
Abstract
BACKGROUND:
Aquatic exercises are among the treatments available to improve the quality of life after stroke.
OBJECTIVES:
To investigate changes in the quality of life after 8-week of aquatic exercises in post-stroke individuals.
METHODS:
A case series study was designed, including four male participants. Exclusive aquatic exercise was performed for 8-week, 50 minutes per session, 2×/week. Their quality of life was evaluated before and after the intervention using the Stroke Impact Scale (SIS).
RESULTS:
Participant 1 improved in the mobility domain, achieving a Clinically Important Difference (CID). Participant 2 improved in the strength and mobility domain, achieving CID; his stroke recovery was 6%, and it reached 50% post-intervention. Participant 3 improved in the mobility domain, achieving a CID and a Minimal Detectable Change (MDC); his stroke recovery increased from 45 to 60% post-intervention. Participant 4 improved the strength, mobility, and activities of daily living domains, achieving a CID and a MDC, but his stroke recovery remained unchanged at 80%.
CONCLUSIONS:
All participants achieved a CID in the mobility domain; thus, the aquatic exercise intervention was considered meaningful. Moreover, the SIS is able to evaluate aspects of the recovery process regarding health-related quality of life after stroke, as demonstrated by the results of the overall recovery after aquatic exercises.
Introduction
Stroke is the third leading cause of death in low- and middle-income countries and has a high socioeconomic impact. It is also the second leading cause of disability worldwide Dee, Lennon & O’Sulivan,al., 2020; Giuriati, Servadio, Temperoni, Curcio, Valente & Galeoto, 2020). This scenario is expected to continue until 2030 (Avan et al., 2019). Seventy percent of strokes and 87% of both stroke-related deaths and disability-adjusted life years occur in low- and middle-income countries (Feigin et al., 2014; Feigin et al., 2009; Strong, Mathers & Bonita, 2007). Furthermore, the stroke incidence in low and middle-income countries has doubled over the last four decades (Feigin et al., 2014), and strokes in those countries occur on average 15 years earlier in people living in low and middle-income countries relative to high-income countries, besides causing more deaths (Owolabi et al., 2015). Individuals of productive working ages are the most affected by stroke. Normally, post-stroke is related to impaired motor function, difficulty in walking, low physical fitness, and a reduced quality of life (Johnson, Onuma, Owolabi & Sachdev, 2016; Saquetto et al., 2019).
Among the available interventions for improving disability after stroke, one is aquatic exercises. These exercises, such as general body movements and walking in water, might be beneficial due to the buoyancy that eases the performance of body movements by providing body weight support, increasing postural balance, and encouraging passive strengthening of weakened muscles (Chae, Jun, Im, Jang & Park Heywood, 2020). However, one of the first systematic reviews on aquatic exercise interventions intended to improve activities of daily living (ADL) after stroke included four trials totaling 94 participants. The authors of the review concluded that there is no evidence that these exercises might help reduce disability after stroke (Mehrholz, Kugler & Pohlet, 2011).
Several outcome measures are available to assess the physical impact of stroke; however, their problems are multidimensional (Mulder & Nijland, 2016). For example, physical function outcome measures are generally the focus in stroke rehabilitation programs (Schepers, Ketelaar, Van de Port, Visser-Meily & Lindeman, 2007), while patient-reported rating scales are becoming more commonly used to measure several aspects of patient health associated with therapeutic interventions (Carod-Artal, Coral, Trizotto & Moreira, 2008).
The Stroke Impact Scale (SIS) is a disease-specific, self-report questionnaire used to assess disability and health status after stroke, developed to incorporate all aspects of stroke that may influence health-related quality of life (Duncan, Bode, Lai & Perera, 2003; Duncan, Wallace, Lai, Johnson, Embretson & Laster, 1999). Assessment of quality of life in these patients is recommended to evaluate their neurological functioning, as simple disability assessment is insufficient to establish the overall influence of stroke on patient well-being (Suenkeler et al., 2002). Quality of life is a relevant index of outcome after stroke and is likely to be more relevant to the patient than impairment or disability (Sturm, Osborne, Dewey, Donnan, Macdonell &Thrift, 2002; Buck, Jacoby, Massey & Ford, 2000). The SIS also demonstrates adequate to excellent test-retest reliability in all domains (Edwards & O’Connell, 2003), excellent interrater reliability for hand function and mobility, and excellent internal consistency (Carod-Artal, Coral, Trizotto & Moreira, 2009).
Lin et al., (2010) performed a study to establish the minimal detectable change (MDC) and clinically important differences (CID) of the physical domains of the SIS and to assess the proportions of patients’ change scores exceeding the MDC and CID cut-offs after stroke rehabilitation. The change score of an individual patient and a stroke group exceeding these thresholds indicate a true change and a clinically important change, respectively. Thus, the SIS has been proven to be a reliable evaluation tool, able to indicate relevant degrees of changes during stroke rehabilitation and it can differentiate patients with varying degrees of stroke severity (Duncan, Wallace, Lai, Johnson, Embretson & Laster, 1999). Nevertheless, there is a scarcity of literature on the effects of aquatic exercises and their possible effects on the quality of life of the individuals’ post-stroke. The purpose of this case series was to describe changes associated with an intervention involving 8 weeks of aquatic exercises in four individuals’ post-stroke by using the SIS.
Methods
Participants
All participants were recruited from the Aquatic Physical Therapy Center “Prof. Paulo A. Seibert” of the University Hospital –Londrina, Brazil. Individuals post-stroke were eligible to participate if they did not present with cognitive impairments. The exclusion criteria included severe cardiac disease, uncontrolled diabetes, arterial hypertension, and a history of other neurological diseases. Individuals currently participating in a self-directed or formal group exercise program were also excluded. Four subjects were screened for eligibility. All participants were informed about the procedures and signed the terms of informed consent approved by the Institutional Review Board (#17138413.1.0000.5231). This study followed the CARE guidelines for case reports (Riley et al., 2017).
Participant 1, 76 years old, male, 11 years after a right-sided cerebrovascular accident (CVA), left side (non-dominant) sensorimotor deficits. The patient had a history of hypertension and type II diabetes. He used a walking stick for household ambulation and out in the community. Participant 2, 67 years old, male, 17 years after a left-sided CVA, right side (dominant) sensorimotor deficits. The patient displayed Broca aphasia, so his wife provided the subjective information regarding his medical history and his current degree of functioning; in addition, he had a history of hypertension and chronic kidney disease. He used furniture for support in household ambulation and a standard wheelchair when out in the community.
Participant 3, 59 years old, male, 2 years after a left-sided CVA, right side (dominant) sensorimotor deficits. The patient had a history of hypertension and displayed a mild degree of Broca aphasia, but he was able to talk. For household ambulation and out in the community he did not need any assistance device for independent gait. Participant 4, 47 years old, male, 2 years after a right-sided CVA, left side (non-dominant) sensorimotor deficits. The patient had a history of hypercholesterolemia and obesity. He used furniture for support in household ambulation and the support of a caregiver when out in the community.
Outcome measures
Baseline and post-intervention measures were performed for all participants. The SIS version 3.0 (Duncan et al., 2003), a stroke-specific questionnaire, was used as the primary outcome to assess the patient’s health status. The questionnaire consists of 8 domains: strength (4 items), hand function (5 items), activities of daily living/instrumental activities of daily living (ADL/IADL) (10 items), mobility (9 items), communication (7 items), emotion (9 items), memory and thinking (7 items), and participation/role function (8 items). The domains strength, hand function, mobility, and ADL/IADL comprised the physical domain. Each item is rated on a 5-point Likert scale regarding the difficulty the patient experiences in performing each activity. Each domain score has a range of 0 to 100 and is computed using the following equation: Score = [(Mean–1)/(5–1)]×100. The score corresponding to each domain was calculated as the mean of the item scores within that domain (Duncan, Bode, Lai & Perera, 2003; Carod-Artal, Coral, Trizotto & Moreira, 2008). A higher score for an item indicates a better health status. The SIS also includes a question to assess what degree the patient perceived their overall recovery from the stroke, with 0 indicating no recovery and 100 indicating full recovery (Lin et al., 2010).
Besides measuring performance using the SIS, as recommended by Lin et al. (2010), the MDC (Minimal Detectable Change) and CID (Clinically Important Difference) of the physical domains of the SIS were used to evaluate the proportional change in patient individual scores after the stroke treatment protocol (Table 1). The same assessor performed pre- and post-intervention assessments for each participant and was not involved in the aquatic exercises program.
The MDC and CID of the Stroke Impact Scale Subscales
The MDC and CID of the Stroke Impact Scale Subscales
MDC, Minimal Detectable Change; CID, Clinically Important Difference. Lin et al. (2010).
Exclusive aquatic exercises were performed for 8-week (50 minutes per session, two sessions per week) in a heated swimming pool measuring 15 m long×13 m wide, depth 1.2 m deep, extent of submersion around 1.2 m, and a water temperature of 32°C. Each session started with 10 minutes of warm-up using lateral, frontal, and back water-walking, followed by 30 minutes of general exercises of ascending and descending a submerged step, trunk rotation in a standing position, bipedal underwater squatting, switching between underwater sitting and standing, applying the Halliwick Concept (transversal and longitudinal rotation control), making trunk patterns with the Bad Ragaz Ring Method (lateral trunk flexion, rotation with trunk in flexion, and rotation with trunk in extension), and expiratory training (Park, Lee, Lee & Lee, 2019; Cha, Shin & Kim, 2017; Chan et al., 2017; Zhang et al., 2016; Montagna, Santos, Battistuzzo & Loureiro, 2014). Each exercise was performed for 10 repetitions, with 20–40 seconds of rest after each set. A cool-down of 10 minutes was then performed using passive mobilization of the scapula and mobilization and passive stretching of the paretic lower and upper limb. All treatment sessions were carried out on an individual basis. Exercise workloads in these programs were designed with graded increments according to the capability of each participant. Licensed physical therapists conducted the treatment sessions.
Analysis
Descriptive data (SIS) are shown for each participant, at baseline and post-intervention, as well as the general post-intervention changes illustrated with a figure. In addition, the MDC and CID of the physical domains of the SIS were utilized to assess the proportional change in individual patient scores after the stroke treatment protocol.
Results
Participant 1 presented improvements in the domain’s strength, mobility, memory, communication, and emotion (Table 2). In the mobility domain, he presented a difference of 8.3 points when comparing post-intervention to baseline, achieving the CID. Figure 1 demonstrates that his overall stroke recovery remained at 40%. Participant 2 presented improvements in the domains strength, mobility, memory, and communication. In the strength and mobility domains, he achieved the CID, with differences of 18.8 and 11.1 points respectively, at post-intervention related to baseline. At baseline, his stroke recovery was 6%, reaching 50% post-intervention.
Baseline and Post-intervention Measures of SIS
Baseline and Post-intervention Measures of SIS
B, baseline; P, Post-intervention.
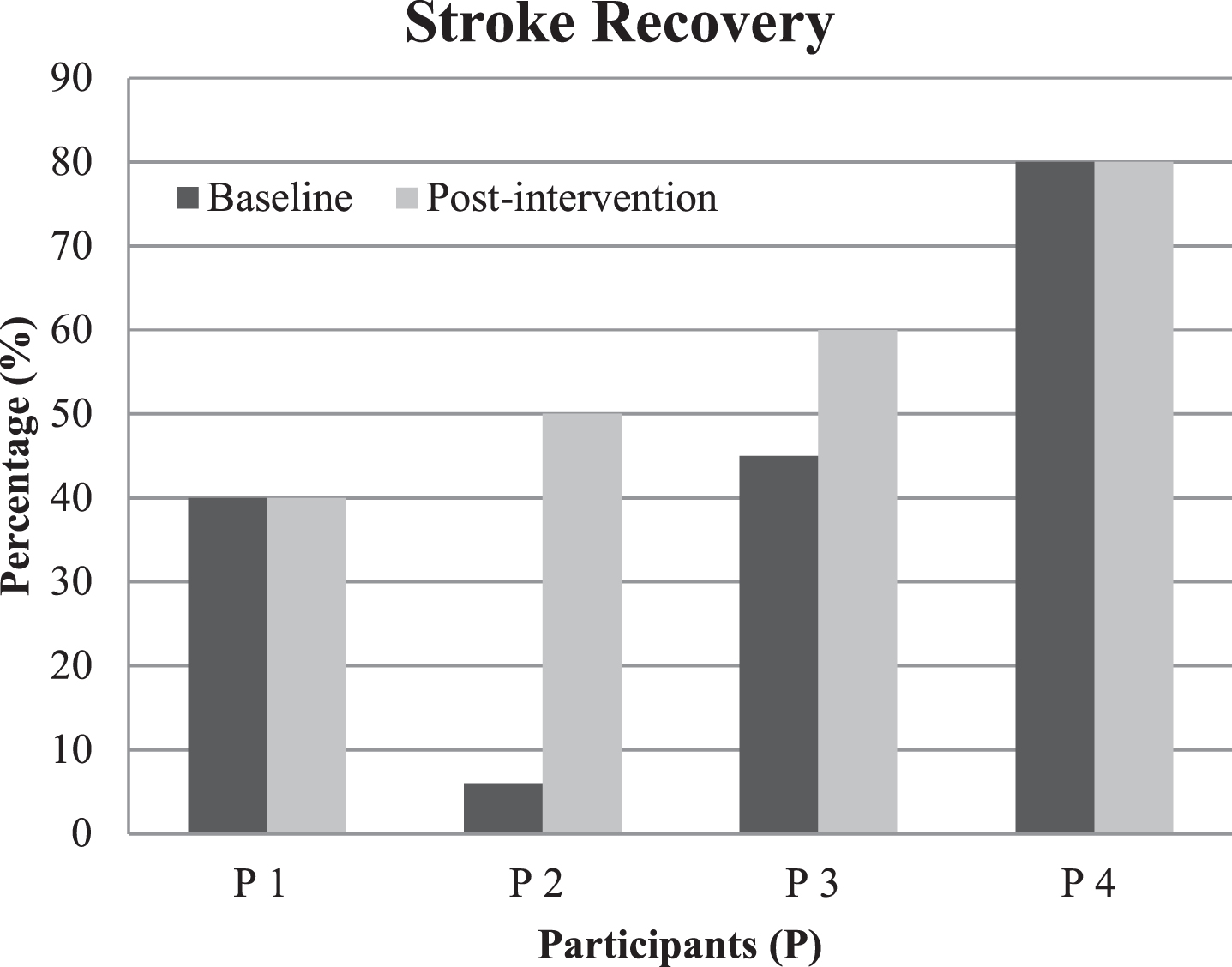
Post-intervention changes in Overall Stroke Recovery using the SIS.
The third participant showed improvement in the domains mobility, ADL/IADL, and emotion. In the mobility domain, he achieved the MDC and CID with differences of 24.6 points from baseline to post-intervention. Regarding the emotion domain, the difference was 7.5 points, reaching the CID. His stroke recovery was 45% at baseline, increasing to 60% post-intervention. The final participant exhibited improvement in all domains except emotion. In the strength domain, the difference from baseline to post-intervention was 15 points, considered a CID. With regard to hand function, mobility, and the ADL/IADL domains, the differences were 32, 21, and 18.5 points, respectively, reaching the MDC and CID. Figure 1 demonstrates that his stroke recovery remained at 80%.
The purpose of this case series was to describe changes associated with an intervention of 8-week aquatic exercises for four individuals post-stroke using the SIS. This is the first study to describe the improvements in the patients’ post-stroke after using this therapy as evaluated by the SIS. The focus on the outcome measure was to highlight the use of a self-report measure that could assess not only mobility, but also other parameters within quality of life. Stroke disabilities affect nearly all quality of life functions; therefore, it is an important index to use when evaluating the effects of stroke rehabilitation (Gray et al., 2007), since it incorporates the effects of motor, sensory, and cognitive function deficits (Lai, Perera, Duncan & Bode, 2003). In this way, the SIS is an appropriate tool to evaluate disability and health-related quality of life after a stroke (Duncan, Wallace, Lai, Johnson, Embretson & Laster, 1999) and can be a viable alternative to be applied in clinical practice.
The results using SIS showed that the participants achieved the CID for the mobility domain, which means the aquatic exercises were considered meaningful and worthwhile by the participants. The mobility component is the category most frequently included in the functional outcome measures for stroke rehabilitation. This emphasis on mobility is understandable because improving mobility is the major goal in the neurological physical therapy field (Chae, Jun, Im, Jang & Park, 2020). All participants in the present study improved in this domain after the exercises, demonstrating that the treatment primarily focused on mobility. Tripp & Krakow (2014) found similar results, with positive effects on functional mobility in subacute stroke patients who performed aquatic compared to land exercises. In the recent systematic review by Saquetto et al. (2019), there was a significant improvement in mobility after applying an intervention using aquatic exercises compared to land exercises, with the results of the intervention evaluated by the Timed up and Go test. In the systematic review by Giuriati, Servadio, Temperoni, Curcio, Valente & Galeoto (2020), their results were also significantly favorable for aquatic exercise compared to exercises on the land during a treatment period of 4- to 6-weeks.
Regarding safety, when mobility is impaired, stroke patients are likely to present an increased risk of falling (Tripp & Krakow, 2014). Aquatic exercises have been reported to improve mobility and decrease the fear of falling (Oh, Lim, Kim, Kim, Song & Yoon, 2014; Devereux, Robertson & Briffa, 2005). Although this study did not investigate the fear of falling, improvements in the mobility of these participants can be associated with a decrease in their fear of falling. This can be explained by the ease of movement (buoyancy) when the exercises are performed in water, plus no consequences of falling in the water, allowing them to focus on improving their mobility, which ultimately decreases their fear of falling (Chan et al., 2017).
Mobility deficits can be induced by impaired muscle strength in individuals who have had a stroke (Zhang et al., 2016). Thus, muscle strength training can be indicated, not only to increase strength, but also to improve functional capability, such as walking and stair climbing (Ada, Dorsch & Canning, 2006). Aquatic exercises can improve leg strength in stroke survivors as observed in participants 2 and 4, who reached the CID post-intervention for the strength domain in the SIS (Zhang et al., 2016; Noh, Lim, Shin & Paik, 2008; Chu, Eng, Dawson, Harris, Ozkaplan & Gylfadóttir, 2004).
It is important to note that the initial baseline values can be decisive and interfere with possible gains. In the systematic review by Nascimento, Flores, Menezes & Teixeira-Salmela (2020), three studies were included in an analysis that showed no improvement in muscle strength after the participants had undergone aquatic exercises. In the systematic review by Giuriati, Servadio, Temperoni, Curcio, Valente & Galeoto (2020) the authors explained that even when the individual results were relatively small for muscle mass gain, the meta-analysis revealed the changes were statistically significant (P = 0.007). This factor may be implicit in our study due to the low number of participants (error type II), which is justified by it being a series of case reports. In addition, to fully evaluate motor function, other scales such as the Fugl-Meyer Upper and Lower Extremity scale, which has stronger evidence for validity than the SIS, are recommended for use as primary outcomes in interventions targeting motor function in chronic stroke populations (Bushnell et al., 2015).
Regarding the ADL/IADL domains, participant 4 showed differences that reached the MDC and CID. This enhancement in ADL could be the result of improvements in movement requiring only a small amount of force due to the assistance of the water buoyancy, consequently decreasing the effects of gravity as well as reducing the burden on the muscles and joints (Kim, Lee & Kim, 2015; Verhagen, Cardoso JR & Bierma-Zeinstra, 2012). To promote functional recovery, the paretic side can be spontaneously enabled, thus enhancing the ability to perform ADLs and improving functional independence (Sato, Kaneda, Wakabayashi & Nomura, 2009).
The SIS includes a question regarding overall recovery from stroke (Lin et al., 2010). Two participantsmaintained their overall stroke recovery at the same level as at baseline (participant 1:40% and participant 4:80%) after the treatment. Participant 2 increased his stroke recovery by 44% (baseline = 6%, post-intervention = 50%) and participant 3, 15% (baseline = 45%, post-intervention = 60%). These improvements could be associated with the previously mentioned functional benefits offered by the water treatment and the SIS capacity to evaluate some aspects of the recovery process after stroke, such as: ADL, IADL, mental health, dysphasia, mobility, walking, and social functioning related to patient quality of life (Lai, Studenski, Duncan & Perera, 2002). Aidar, Silva, Reis, Carneiro & Carneiro-Cotta, (2007) also evaluated the effects of aquatic exercises on the quality of life in stroke patients, and their results showed improvements; however, they applied the SF-36 questionnaire in an abbreviated form. Recent clinical trials and systematic reviews have also assessed the quality of life by SF-36, SF-8, and State-Trait Anxiety Inventory (Saquetto et al., 2019; De la Cruz, 2020). However, none of these questionnaires are specific to stroke. The importance of tests to be specific is due to the fact that the tests have to be sensitive enough to identify changes in the patient’s specific condition.
Although favorable outcomes were reported in our study, its case series design prevents us from drawing robust conclusions about the impact of aquatic exercises on improvements in the SIS results. The inherent design of any case series creates a selection bias, which must be taken into consideration when reviewing the outcomes. Therefore, this type of study is well established in the literature, where pertinent data about real-life are shared. This represents a valuable research and educational resource and contributes to illustrating elements of patient management. The authors acknowledge that some results in each SIS domain may have been influenced by factors related to their emotional state or other events in the lives of the participants at the moment of data collection. In addition, applying other specific measures, such as physical function, could contribute to a better understanding of the clinical framework of each participant. In addition, the scores used for the CID proposed by Lin et al. (2010) are recommended for clinical trials, not individual patients. Larger studies with a control group are needed to confirm and clarify these outcomes to allow for investigations into the causal relationship between aquatic exercise and improvements in the SIS measures. Future research should also compare whether aquatic exercises are more effective than other forms of exercise in individuals’ post-stroke by using the SIS evaluation.
Footnotes
Acknowledgments
The authors would like to thank Prof. Sônia M. F. Luiz, PT, PhD and the University Hospital at Universidade Estadual de Londrina for its administrative assistance of the Aquatic Physical Therapy Center “Prof. Paulo A. Seibert”. The last author also wishes to express his thanks to CNPq (National Council for Scientific and Technological Development - Brazil) for the productivity scholarship.
Conflict of interest
None declared.