterogeneity within the TBI group in terms of the severity of the injury. However, this study provides preliminary evidence on a novel intervention using a new metric that quantifies sensory acuity (PPT). The results of this pilot study support the investigation of the proposed intervention in a larger cohort. In future studies, a larger homogeneous sample of TBI needs to be assessed at multiple time-points to comprehensively understand the PPT as an outcome as well as the effect of the intervention. Further, as PPT relates to the detection of body-sway in a dynamic environment, the link between the PPT and falls as well as the efficacy of the PPT-based intervention to reduce falls, need to be investigated in the future. Future investigation will also include the changes in the response latencies post-intervention.
Conclusion
This investigation quantified impaired sensory acuity (in terms of PPT) in individuals with chronic TBI. At the completion of a novel near-sensory perturbation-based intervention, 4 out of 5 TBI-I gr-oup participants showed improvement in sensory acuity to 0.33 Hz, 0.5 Hz and 1 Hz perturbations to the base of support. These improvements were also accompanied by improved functional outcomes of static and dynamic balance and mobility. The results of this study provide preliminary evidence for a novel outcome (PPT) that quantifies sensory acuity to perturbations and its use in interventions aimed to improve mobility in individuals with TBI. The combined approach of sensory acuity assessment and its integration in perturbation-based intervention holds promise for improving perturbation detection abilities in individuals with TBI which could in-turn improve functional balance. The results of this pilot study support the investigation of this novel intervention in a larger cohort of individuals with TBI.
Conflict of interest
The authors have no conflict of interest to declare.
Footnotes
Acknowledgments
This study was supported by the New Jersey Commission on Brain Injury Research (NJCBIR) Multi-Investigator grant (CBIR15MIG004). The authors would also like to thank Dan Tanis, Will Weber and Oluwaseun Ibironke for their contributions to participant recruitment and data collection.