
Abstract
BACKGROUND:
Traumatic Brain Injury (TBI) is characterized by a highly heterogenous profile in terms of pathophysiology, clinical presentation and outcome.
OBJECTIVE:
This is the first population study investigating the epidemiology and outcomes of moderate-to-severe TBI in Cyprus. Patients treated in the Intensive Care Unit (ICU) of Nicosia General Hospital, the only Level 1 Trauma Centre in the country, were recruited between January 2013 and December 2016.
METHODS:
This was an observational cohort study, using longitudinal methods and six-month follow-up. Patients (N = 203) diagnosed with TBI were classified by the Glasgow Coma Scale at the Emergency Department as moderate or severe.
RESULTS:
Compared to international multicentre studies, the current cohort demonstrates a different case mix that includes older age, more motor vehicle collisions and lower mortality rates. There was a significantly higher proportion of injured males. Females were significantly older than males. There were no sex differences in the type, severity or place of injury. Sex did not yield differences in mortality or outcomes or on injury indices predicting outcomes. In contrast, older age was a predictor of higher mortality rates and worse outcomes.
CONCLUSION:
Trends as described in the study emphasize the importance of continuous evaluation of TBI epidemiology and outcome in different countries.
List of abbreviations
Emergency Department Glasgow Coma Scale Glasgow Outcome Scale Extended Intensive Care Unit Motor Vehicle Collision Nicosia General Hospital Quality of Life Quality of Life after Brain Injury Simplified Acute Physiology Score II Sequential Organ Failure Assessment Score Traumatic Brain Injury
Introduction
Traumatic Brain Injury (TBI) is considered as one of the most complex and chronic conditions due to its highly heterogenous profile in terms of pathophysiology, clinical presentation and outcome. Considering current reports of changes in the demographics of TBI, along with differences in acute medical treatment and variability in rehabilitation practices around the world (Andriessen et al., 2011), the current study aims to specify the unique characteristics of the TBI survivor in the context of Cyprus and join global efforts in understanding the epidemiology, trends and outcomes of TBI.
TBI mortality rates range between less than 1% in mild TBI to 40% in severe TBI (Murray et al., 1999; Smits et al., 2007). However, even with the implementation and adherence to international guidelines advocating a structured and systematic approach to acute TBI management, mortality rates have not declined (Stein et al., 2010). Furthermore, increased life expectancy in the general population is reflected in increased prevalence of older patients with TBI (Maaset al., 2008). Older age is accompanied by a specific pattern of injuries, i.e. falls and vehicle-pedestrian injuries. Changes in demographics could partly explain the stagnating mortality rates since older age is related to worse outcomes (Hukkelhoven et al., 2003).
Studying TBI in Cyprus offers distinctive opportunities since the country presents unique socio-cultural characteristics, i.e. low divorce rates, strong family involvement, and a relatively genetically homogenous population due to its island-nation character (Mediterranean island country with a small population); for example, the frequency of the APOE4 allele, which has been implicated in poor recovery post-TBI, is among the lowest around the world (Cariolou et al., 1995). Additionally, since TBI from motor vehicle collisions (MVCs) results in greater severity than do all other aetiologies combined (Munivenkatappa et al., 2016) and since Cyprus has a high number of MVCs compared to other EU countries (European Commission, September 2017), it is expected to have a higher rate of severe TBI than other EU countries. Finally, Cyprus boasts one of the highest life expectancies in Europe with 80.5 and 84.9 for males and females respectively (Raleigh, 2019). Hence, the demographic distribution of the Cypriot population and outcomes may be different compared to other nations.
The present study will also contribute to the growing body of studies investigating sex issues in TBI outcome. The complex and dynamic relationship between biology, education, income, health practices, and environment may affect injury outcome differentially in males and females at the acute and chronic phase post-injury (Mollayeva & Colantonio, 2017). Despite the potential implications in TBI prevention and rehabilitation efforts, sex and gender research is a relatively new area of research and only a small percentage of the published literature in TBI has addressed this issue (Spani et al., 2018).
The current state of the art in sex and gender differences in TBI severity and outcome is both limited and inconclusive. Specifically, the severity of injury, as measured by the Glasgow Coma Scale (GCS), was found to be significantly different between females and males (Munivenkatappa et al., 2016), but these differences were in part due to the different causes of injury. Furthermore, among studies of moderate-to-severe TBI, 34% found that females fared worse than males and 46% of the studies showed that females fared better (Gupte et al., 2019).
Some studies describe superior overall responses to rehabilitation therapy in females (Brown et al., 2012; Grosswasser et al., 1998) and better hospitalization outcome than males in terms of mortality (Tobi et al., 2016), whereas other studies describe poorer outcome in females on primarily subjective outcome measures (Farace & Alves, 2000) and higher mortality in females (Klauber et al., 1981; Kraus & Nourjah, 1998; Munivenkatappa et al., 2016). Factors involved in possible gender-related differences in outcome are in part socially motivated (adequate representation, equal rights and equal access to rehabilitation) and in part biological (i.e. anatomical dimorphism and hormonal influences). Recognizing the importance of sex/gender is key in determining whether it has a significant effect on TBI.
The international incidence of TBI (of any severity) is reported to be 349 (95% CI 96 –1266) per 100,000 person-years. When these results are stratified by sex, the pooled annual incidence of TBI among females is 195 (95% CI 84–452) per 100,000 person-years, compared with 388 (95% CI 138–1092) per 100,000 person-year among males (Mollayeva et al., 2018). The ratio of injured males:females changes across the lifespan. There is a high male:female ratio during adolescence and young adulthood attributed to MVCs that can reach up to 4.5:1 (Munivenkatappa et al., 2016). By contrast, there is approximate unity or inversion of the sex ratios in mid-life and older adulthood (i.e. age 45 to 75). In older patients (above 65 years) no sex differences have been observed in the rate of TBI, while after the age of 75 years, there is a slightly higher incidence of mild TBI in females, mostly due to falls (Pentland et al., 1986). Thus, it is important noting that although males may sustain a greater number of TBIs than females, females still comprise a substantial portion of TBI patients.
The present study is the first national population study on the epidemiology of TBI treated in the ICU over a four-year period. Demographic variables, injury etiology, acute management, acute outcome and six-month follow-up data are analysed in this observational study. According to international statistics provided by the US Centres for Disease Control, about 2% of the general population live with TBI related disabilities, which amounts for about 17,500 survivors in Cyprus (estimated population of 875,900, controlled by the Republic of Cyprus; Ministry of Finance, 2018). Only a small percentage of individuals with severe TBI (less than 30%) receive acute rehabilitation per year at the Melathron Agoniston EOKA, which is the only acute comprehensive rehabilitation centre in Cyprus. The fragmented health care system, with limited access to inpatient rehabilitation and no post-acute comprehensive rehabilitation services for TBI survivors, provides unique opportunity to study the true effects of TBI.
Methods
Design
This was an observational, national cohort study with a six-month follow-up.
Study site
The study took place at Nicosia General Hospital (NGH) in Cyprus, the national Level 1 Trauma Centre, a multidisciplinary ICU with 17 beds. The cohort study included patients admitted in the ICU from the period of January 2013 until December 2016, whereas the six-month follow-up phase involved patients admitted in the ICU from March 2015. This level 1 Trauma Centre serves the needs of the population under the control of the Republic of Cyprus (i.e. excluding the population of the occupied area of Cyprus).
Participants
All adult patients with moderate-to-severe TBI admitted in the ICU during the target period were included in the study. Mild cases admitted in the ICU were excluded as a potential source of bias, since mild TBI cases were usually admitted due to severe injuries to other parts of the body than the head and their numbers in the ICU were not representative of the mild TBI cases on a national level. Exclusion criteria also involved hospital admission over 24 hours after injury. Regarding the six-month follow-up, only survivors who were Greek or English speakers were assessed.
Method
Data obtained from this study were retrieved from the Prosafe electronic database funded by the European project CREACTIVE (FP7-HEALTH-2013-INNOVATION-1). Patients included in the study were assessed in the Emergency Department (ED) and on admission to the ICU. Their clinical data were collected from medical records by trained nurse staff supervised by a physician and were entered in the Prosafe database. Injury severity was classified based on the GCS score at admission to the ED, defined as moderate (CGS 9–12) or severe (GCS 3–8). When the patient was intubated, the GCS score obtained before intubation was used as a qualifier to determine eligibility for study inclusion.
Regarding the outcome assessment, in-hospital mortality and discharge location were collected from the the Prosafe database. The six-month follow-up outcome was assessed through a telephone interview using: Glasgow Outcome Scale Extended (GOSE), a global scale for functional outcome that rates patient status into one of five categories: 1 = Death (D), 2 = Vegetative State (VS), 3 = Lower Severe Disability (SD–), 4 = Upper Severe Disability (SD+), 5 = Lower Moderate Disability (MD–), 6 = Upper Moderate Disability (MD+), 7 = Lower Good Recovery (GR–), and 8 = Upper Good Recovery (GR+). GOSE was administered through a structured interview to either the survivor directly or to the primary caregiver; Quality of Life after Brain Injury Overall Scale (QOLIBRI-OS), a brief instrument (six items) specifically developed to assess health-related Quality of Life (QoL) after TBI. The questionnaire covers the following dimensions: 1. Cognition, 2. Self, 3. Daily life and Autonomy, 4. Social Relationships, 5. Emotions, and 6. Physical Problems. The scores are reported on 0 –100 scale, where 0 = worst possible QoL and 100 = best possible QoL. QOLIBRI-OS was only used when direct contact with the survivor was feasible and was administered through a structured interview.
Data were analysed using SPSS 25. Mostly descriptive data are presented. The primary data analysis was Pearson χ2 test. The level of significance was set at α= 0.05. Logistic regression was conducted to assess the odds ratio on the risk of death following TBI hospitalization, after adjustments for age and sex.
Results
Acute phase
The cohort included 203 patients (80% male) with M age = 43.90 (SD = 21.11) years and 20% female with M age = 53.18 (SD = 22.44). On average, males had a lower mean age of almost 10 years as compared to females (t(201) = –2.46, p < 0.05 with small effect size, 0.17). The difference between the frequency of TBI occurrence between sex was significant (χ2(1) = 74.53, p < 0.001). Overall 79% of the injuries were severe and 21% were moderate TBIs, with no significant association between the frequency of severity and sex (χ2(1) = 0.38, p > 0.05). Patient and injury characteristics are presented in Table 1. MVCs were the most common cause of injury and thus the most common location of injury was a public place. There was no significant association between the location of injury and sex (χ2(3) = 5.35, p > 0.05) or between the injury mechanism and sex (χ2(10) = 12.45, p > 0.05). There was no significant difference (t(51.47) = –1.41, p > 0.05) in the average age of patients involved in MVCs, M = 44.29 (SD = 22.93), as compared to falls, M = 50.17 (SD = 19.63).
Demographic characteristics and causation
Demographic characteristics and causation
Note. Values are reported as n (%) or mean (sd).
Regarding the type of trauma, over 75% of the injuries were closed head injuries with the most common type of intracranial injury being subdural hematoma for males and subarachnoid haemorrhage for females (Table 2), even though no significant sex associations were detected (χ2(4) = 4.07, p > 0.05; χ2(111) = 120.16, p > 0.05). Both Sequential Organ Failure Assessment (SOFA) and Simplified Acute Physiology Score (SAPS II) revealed similar scores for males (M = 9.10 and M = 47.44) and females (M = 9.58 and M = 51.92), t(195) = –0.82, p > 0.05; t(195) = –1.55, p > 0.05, which means that the ICU scoring systems for predicting mortality showed similar prognostic patterns for sex.
Injury severity parameters
Note. Values are reported as n (%) or median (interquartile range) or mean (sd).
Of the patients admitted to the ICU, 98% required mechanical ventilation (Table 3) and this association was significant to the severity of TBI, χ2 (1) = 7.23, p < 0.05. Based on the odds ratio, the odds of having invasive ventilation was 0.08 times higher if the severity of brain injury was severe than if it was moderate. However, sedation which was reaching up to 91% had no significant association with the severity of TBI (χ2 (1) = 3.90, p = 0.05). Raised ICP (>20 mm Hg) was observed in 37% of males and 27% of females. An ICP monitoring device was placed in 76% of males and 67% of females (χ2(1) = 1.35, p > 0.05) and Mannitol was administered in 35% of male ICU-admitted patients and in 14% of female (χ2(1) = 3.95, p = 0.05). Hypertonic saline was administered in 31% of males and 14% of females (χ2(1) = 2.76, p > 0.05). Therapeutic hypothermia (n = 31) and barbiturates (n = 17) were rarely used.
Interventions at intensive care
Note. Values are reported as n (%) or mean (sd).
Through an analysis of logistic regression (forward LR method) on the observed outcome (Fig. 1), age was found to be a significant predictor of mortality for both ICU and Hospital outcome (Tables 4 and 5). However, adding sex in the model and/or their interaction term did not lead to more accurate classification. More specifically, patients who deceased in the ICU had a mean age of 52.91 (SD = 23.43) whereas patients who discharged alive from the ICU had a mean age of 44.23 (SD = 21.14). Patients who deceased post-ICU discharge and were hospitalized in another ward had a mean age of 65.14 (SD = 15.46), whereas patients who discharged alive from the hospital had a mean age of 42.31 (SD = 20.58).
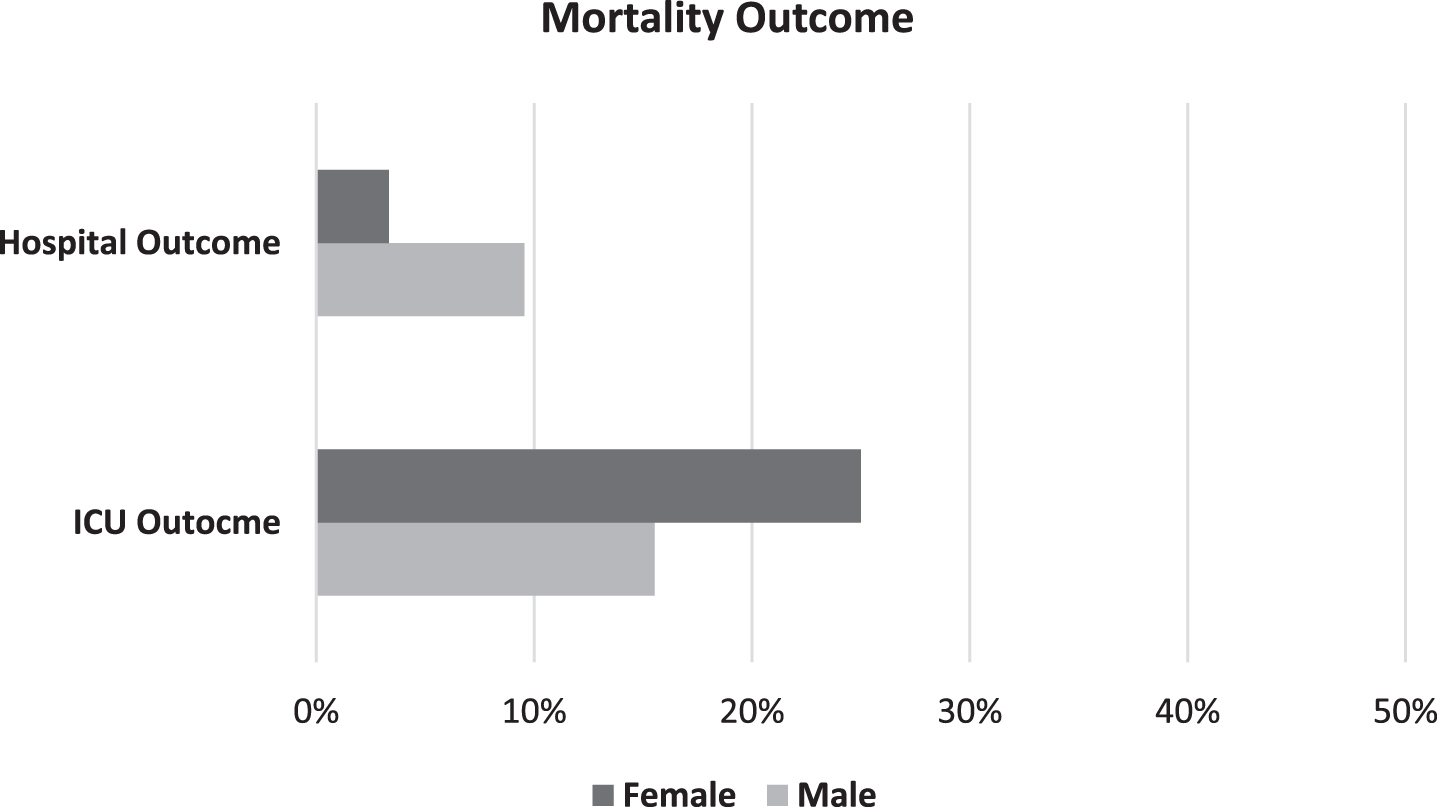
Mortality outcome by sex.
Coefficients of the model predicting whether a patient will decease in the ICU
Note. R2 = .02 (Hosmer & Lemeshow) .02 (Cox & Snell) .04 (Nagelkerke). Model χ2(1) = 4.59, p < .05. *p < .05, **p < .001.
The highest percentage for all moderate and severe patients was discharged to their home six months post-injury (Table 6). QOLIBRI-OS revealed only minor satisfaction and was especially low for patients with moderate TBI as compared to patients with severe TBI. Although this phenomenon is discussed below, data are severely limited for conclusive analysis.
Figure 2 presents the six-month outcome (March 2015 –December 2016) for patients after their injury (N = 28), using GOSE scoring. Mortality was only present in 10% of the moderate injuries. 50% of the patients with moderate TBI had an USD, whereas 44.45% of the patients with severe TBI had a LSD. Furthermore, as shown in Fig. 3, there is a negative association between age and GOSE outcomes. However, due to the limited number of TBI survivors in the follow-up arm of the study, results should be interpreted with caution.

Cumulative percentages of six-month outcome in patients using GOSE. *VS: Vegetative State; LSD/USD: Lower/Upper Severe Disability; LMD/UMD: Lower/Upper Moderate Disability; LGR/UGR: Lower/Upper Good Recovery.
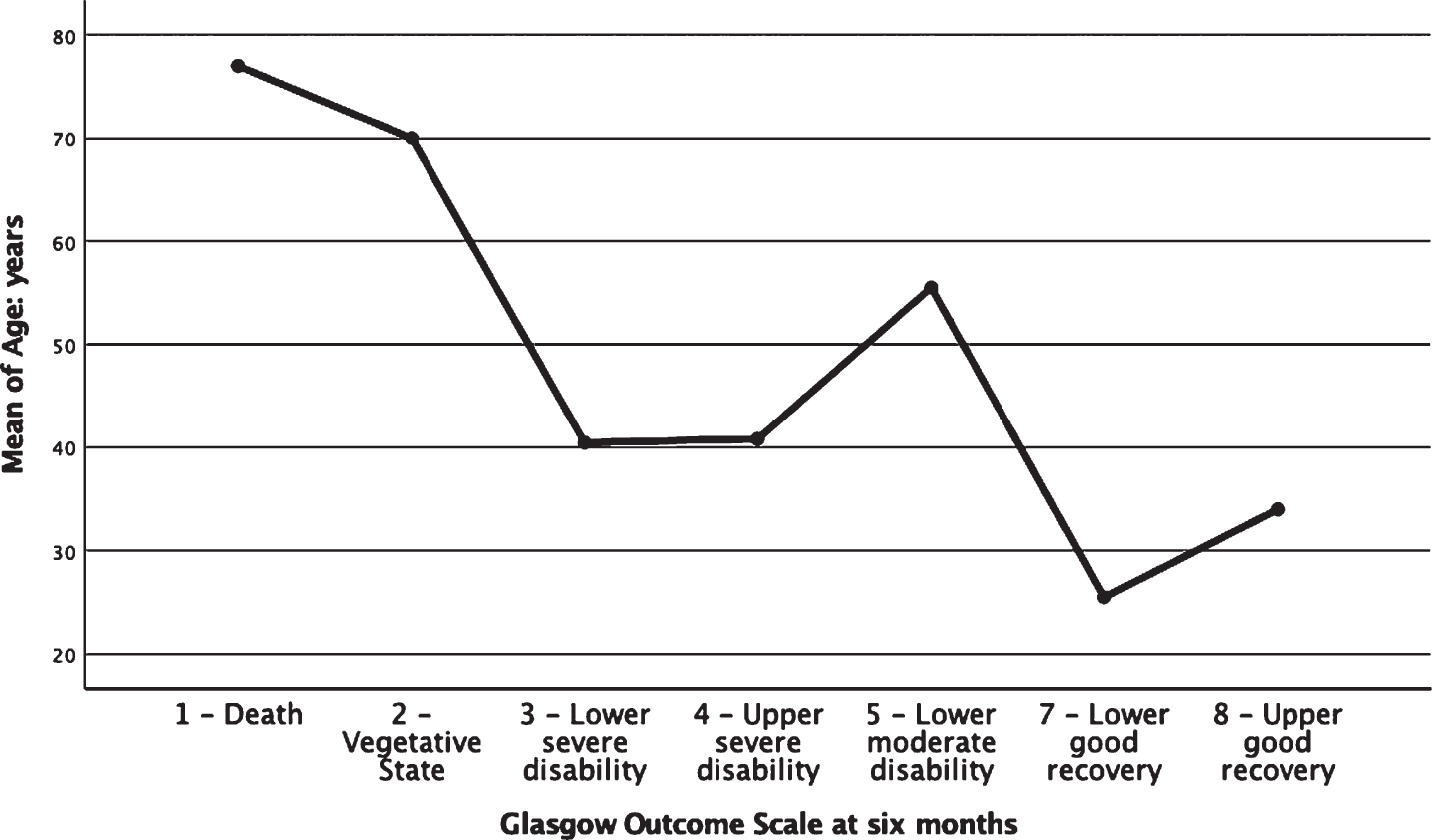
Graph representing GOSE scoring and age in six-month outcome.
The present study is the first national population study on the epidemiology of moderate-to-severe TBI treated in the ICU over a four-year period. Availability of TBI demographic and acute clinical data in addition to outcome measures, offer the opportunity of exploring epidemiological and sex profiles in this island country with its unique sociocultural characteristics.
According to the current study, about 3.88 cases per 100,000 people were estimated to sustain severe TBI every year in Cyprus. The numbers regarding moderate TBIs are not considered all-inclusive since patients with uncomplicated TBI may be admitted in other hospitals. Mean age in the current TBI cohort (M = 45.72, SD = 21.64) is among the highest of all previously reported studies in other countries, which is in line with the reported trend of increasing age in TBI (Maas et al., 2017). More specifically, in studies of all ages, all TBI severities and all injury-mechanisms, the lowest reported mean age was 26.7 in the Republic of San Marino (Servadei et al., 1985); the highest was 44.5 in Austria (Mauritz et al., 2014). As a result of population aging, it has been suggested that falls emerge increasingly frequently as a cause of injury regardless of race and sex (Kraus et al., 1984), while in adolescence and young adulthood, males and ethnic minorities are at increased risk of TBI due to violence and MVCs (Bruns & Hauser, 2003). The mechanism of injury in developed countries is strongly associated with the patients’ demographics. In the current study, MVCs still rank first with falls constituting the second most common cause of TBI. However, as mentioned earlier, this was an expected finding since MVCs are quite high in Cyprus (European Commission, September 2017). It is furthermore noted that Cyprus is generally a safe country and violent crimes are low compared to EU countries of similar size (Advisory, U.S. Department of State Travel, 2019), something that was also reflected in the TBI epidemiological results regarding the mechanism of brain injury. Hospital length of stay seems to follow the trend of other studies (Tobi et al., 2016).
Regarding the management of patients who sustained severe TBI, neurosurgery was performed in 74% of patients which is quite high compared to 37–67% in previous studies (Myburgh et al., 2008). Sedation is becoming more common (Stocchetti et al., 2004) and ICP monitoring was also quite high in the current study (74%) compared to others (43–57%; (Mauritz et al., 2008). These procedures are also related back to the high frequency of neurosurgical procedures performed. These findings suggest that the ICU in Cyprus adopts aggressive measures in dealing with TBI as compared to other countries. This attitude could be partly attributed to the strong family support that characterizes the Cypriot culture, which in turn leads practitioners in taking aggressive life-saving measures.
The frequency of use of brain-specific therapies in our cohort was similar to recent studies (Mauritz et al., 2014). For example, in our study brief hyperventilation was used in 7.6% (vs. 6.1–64%) and barbiturates were administered in 14.4% (vs. 8.7–39%). Despite implementation of structured protocols, differences in opinions continue to add in the variety in “treatment aggressiveness” that is being observed in various stages of TBI medical management across studies.
Compared to earlier observational TBI studies, our cohort revealed relatively low mortality rates in ICU and hospital discharge (Andriessen et al., 2011), which could be related back to the aggressive treatment of the ICU. Age was found to be a predictor of mortality, in both ICU and Hospital outcome, whereas sex was not. Age as a predictor was a quite expected result since age-related co-morbidities reduce physiological reserve and increase the incidence and severity of brain damage due to second injury mechanisms. Furthermore, treatment used for co-morbidities may predispose the patient to an increased risk for haemorrhage or may worsen the evolution of intra-cerebral traumatic lesions, thus interfering with brain reserve mechanisms and with the potential for plasticity and neural repairs. Additionally, the perception of a universally poor prognosis in older age may lead to therapeutic nihilism and decisions of less aggressive treatment that consequently fuels a self-fulfilling prophecy of poor outcome and reinforces prejudices (Stocchetti et al., 2017).
In terms of sex, the incidence of TBI in females (19.7%) treated in the ICU of Cyprus was significantly lower than males (80.3%). The reported proportion of males with TBI in other international studies was always greater than that of females (irrespective of age, severity and mechanism of injury), ranging from 55% in Sweden in 2001 to 80% in Ireland in 2005 - 2007 (Frohlich et al., 2011; Styrke et al., 2007). In our cohort, females were significantly older (M = 53.18) than males (M = 43.90), which is also evident in the existing data of other countries (Kraus et al., 2000). Similar case fatality rates were found between males (24.22%) and females (27.50%). US data indicate higher mortality in females compared to males (Kraus et al., 2000) and other studies show higher rate of males’ case fatality rate (Klauber et al., 1981), although in certain age groups the fatality rate was significantly elevated in females. More specifically a surveillance study (Coronado et al., 2011) demonstrated that each year of the reporting period, TBI mortality rates among males were higher than those among females, especially among the age of 20–24 years. In this age group, males had rates at least four times higher than those for females.
At six-month follow-up, 10% of the moderate TBI patients had died but none of the severe TBI patients. In previous observational studies, six-month mortality ranged between 16% and 19% in moderate TBI (Compagnone et al., 2009; Murray et al., 1999) and between 32% and 49% in severe TBI (Myburgh et al., 2008; Rusnak et al., 2007). In surviving patients, GOSE findings revealed that most severe TBI cases had a LSD whereas most moderate TBI cases had an USD. Most TBI survivors, six months post-injury, were placed at their home whereas 41.18% of severe TBI survivors were still in the inpatient rehabilitation centre. QOLIBRI-OS ratings were quite low especially in moderate patients (28.13%) even though they had a better GOSE score overall. Although data collected at follow-up phase were severely limited for conclusive analysis, it is worth noting this difference. The phenomenon of diminished self-awareness associated with injury severity has been observed cross-culturally (Arnould et al., 2016; Kelley et al., 2014; Pettemeridou et al., 2020), suggesting that the problem is related to neurologic impairments of perception and secondary psychological coping mechanisms.
Coefficients of the model predicting whether a patient will decease in the hospital
Coefficients of the model predicting whether a patient will decease in the hospital
Note. R2 = .16 (Hosmer & Lemeshow) .09 (Cox & Snell) .20 (Nagelkerke). Model χ2(1) = 15.60, p < .001. *p < .05, **p < .001.
Six-month follow-up (2015 – 2016)
*Values reported as n (%).
The establishment of the electronic data records in the ICU at NGH in 2011 provided the first opportunity to investigate the epidemiology of TBI in the ICU context. Some study limitations need to be addressed. Similar to other projects, this study also suffered from missing data in all pre-hospital, some hospital and some six-month follow-up data (Myburgh et al., 2008). Loss to follow-up was explained in part by the fact that some patients who were non-Cypriot residents had returned to their home country prior to the six-month follow-up. Another source of loss to follow-up was the absence of contact information.
We also acknowledge that variability among studies on injury indices and patient outcomes may be due to methodological differences. For example, the classification of TBI severity varied considerably in different multicenter observational studies (Myburgh et al., 2008; Rusnak et al., 2007). Moreover, the accuracy of the GCS as an instrument to grade injury severity has been challenged. A growing use of sedatives and neuromuscular blocking agents in the pre-hospital setting results in more patients with artificially low GCS scores at hospital admission (Stocchetti et al., 2004) and weakens the predictive value of the GCS score. Consequently, much effort is currently directed toward standardization of data collection across studies i.e. common data elements (CDE).
Despite the significant health, social and economic burden, services in Cyprus for survivors of TBI exhibit serious problems due to fragmentation with significant disparities in access, and lacking a coordinated and comprehensive interdisciplinary approach to management. For example, inpatient rehabilitation is not part of the standard of care; a large number of patients, 70% in the present study, do not receive systematic inpatient comprehensive rehabilitation during the early phases of recovery when the brain reorganizes spontaneously after injury. It has been demonstrated that this lack of organized rehabilitation results in brain atrophy and decreased structural and functional connectivity associated with chronic neurocognitive deficits (Konstantinou et al., 2016; Konstantinou et al., 2019; Yiannakaras et al., 2019). Whereas those who receive treatment demonstrate significant gains in neurocognitive performance and functional outcomes (Cicerone et al., 2019; Constantinidou, 2019). Also, no epidemiological studies have been conducted for hospitalized patients prior to this study, and there are no surveillance systems in order to obtain reliable information on the impact, prevalence, incidence and disease progression that will guide policy and services. Lack of longitudinal and large cohort data makes it challenging to promote and implement evidence-based clinical and public health interventions to reduce the incidence and burden of injury. As these problems suggest, radical changes in the management of brain injury are required.
Our study on the epidemiology of moderate-to-severe TBI demonstrates a different case mix from earlier series (older age, more MVCs etc.) and lower mortality rates. The epidemiological pattern emphasizes the need for implementation of prevention policy targeting especially road safety, with a focus on MVCs i.e. better road safety and improved transportation system, stricter road security laws against drunk driving, speeding, and cessation of driving as well as mandatory use of prevention tools such as airbags, helmets and car seatbelts. Combining information from more than one time point and documentation of additional factors of classification may advance injury severity diagnosis and outcome prediction as well as impact the health economics in TBI. Improvements in completeness and quality of epidemiological data in TBI is deemed necessary and there is a need for adopting an international consensus in standardizing epidemiological monitoring of TBI. Once again, Cyprus offers the opportunity to study TBI in a relatively homogeneous group thus contributing to international efforts to improve acute management and improve outcomes for patients with TBI.
Conflict of interest
The study was funded by the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement no. 602714 (CREACTIVE) and in part by the Republic of Cyprus and the European Regional Development Fund under the Framework Programme “RESTART 2016-2020/EXCELLENCE HUBS: PILLAR II” for Research, Technological Development and Innovation (EXCELLENCE/1216/0411). .
Footnotes
Acknowledgments
The authors would like to thank the team of the Brain Injury Neurorehabilitation Project (BRAIN REHAB) and the CREACTIVE Study Country coordinators and members of the Steering Committee: Luca Antiga, Guido Bertolini (Coordinator), Akos Csomos, Or Duek, Primoz Gradisek, Rafael Kaps, Vera Knyazer, Isaac Lazar, Roberto Latini, Malgorzata Mikaszewska-Sokolewicz, Giulia Paci, Nektaria Xirouchaki. They would also like to express their gratitude to all study patients and their families.