
Abstract
BACKGROUND:
Peripheral nerve injury can result in both sensory and motor deficits, and these impairments can last for a long period after nerve repair.
OBJECTIVE:
To systematically review the effects of sensory re-education (SR) on facilitating hand function recovery after peripheral nerve repair.
METHODS:
This systematic review was limited to articles published from 1970 to 20 December 2020. Electronic searching was performed in CINAHL, Embase, PubMed, Web of Science, and Medline databases to include trials investigating the effects of SR training on hand function recovery after peripheral nerve repair and included only those studies with controlled comparisons.
RESULTS:
Sixteen articles were included in final data synthesis. We found that only four studies could be rated as having good quality and noted obvious methodological limitations in the remaining studies. The current evidence showed that early SR with mirror visual feedback and the combinational use of classic SR and topical temporary anesthetic seemed to have long- and short-term effects, respectively on improving the sensibility and reducing the disabilities of the hand. The evidence to support the effects of conventional classical SR on improving hand functions was not strong.
CONCLUSIONS:
Further well-designed trials are needed to evaluate the effects of different SR techniques on hand function after nerve repair over short- and long-term periods.
Introduction
Peripheral nerve injury can result in both sensory and motor deficits, and these impairments can last for a long period after nerve repair (Oud, Beelen, Eijffinger & Nollet, 2007). Hands without sensibility are like eyes without vision, and this hinders the activities of daily living (Oud et al., 2007; Shieh, Chiu, Lee & Hsu, 1995). Therefore, it is of great importance to enhance the recovery of sensibility and to improve hand function in facilitating functional hand usage in daily life.
Although nerve repair reestablishes a mechanical structure for nerve regeneration, the sensibility is not always easily regained. Dellon (1997b) showed that peripheral nerve regenerates at a rate of one millimeter per day. Therefore, six to eight months are indispensable for the recovery of hand sensibility if the injury is at the wrist level. Nevertheless, a much longer time period than expected may be needed after some nerve injuries for the recovery of hand sensibility (Lundborg, Rosén, Dahlin, Holmberg & Rosén, 2004), which is probably due to the reorganized cortical representation after the injuries (Dellon, 1997a; Rosén, 1996). Within the first three weeks following peripheral nerve injury, the loss of sensory input can lead to substantial cortical reorganization in the primary somatosensory cortex such that the cortical territory of body areas with sensory loss can be taken over by the adjacent cortices (Dellon, 1997a; Lundborg, 2000). Conversely, although disrupted nerves can regenerate after repair, their axons may not grow in the same tube as previously, resulting in mismatched innervation in the skin. As a result, the corresponding hand area in the primary motor cortex cannot correctly understand the input signal from the injured body areas, leading to a phenomenon described as “the hand is speaking a new language to the brain” (Lundborg, 2010; Merzenich & Jenkins, 1993).
Sensory re-education (SR) was first described in the 1970s (Dellon, Curtis & Edgerton, 1971; Parry & Salter, 1976). It has been defined as an intervention to improve tactile gnosis by maintaining or restoring the territory of affected skin areas in the somatosensory cortex using cognitive learning techniques (e.g., visualization and verbalization), alternative senses (e.g., vision and hearing), or graded tactile stimuli (Dellon & Jabaley, 1982; Jerosch-Herold, 2011). It is a learning process to let the brain understand what language the hand is speaking (Lundborg & Rosén, 2001).
Dellon (1997a) showed that a 15-minute SR program effectively improved the sensibility in a patient who was still suffering from sensory dysfunction, although the injured nerve had been repaired many years ago. However, poor functional sensibility results are often got in the clinical practice. Traditionally, SR is introduced to patient when the hand is reinnervated, it may need several months. The late onset of SR training after nerve repair may be an explanation of this disappointing recovery. Therefore, timing of the onset of SR might influence effects of this training program. In recent years, with the increasing evidence that prove the plasticity of the brain, researchers also emphasized the important role of the rapidity of the possibility for functional reorganization on cortical and subcortical level (Rosén & Lundborg, 2004). Miller, Chester and Jerosch-Herold (2012) noted that SR can be divided into early and late phases. In the early phase, the hand does not have any sensibility, and this period may last for three or four months if the nerve injury is at the wrist level (Rosén, Balkenius & Lundborg, 2003). Training in this phase should focus on supplementary sensory stimuli, including visuo-tactile interaction and audio-tactile interaction (Jerosch-Herold, 2011). Once the hand is re-innervated, the late phase training, which is considered to be the “classical SR” following the principles of Dellon et al. (1971) and Parry and Salter (1976) should be started.
The first review related to SR was conducted by Oud et al. (2007), but it included only studies investigating the influencing factors of classical SR. The authors showed that evidence was insufficient to support the role of SR in improving functional sensibility. A subsequent review by Miller et al. (2012) focused only on SR training in patients with median or ulnar nerve injury, and their report focused only on the application of SR in the late phase but not in the early phase. In light of the important role of SR after nerve injury, we mainly reviewed the promotion of systematic evaluation of SR training on hand function recovery after peripheral nerve injury in this study. We reviewed the current studies assessing the effectiveness of the SR protocol, regardless of the patient’s stage of recovery.
Methods
The present study is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher, Liberati, Tetziaff & Douglas, 2009).
Search strategies
This systematic review was limited to articles published from 1970 to 23 December 2020. We performed an electronic search in CINAHL, Embase, PubMed, Web of Science, and Medline databases using the following keyword combinations: (sensory re-educati*) or (sensory reeducat*) or (sensory re-learn*) or (sensory relearn*) AND (peripheral nerve) or (median nerve) or (ulnar nerve) or (radial nerve) AND (nerve repair) or (nerve injur*) or (nerve surger*).
We included studies that met all of the following criteria: (1) randomized or quasi-randomized control trials (RCT or quasi-RCT); (2) adult patients after upper-limb peripheral nerve repair; (3) use of SR and sensory re-learning training programs as an intervention; and (4) published in English. We excluded studies that met any of the following criteria: (1) no clinical measurements related to hand function, (2) sample size less than 10, and (3) conference abstracts.
First, two reviewers independently selected all records based on titles and abstracts to exclude studies obviously irrelevant to our topic. Second, full texts of the remaining articles were reviewed for the eligibility criteria. Then, the two reviewers had a face-to-face discussion to reach an agreement on study inclusion, and any discrepancies were resolved by a third reviewer.
Assessment of methodological quality
Two reviewers independently assessed the methodological quality of the included studies using the Physiotherapy Evidence Database (PEDro) scale (Maher, Catherine, Herbert, Moseley & Mark, 2003). This scale contains 11 items and each item is judged by “yes” or “no” responses. The total number of “yes” responses for all items, except item one, is the final PEDro score, which ranged from 0 to 10 points. Studies with a final score lower than 4 points are described as having poor quality; 4–5 points as fair quality; 6–8 points as good quality; and 9–10 points as excellent quality. Another face-to-face discussion was carried out to achieve an agreement on quality assessment and any discrepancies were resolved by a third reviewer.
Data extraction and synthesis
Two reviewers independently conducted data ex-traction. A customized form was produced for data extraction regarding the general characteristics and results of the included studies. The extracted information consisted of authors, study design, characteristics of patients, experimental interventions (starting time, frequency and duration of training), outcome measures, and results. To perform a comprehensive qualitative synthesis, we considered both the consistency of results across included studies and the heterogeneity in methodological quality and sample size.
Results
Literature search and study characteristics
The flowchart of study selection is presented in Fig. 1. The initial search identified 241 records, from which 16 articles were finally included in the current review. Nine of these articles were RCTs (Cheng, 2000; Hassan-Zadeh, Lajevardi, Esfahani & Kamali, 2009; Lundborg, Bjorkman & Rosen, 2007; Paula et al., 2016; Rosén, Björkman & Lundborg, 2006; Rosen & Lundborg, 2007; Rosen et al., 2015; Saberi et al., 2018; Vikström, Rosén, Carlsson & Björkman, 2018) and seven were nonrandomized controlled trials (Antonopoulos et al., 2019; Imai, Tajima & Natsuma, 1989, 1991; Mavrogenis, Spyridonos, Antonopoulos, Soucacos & Papagelopoulos, 2009; Mendes et al., 2018; Priya, 2012; Shieh et al., 1995). In the included articles three pairs of articles by Imai et al. (1989, 1991), Lundborg et al. (2007) and Rosén et al. (2006), Rosen et al. (2015) and Vikström, Rosén, et al. (2018), respectively, were reported based on the same dataset of three trials. Considering that pairs of articles of each trial focused on different time effects or outcomes, we assessed all of these articles for quality. Characteristics of the 16 studies are presented in detail in Table 1. The individual sample size ranged from 13 to 52 and a total of 374 adults with median nerve injury, ulnar nerve injury, or both at the digital, wrist, distal forearm, or forearm level were included.
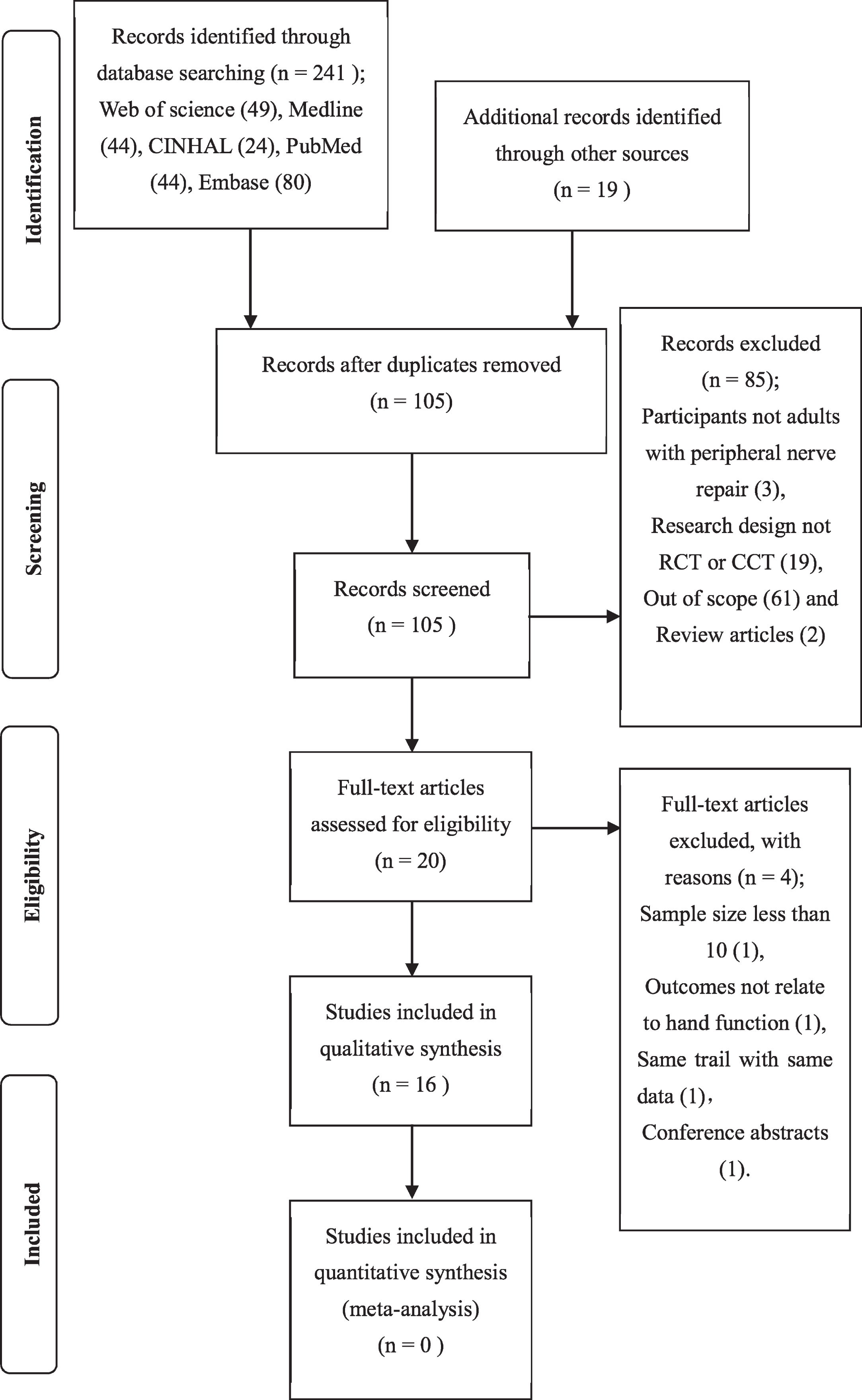
PRISMA flow diagram of studies through the review.
Summary of Study Characteristics
Abbreviations: SR = sensory re-education; min = minute; wk = week; d = day; yr = year; mon = month; SGS = sensor glove system; SWMT = Semmes-Weinstein Monofilament test; MVF = mirror visual feedback; MT = mirror therapy; ORT = object recognition test; MPT = Moberg’s pick-up test; TTT = touch threshold test; 2PD = two-point discrimination; STI = shape-texture identification; DASH = Disabilities of the Arm, Shoulder and Hand patient-reported questionnaire; NRS11 = numerical 11-point box scale; CISS = cold intolerance symptom severity.
The result of methodological quality assessment is presented in Table 2. The PEDro scores of all studies ranged from 2 to 6 points, indicating that four were good-quality studies (Lundborg et al., 2007; Rosén et al., 2006; Rosen et al., 2015; Vikström, Rosén, et al., 2018) and five were fair-quality studies (Hassan-Zadeh et al., 2009; Mendes et al., 2018; Paula et al., 2016; Rosen & Lundborg, 2007; Saberi et al., 2018). A poor-quality rating was given to the remaining seven studies (Antonopoulos et al., 2019; Cheng, 2000; Imai et al., 1989, 1991; Mavrogenis et al., 2009; Priya, 2012; Shieh et al., 1995).
Quality Review Table
Quality Review Table
Item 1: random allocation; Item 2: Concealed allocation; Item 3: Baseline comparability; Item 4: Blind participants; Item 5: Blind therapists; Item 6: Blind assessors; Item 7: Adequate follow-up; Item 8: Intention-to-treat analysis; Item 9: Between-group-statistical comparisons; Item 10: Point estimates and measures of variability.
Interventions used in the studies varied in modality and starting time and were divided into four categories.
Mirror visual feedback in the early SR phase
Four articles (Paula et al., 2016; Rosen et al., 2015; Saberi et al., 2018; Vikström, Rosén, et al., 2018) from three trials reported the effect of early SR training using mirror visual feedback (MVF). Two of these studies (Rosen et al., 2015; Vikström, Rosén, et al., 2018), which were based on the same trial, also used the observation of synchronous touch of both hands to perform MVF. Subjects of three studies (Paula et al., 2016; Rosen et al., 2015; Vikström, Rosén, et al., 2018) received MVF training immediately within the first week after nerve repair. During the MVF training, subjects were clearly asked to move both of their hands simultaneously. The remaining study (Saberi et al., 2018) started MVF training nearly one month after nerve repair (mean = 34.5 days, SD = 0.99 days), and subjects moved only the healthy hand, not both hands. In addition to simple hand movements in the MVF training, subjects also used their healthy hand to perform task-based activities in two studies (Paula et al., 2016; Saberi et al., 2018).
Three studies (Paula et al., 2016; Rosen et al., 2015; Vikström, Rosén, et al., 2018) assessed hand functions using a model instrument, which was known as the Rosen score (Rosén & Lundborg, 2003), and the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire at 3 months, 6 months, and 4–9 years after surgery. The Rosen score is made up of three subtests, and each test stands for sensory domain, motor domain and pain, and discomfort domain. A significant difference between groups was obtained only in one trial (Rosen et al., 2015; Vikström, Rosén, et al., 2018) in terms of shape-texture identification (STI) and two-point discrimination (2PD) at 6 months, and the change between 3 and 6 months. Even after a long-term follow-up, the intervention group still showed significantly better performance in sensory domain and had fewer self-reported problems than the control group. One study (Saberi et al., 2018) compared the changes in Semmes-Weinstein Monofilament test (SWMT), static 2PD, and stereognosis test between the two groups after 8 weeks of intervention. The changes in all measurements in the intervention group were significantly greater than those in the control group.
SGS in the early SR phase
Two studies (Mendes et al., 2018; Rosen & Lundborg, 2007) initiated the training of SGS within two weeks after surgery by using early SR training. The SGS consisted of gloves, amplifier, miniature microphone, and headphone. SGS allows the users to observe and hear sounds by touching objects having different textures with their fingers. Once voluntary mobilization was allowed, patients also used the SGS in their light daily activities (Rosen & Lundborg, 2007).
Mendes et al. (2018) focused on the between-group differences in the touch threshold test, 2PD, STI and DASH, which were administrated in the first, third, and sixth month after repair. No significant between-group differences were discovered in any measures at any time points. Another study (Rosen & Lundborg, 2007), however, compared the static 2PD and STI from the Rosen score for two groups at 3, 6, and 12 months and reported that the intervention group showed significantly better STI results than the control group at 12 months.
Classical SR
Seven articles (Antonopoulos et al., 2019; Cheng, 2000; Imai et al., 1989, 1991; Mavrogenis et al., 2009; Priya, 2012; Shieh et al., 1995) based on six trials used the classical SR program as the intervention. Although their interventions were not identical, the authors did follow the principles of classical SR. Four studies (Imai et al., 1989, 1991; Mavrogenis et al., 2009; Shieh et al., 1995) started the classical SR training when re-innervation was complete or when the patients could feel moving touch at their fingertips, that is, protective sensation was achieved. The remaining three studies (Antonopoulos et al., 2019; Cheng, 2000; Priya, 2012) had an exact time point. For example, Priya (2012) pointed out that the intervention commenced in the fourth week after nerve repair; and Antonopoulos et al. (2019) found that patients could feel the vibration of a 256 cps tuning fork at an average of 3.5 months (3–4 months) after the operation; while Cheng (2000) took safty as priority and started intervention at 3 weeks after surgery when participants were allowed to take off protective splint and actively move injuried fingers.
Two studies (Antonopoulos et al., 2019; Mavrogenis et al., 2009) reported outcomes after a long-term follow-up (1.5, 3, and 6 years) by using the locognosia test, 2PD (dynamic and static), and the Moberg pick-up test. Significant between-group differences were found only in the locognosia test at 1.5 and 3 years. Priya (2012) reported significant improvement in mean 2PD (static and dynamic), object recognition test, and level of paresthesia in the intervention group at 4 weeks. Experimental groups got significantly better SWMT and 2PD recovery than those in the control groups in studies by Cheng (2000) and Shieh et al. (1995). The difference is that Cheng (2000) assessed sensibility at 3 weeks and 6 months after surgery, while the follow-up time of the study by Shieh et al. (1995) varied in groups, that is, the mean time was 54.42 weeks (range 28–98 weeks) in the experimental group and 40.5 weeks (range 12–105 weeks) in the controls. Imai’s team reported different outcomes in two studies (Imai et al., 1989, 1991). SWMT, static and moving 2PD, object recognition test, and assessment of paresthesia were assessed at 1–2 years postoperatively in the intervention group and at 1–16 years (mean 6.6 years) in the control group. Results of the assessments, except for SWMT, were reported. After between-group comparison, significantly better recovery in SWMT, paresthesia, and object recognition test was achieved in the intervention group at 9 months, 12 months, and 2 years.
Classical SR and topical temporary anesthetic
Three studies (Hassan-Zadeh et al., 2009; Lundborg et al., 2007; Rosén et al., 2006) based on two trials combined classical SR and topical temporary anesthesia (EMLA® and Lidocaine-PTC, respectively) as interventions to evaluate whether topical temporary anesthesia could improve the effect of SR. In their interventions, subjects received local anesthesia on the palmar forearm, matched from the wrist level to proximal 15 cm, and then performed supervised classical SR training. One trial (Lundborg et al., 2007; Rosén et al., 2006) initiated intervention at a mean of 22 months (range, 11–52 months) after surgery, and the other trial (Hassan-Zadeh et al., 2009) commenced similar intervention at a mean of 20.9 months (range, 5–38 months) after surgery.
One of the trials (Lundborg et al., 2007; Rosén et al., 2006) reported short-term (1, 2, and 6 weeks) and long-term (8–11 months) outcomes of both groups using the Rosen score. For tactile gnosis (2PD and STI), significant between-group differences were obtained 1 and 6 weeks after the treatment, but they did not last for 8–11 months. Rosén et al. (2006) reported that significantly better results were obtained in the intervention group on SWMT, whole sensory domain, and total Rosen score after 6 weeks of treatment. Another trial (Mavrogenis et al., 2009) observed the mean values of SWMT and 2PD after 2 and 6 weeks of treatment, and a significant difference was observed between the two groups at both time points.
Discussion
This paper provided the latest evidence for the effects of SR on hand function after nerve repair of the upper extremity in adults. Compared with the previous two systematic reviews of SR, which were published between 2007 and 2012, this review included a larger number of RCT and quasi-RCT studies using different early SR programs. It is also the first review to investigate the effects of SR on hand function, not only limited to sensibility. Sixteen clinical studies with varied methodological quality were systematically reviewed. According to the sixteen included studies, SR might have an overall effect on improving the sensibility and reducing disabilities of the hand. Early SR with MVF appeared to have long-term effects on functional sensibility (tactile gnosis and perception of touch), dexterity, and self-reported problems of hand functions, which were consistently shown in two good-quality studies.
Underlying mechanism
Zink and Benjamin (2020) identified four types of cortical plastic changes that occur after upper extremity peripheral nerve injury, they are “Unmasking or removal of inhibitory controls in the affected region”, “Axonal sprouting and misdirection of regenerating peripheral nerves”, “Alteration of bilateral somatosensory and supplementary motor cortex maps”, “Invasion and expansion of adjacent cortical maps of affected nerve.” The therapeutic possibilities of SR were provided by this brain plasticity (Duffau, 2006; Rosén & Lundborg, 2004; Vikström, Carlsson, Rosén & Björkman, 2018). In SR, different techniques would be used in different phases to guide brain plasticity to support and enhance peripheral functions. In the early phase, cortical reorganization occurs in the somatosensory cortex after nerve transection immediately, and the region previously innervated by the injured nerve is occupied by territories of adjacent normal body parts (Lundborg, 2000; Rosén & Lundborg, 2004). In this phase, an early SR program uses alternative senses, such as vision or hearing, as a substitute for the loss of tactile stimuli to activate and maintain the hand map at the cortical area (Jerosch-Herold, 2011; Vikström, Carlsson, et al., 2018).
The mechanism underlying these substitutional stimuli is based on the hypothesis of cross-modal plasticity of the brain, which possibly creates an interaction between senses or sensory substitution (Bavelier & Neville, 2002; Mendes et al., 2013). According to the theory of long-term potentiation, applying consecutive pairings of cross-modal stimuli can strengthen the dendritic branching increments, which consequently increase the quantity of synaptic buttons and reduce neurotransmitter recapture and intracellular cascade facilitation. As a result, the relationship between nodes of a multi-scale network is promoted, and learning and adaptive behaviors are improved (Mendes et al., 2013).
In the studies reported by Mendes et al. (2018) and Lundborg et al. (2005) researchers used functional magnetic resonance imaging to investigate early cortical responses after a one-week early SR training with SGS. They found that an effective connection was established between the cortical hand map (Brodmann 3 area) and associative areas (auditory area), which proved that the use of SGS helped promote audio-tactile interaction and successfully built cross-modal plasticity.
It has been reported that MVF, which also is used in early SR, is a more effective method to induce higher activation in motor neurons (i.e., the “mirror neurons” in the sensorimotor cortex and supplementary motor area). The mirror neuron system plays a key role in motor action understanding and imitation by listening or reading action words and observing the MVF of action (Bai, Fong, Zhang & Hu, 2019; Svens & Rosén, 2009). Thus, researchers hypothesized that “sensory” observing or listening would active the somatosensory cortex, and they applied sensory MVF in early SR training (Svens & Rosén, 2009).
In the second phase, axons regenerate and the hand is re-innervated. Because of the misdirection of axonal growth, the cortical reorganization is unstructured (Rosén & Lundborg, 2004) and irreversible. The classical SR program, which inputs sensory stimuli to the injured nerve territory with visual feedback, memory, and learning, could be applied to help patients learn this “new language” spoken by the brain to adapt to the new synaptic organization. The cut-off time point between the two phases or the time point at which early and classical SR should be applied, however, is not specific. According to researchers who developed classical SR, SR training of the second phase commonly started once touch could be perceived by the hand (Dellon et al., 1971; Parry & Salter, 1976). In recent years, researchers suggested that the cut-off time was the time when some re-growing axons had reached the end of the hand (Rosen et al., 2015; Svens & Rosén, 2009). It is known that the sequence of sensory recovery is first the perception of pain and temperature that relates to unmyelinated and thinly myelinated fibers recovery, and then it is followed by the 30 Hz vibration, moving touch, static touch, and 256 Hz vibration that are related to large myelinated fibers recovery (Dellon, 1997c). Thus, a gap may exist between the time when axons re-grow to the hand and the time when touch is perceived by the hand. This nonidentical standard may explain why the starting time of interventions in the reviewed studies varied under these two principles. Nevertheless, by summarizing these studies, the cut-off time point may be identified between 3 to 4 months after nerve repair, if the injury is at the wrist level.
In summary, second phase (or classical) SR program and early phase SR with MVF were based on all four types of cortical plasticity mechanism that mentioned above. And early phase SR with SGS used cross-modal sensory substitution strategies related to the “Unmasking or removal of inhibitory controls in the affected region” mechanism. This was also proved by Zink & Benjamin (2020) in their current review.
Treatment influence factors
The treatment response to SR correlates with many factors, such as age, peripheral nerve status, and cognitive capacity (Miller et al., 2012; Rosén, Lundborg, Dahlin, Holmberg & Karlson, 1994; Vikström, Carlsson, et al., 2018). Previous studies have shown that 54% of the variance can be explained by the first two factors, whereas the specific cognitive capacities (verbal learning and visuo-spatial capacity) explained about 15% of the variation (Rosén et al., 1994). SR training program includes abstract components that is challenging to the cognitive capacities of trainers, especially, in early SR program. Generally, most trials included in this review had collected participants’ data on age and limited the criteria of eligibility in the peripheral nerve status, such as type of injury, timing of repair, and surgical technique. None of the trials, however, had considered or collected the data on the education level or cognitive capacities of patients who were included at baseline to determine whether the groups were equivalent.
A qualitative methodology study (Vikström, Carlsson, et al., 2018) was done to investigate the pers-pective of patients on early SR training, and three factors, explaining 45% of the variance, had been identified. Two of them, explaining 19% of the variance, were factors that descripted as “Do not get an illusion of touch easily and need support in their SR” or “Are not motivated, manage to get an illusion of touch but do not complete the sensory relearning”. This might cause some patients did not adhere to their long-term SR training.
As far as the methodological quality of included studies is concerned, the high attrition rate weakens the validity of findings. In 11 out of the 16 reviewed studies, more than 15% of participants did not undergo measurement of a key outcome at one of those time points when the outcomes were assessed. This finding meant that most of the trials could not obtain an adequate follow-up and some participants had dropped out of the studies. High drop-out rates decrease the statistical power, especially when there is a differential pattern of attrition between groups (Mahaniah & Rao, 2004). A significant difference between groups after treatment could be due to the bias related to attrition, not necessarily due to the effectiveness of treatment. A clear explanation of requirements to subjects and blinding of all subjects can minimize this attrition. Moreover, researchers should consider the drop-out rate when calculating the sample size. With such a drop-out rate, however, most of the reviewed studies did not clearly describe whether the subjects received treatment or control conditions as allocated, and also did not report about the use of intention to treat (ITT) analysis. The CONSORT statement (Schulz, Altman & David, 2011) recommends the use of ITT and flow charts to record in detail how subjects are included or excluded in each phase of the trial. Only Rosen et al. (2015) clearly pointed out that ITT was used in their research, and their participant follow-up chart was exhaustive.
Practice recommendation
The latest research by Zink and Benjamin (2020) highly recommended Classical SR in occupational therapy, and early SR with MVF or SGS were recommended for secondary or situationally use. However, all above recommendations are based on mechanism without considering the interventions’ efficacy. Our current study focus on effects of SR could be a supplement for this limitation. We find two RCTs with good quality reported the effects of early SR with using MVF (Rosen et al., 2015; Vikström, Rosén, et al., 2018). Therefore, applying early SR with MVF can be an effective intervention for people with sensibility dysfunction after peripheral nerve injury. Successful SR program should follow several principles, that is, 1) well-informed participant with activity and motivation, 2) and a long-term, repeated training sessions (Rosen et al., 2015; Vikström, Carlsson, et al., 2018). In detail, therapists or clinicians who conduct SR should make sure that patients are well educated with the concept of SR and fully understand it, so that, they are able to get an illusion of touch and complete the whole SR program (Vikström, Carlsson, et al., 2018).
One of the strengths of this review is that it focused not only on the evaluation of the effect of SR in functional sensibility but also on the whole related hand function. Therefore, we focused on the study of peripheral nerve injuries at upper extremity in adults. The outcome measurements of studies were not limited to sensibility and functional sensibility, and self-reported questionnaires of activities and participation also were applied. Another strength of this review is that the PEDro scale, which was used during the methodological quality assessment, was specially developed to identify an RCT or quasi-RCT if it seemed to be externally and internally valid and had sufficient statistical information to show the results. The limitation of this review is that various treatment techniques of SR made it difficult to perform a quantitative synthesis to investigate every SR technique.
Conclusions
The technique of SR varied in different trials. Overall, it seems that SR can enhance the recovery of hand functional sensibility and further reduce the patients’ subjective uncomfortable feeling and disabilities of the hand. However, the quality and quantity of studies to prove the effectiveness of each SR technique was limited. Further well-designed trials with blinding and adequate sample sizes are needed to evaluate the effectiveness of different SR techniques in hand function after nerve repair over short- and long-term periods. The test reported also should follow the principles of the CONSORT statement and describe the used SR technique in detail.
Footnotes
Acknowledgments
The authors would like to express their appreciation to Shengjie Xia for reviewing the contents of this review.
Conflict of interest
The authors declare no conflicts of interest with respect to the research, authorship, and publication of this article.